The International Sensitivity Index (ISI) is a calibration value assigned to every thromboplastin reagent used in PT testing. It is the number that allows laboratories worldwide to convert their raw PT ratios into a standardised INR — making coagulation results comparable across institutions, countries, and reagent manufacturers.
Without ISI, PT results would be laboratory-specific and clinically incomparable. Understanding what ISI is and how it works clarifies why the INR formula is designed the way it is, and why reagent quality matters in anticoagulation monitoring.
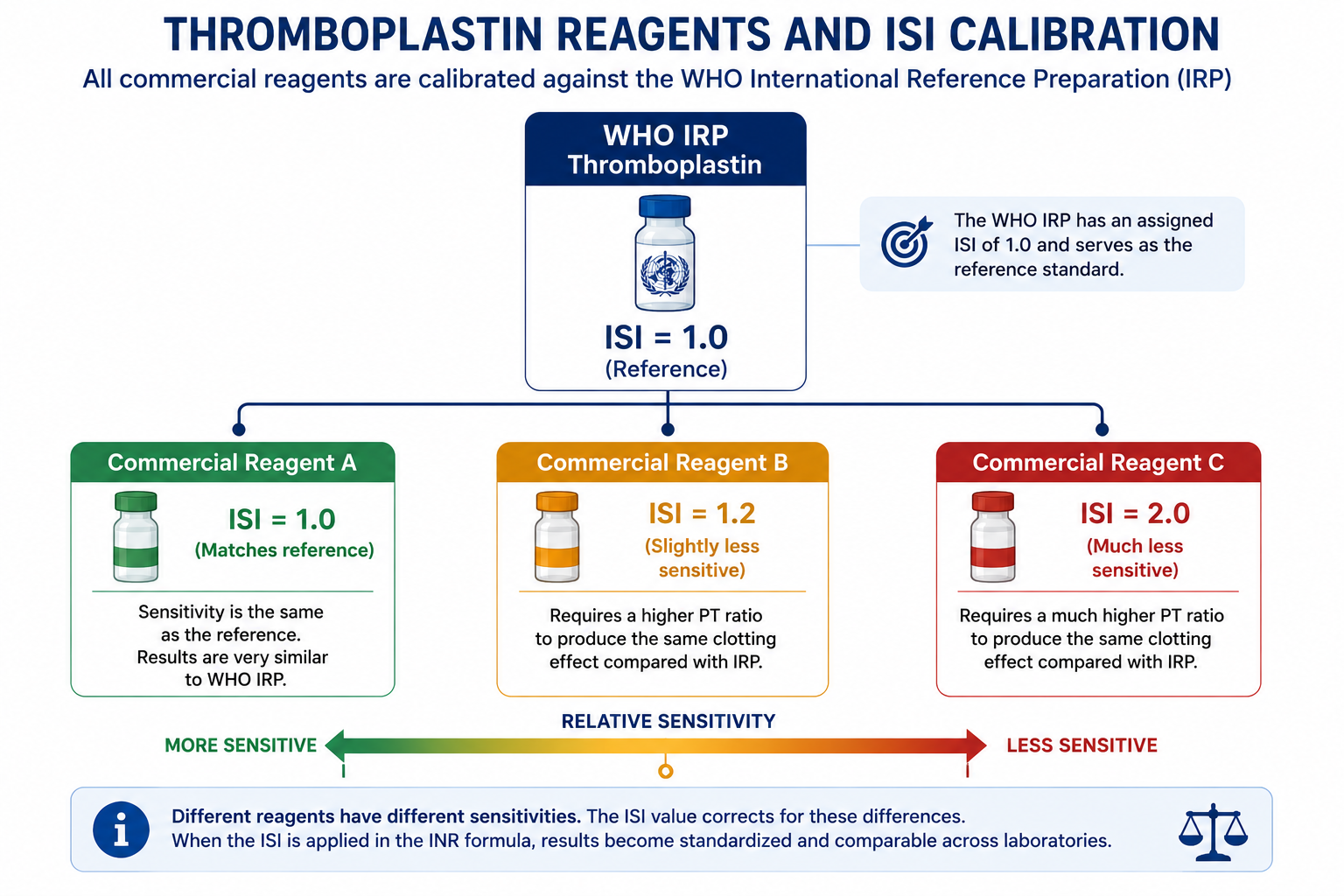
ISI tells us how sensitive a thromboplastin reagent is compared with the WHO reference. A value close to 1.0 means the reagent behaves like the reference. A higher value means the reagent is less sensitive and needs greater correction when calculating INR.
Learning Objectives
- Define the International Sensitivity Index (ISI)
- Explain why different thromboplastin reagents produce different PT values
- Describe how ISI is determined by calibration against the WHO reference
- Compare the clinical implications of low ISI versus high ISI reagents
- Explain how ISI corrects for reagent differences in the INR formula
What is the ISI?
The International Sensitivity Index (ISI) is a dimensionless calibration constant that expresses the sensitivity of a thromboplastin reagent to reductions in the vitamin K-dependent clotting factors (Factors II, VII, and X), relative to the WHO International Reference Preparation (IRP).
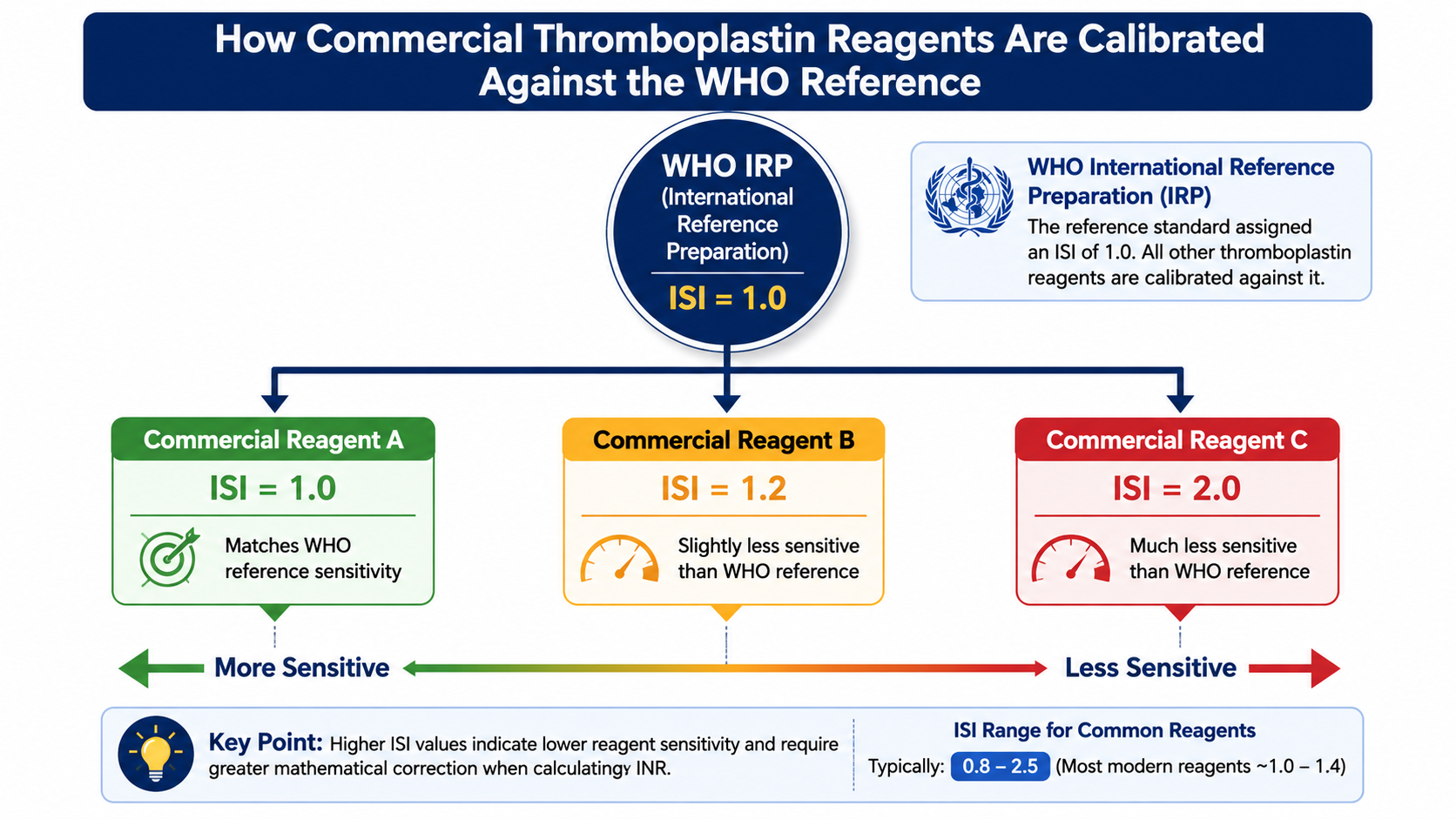
The WHO IRP is a globally standardised thromboplastin preparation maintained in Geneva. By definition, it has an ISI of exactly 1.0. Every commercial reagent is calibrated against this reference, and the result of that calibration is the ISI value stamped on the reagent package insert.
Why Thromboplastin Reagents Differ
Thromboplastin (tissue factor + phospholipid) is the key reagent added to plasma to initiate the PT test. Historically, thromboplastin was extracted from a variety of biological sources including human brain, rabbit brain, and bovine lung. Today, most commercial preparations use recombinant tissue factor with synthetic or natural phospholipid.
These differences in source, extraction method, tissue factor concentration, and phospholipid composition mean that different reagents have different intrinsic sensitivities to reductions in vitamin K-dependent clotting factor levels. A highly sensitive reagent detects small changes in Factor VII or Factor X activity and reports a larger PT prolongation. A less sensitive reagent requires a more marked factor reduction before it registers the same PT change.
This is the fundamental problem: a patient with therapeutic warfarin anticoagulation might produce a PT ratio of 2.0 using one reagent and only 1.4 using another — not because their coagulation status changed, but purely because the reagents respond differently to the same degree of factor depletion.
How ISI is Determined
ISI is determined by the reagent manufacturer through a formal calibration procedure as follows:
- A set of fresh plasma samples is collected from 60 patients on stable long-term warfarin therapy and 20 healthy volunteers.
- All samples are tested using both the test reagent (the one being calibrated) and the WHO International Reference Preparation.
- The log(PT with test reagent) is plotted against log(PT with WHO reference) for all samples. This produces an orthogonal regression line on a log-log plot.
- The slope of this regression line is the ISI for that reagent.
PT values follow a log-normal distribution in anticoagulated patients, and the relationship between PT values from two different reagents is most linear when plotted on a log-log scale. This statistical approach gives the most unbiased estimate of the ISI slope and ensures the formula's exponent correctly standardises results across the full therapeutic range.
A reagent whose log-log slope equals 1.0 behaves identically to the WHO reference — it gets an ISI of 1.0. A reagent that is less sensitive (produces a smaller PT ratio for the same patient) has a log-log slope > 1.0 and receives an ISI > 1.0. A more sensitive reagent receives an ISI < 1.0 (rare in practice).
Because ISI is derived from a log-log calibration relationship, the mathematical correction is applied as an exponent rather than a simple multiplier. This is why the INR formula raises the PT ratio to the power of the ISI. In practical terms: INR is not PT ratio × ISI — it is PT ratioISI. For the full calculation walkthrough, see How INR Is Calculated.
Low ISI vs High ISI
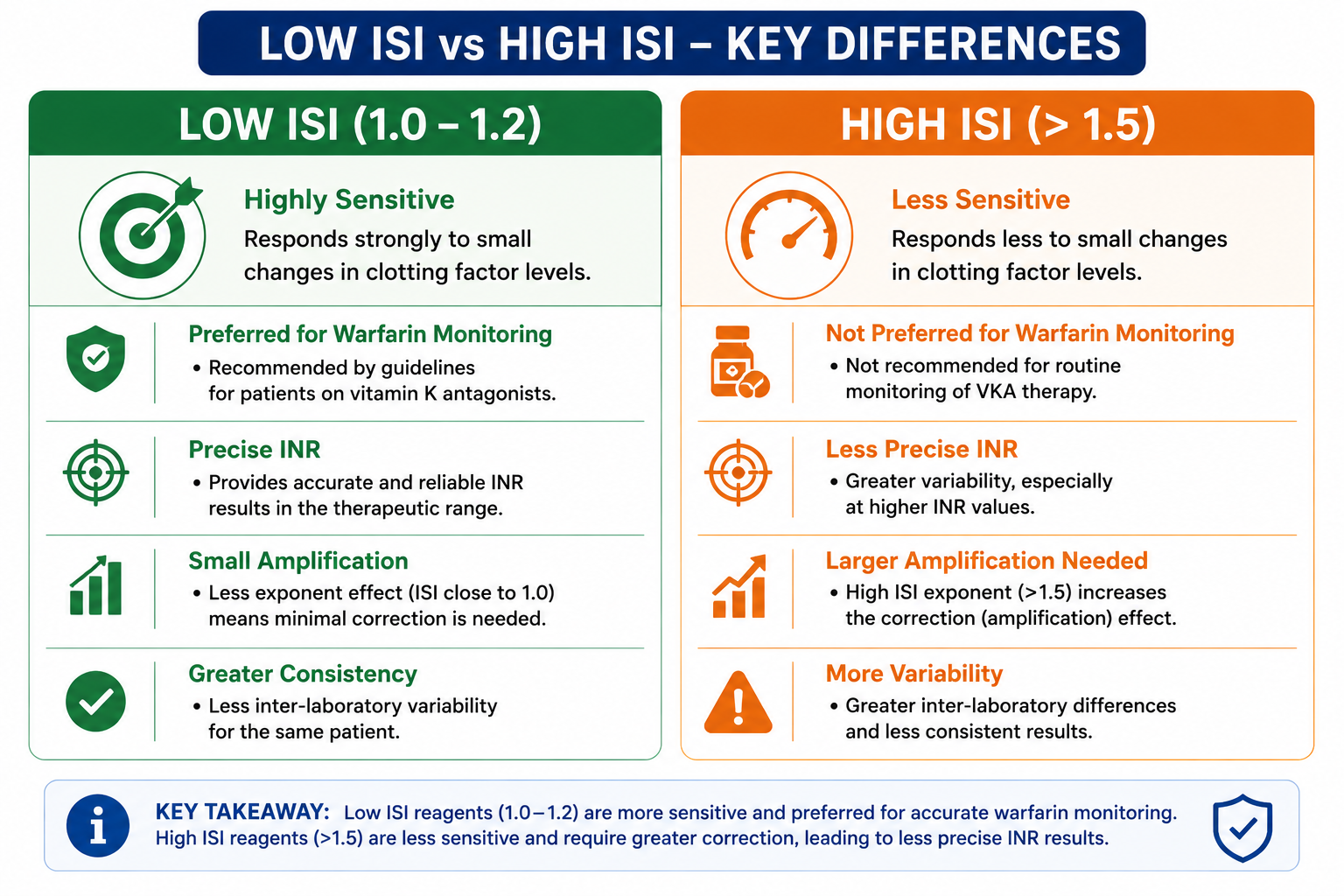
- Highly sensitive to clotting factor changes
- Close to the WHO reference reagent behaviour
- Produces larger raw PT ratios for same patient
- Less mathematical amplification needed
- More precise INR — less amplification of measurement error
- Preferred for warfarin monitoring
- Less sensitive to clotting factor changes
- Diverges more from WHO reference behaviour
- Produces smaller raw PT ratios for same patient
- Larger exponent amplification required
- INR less precise — amplifies measurement variability
- Not preferred; associated with wider INR confidence intervals
Most modern recombinant thromboplastin reagents have ISI values in the range of 0.9–1.3, which is considered optimal for warfarin monitoring. Older rabbit brain thromboplastin preparations were much less sensitive (ISI up to 2.0+), which is one reason early warfarin monitoring was unreliable before ISI calibration was introduced.
Effect of ISI on INR
The ISI determines how much the PT ratio is mathematically amplified before reporting. Consider the same patient tested at two laboratories:
| Parameter | Lab A (ISI = 1.0) | Lab B (ISI = 2.0) |
|---|---|---|
| Patient's actual coagulation status | Identical — same patient, same blood draw | |
| PTpatient | 24 s | 17 s |
| PTmean normal | 12 s | 12 s |
| PT ratio | 2.0 | 1.42 |
| ISI exponent applied | 2.01.0 | 1.422.0 |
| Reported INR | 2.0 | 2.0 |
Despite producing very different raw PT values (24 s vs 17 s) and different PT ratios (2.0 vs 1.42), both laboratories report the same INR of 2.0. The ISI exponent is what makes this possible. The clinician receives a single standardised number that is independent of which reagent was used.
Clinical Relevance of ISI
From a clinician's perspective, the ISI is handled entirely by the laboratory — it is embedded in the instrument software and applied automatically to every result. The clinician receives only the INR. However, understanding ISI matters in several contexts. INR is used in warfarin monitoring, pre-operative assessment, and liver disease severity scoring systems such as Child-Pugh and MELD. For broader interpretation of PT and INR results, see PT and INR Explained.
1. Point-of-Care INR Testing
POC INR devices (e.g. CoaguChek, Roche) use disposable reagent cartridges with embedded calibration. The ISI for the cartridge is used by the device's algorithm to convert the measured optical or electrochemical signal into a PT and then an INR. Not all POC devices are equally well-calibrated — clinicians and anticoagulation nurses should be aware that POC and laboratory INRs can occasionally diverge, particularly at very high or low INR values.
2. Inter-Laboratory Discrepancies
A patient who checks their INR at one hospital and then at another may occasionally receive slightly different results even with correct technique. While both results are standardised via ISI, residual imprecision (analytical variation, ISI calibration error, sample handling differences) means INRs from two labs are rarely perfectly identical. Results within 0.2–0.3 INR units of each other are generally consistent; larger discrepancies warrant investigation.
3. Reagent Change in a Laboratory
When a laboratory switches thromboplastin reagent manufacturer, they must establish the new reagent's ISI and PT mean normal before reporting results. Clinicians and anticoagulation services should be notified, as a reagent change can sometimes cause a systematic shift in reported INR values even if patient coagulation status is unchanged.
Laboratory Considerations
Laboratories performing PT/INR testing must meet several quality requirements related to ISI:
- Modern laboratories generally prefer thromboplastin reagents with low ISI values, typically around 1.0–1.4, because they provide more precise INR measurements with less mathematical amplification of measurement error.
- Establish local PT mean normal using at least 20 healthy, non-anticoagulated adult donors — the geometric mean is used.
- Participate in external quality assurance (EQA) programmes to detect systematic INR errors across the laboratory network.
- Recalibrate after each new reagent lot because ISI can vary slightly between manufacturing batches even from the same supplier.
- Verify ISI on the instrument — some instrument-reagent combinations require local ISI calibration in addition to the manufacturer-assigned value.
Exam Tips
- WHO IRP ISI = 1.0 — this is the anchor of the whole calibration system.
- ISI = slope of log(PT test reagent) vs log(PT WHO reference) on a log-log regression plot.
- Low ISI = more sensitive reagent = better precision for warfarin monitoring.
- High ISI = less sensitive reagent — needs larger exponent to compensate, which amplifies measurement error.
- ISI is the exponent in the INR formula — when ISI = 1.0, INR = PT ratio (they coincide).
- Clinicians do not interact with ISI directly — the lab applies it automatically. The clinician receives only the final INR.
- For exam purposes: understand the concept of ISI and its role in standardisation, not the detailed statistical procedure for determining it.
Frequently Asked Questions
Key Takeaways
- ISI is a calibration constant expressing a thromboplastin reagent's sensitivity relative to the WHO IRP (ISI = 1.0)
- It is determined as the slope of the log-log regression of test reagent PT vs WHO reference PT, using samples from stable warfarin patients and healthy controls
- ISI is the exponent in the INR formula because it is derived from a log-log calibration slope — exponentiation, not multiplication, is the correct correction
- Low ISI (≤ 1.2): highly sensitive reagent, preferred for warfarin monitoring, more precise INR
- High ISI (> 1.5): less sensitive reagent, requires greater amplification, produces less precise INR
- Clinicians do not handle ISI — it is applied by the laboratory automatically before reporting INR
- Reagent changes in a laboratory may shift reported INR values — anticoagulation services must be notified
References
- WHO Expert Committee on Biological Standardization. Guidelines for thromboplastins and plasma used to control oral anticoagulant therapy. WHO Technical Report Series No. 889. Geneva: WHO; 1999.
- van den Besselaar AMHP, Witteveen E, Meeuwisse-Braun J. Influence of thromboplastin source on ISI and INR values in patients on stable oral anticoagulant treatment. J Thromb Haemost. 2001;86(4):565–570.
- Poller L, et al. A multicentre calibration of laboratory INR: a pilot study. Br J Haematol. 1998;101(3):476–481.
- Horsti J, Uppa H, Vilpo JA. Poor agreement among prothrombin time international normalized ratio methods. Clin Chem. 2005;51(3):553–560.
- Kitchen S, et al. BCSH guidelines for the use of near-patient testing for haemostasis. Br J Haematol. 2006;135(2):257–265.
- World Health Organization Expert Committee on Biological Standardization. Requirements for thromboplastins and plasma used to control oral anticoagulant therapy. WHO Technical Report Series. Geneva: WHO.
This article is intended for medical education only. It does not constitute clinical advice. Always refer to current local guidelines and specialist input for clinical decision-making regarding coagulation testing.