APTT (Activated Partial Thromboplastin Time) is one of the most commonly requested coagulation tests in clinical practice. It is used to investigate bleeding disorders, identify coagulation factor deficiencies, detect inhibitors, and monitor unfractionated heparin therapy.
Unlike PT, which primarily evaluates the extrinsic pathway, APTT evaluates the intrinsic and common coagulation pathways. Understanding what APTT measures and why it becomes prolonged is essential for interpreting coagulation profiles and diagnosing disorders such as haemophilia, lupus anticoagulant syndrome, and disseminated intravascular coagulation (DIC).
Read this article alongside PT and INR Explained — together they cover the two fundamental coagulation tests used in routine clinical practice.
APTT stands for Activated Partial Thromboplastin Time. It measures the time required for plasma to clot after activation of the intrinsic coagulation pathway. APTT primarily assesses intrinsic pathway factors and common pathway factors. A prolonged APTT suggests deficiency, inhibition, or dysfunction of one or more factors within these pathways.
Learning Objectives
- Explain what APTT measures and which coagulation pathway it tests
- Identify which coagulation factors affect APTT
- Differentiate PT from APTT in terms of pathway, factors, and clinical use
- Recognise common causes of prolonged APTT and group them by mechanism
- Interpret an isolated prolonged APTT (normal PT, prolonged APTT)
- Understand the principle of mixing studies and interpret their results
- Explain why APTT is used to monitor unfractionated heparin
What Does APTT Measure?
APTT is performed by adding an activating agent (such as kaolin, celite, or ellagic acid) and a partial thromboplastin (phospholipid without tissue factor) to citrated plasma, then adding calcium and measuring the time to clot formation.
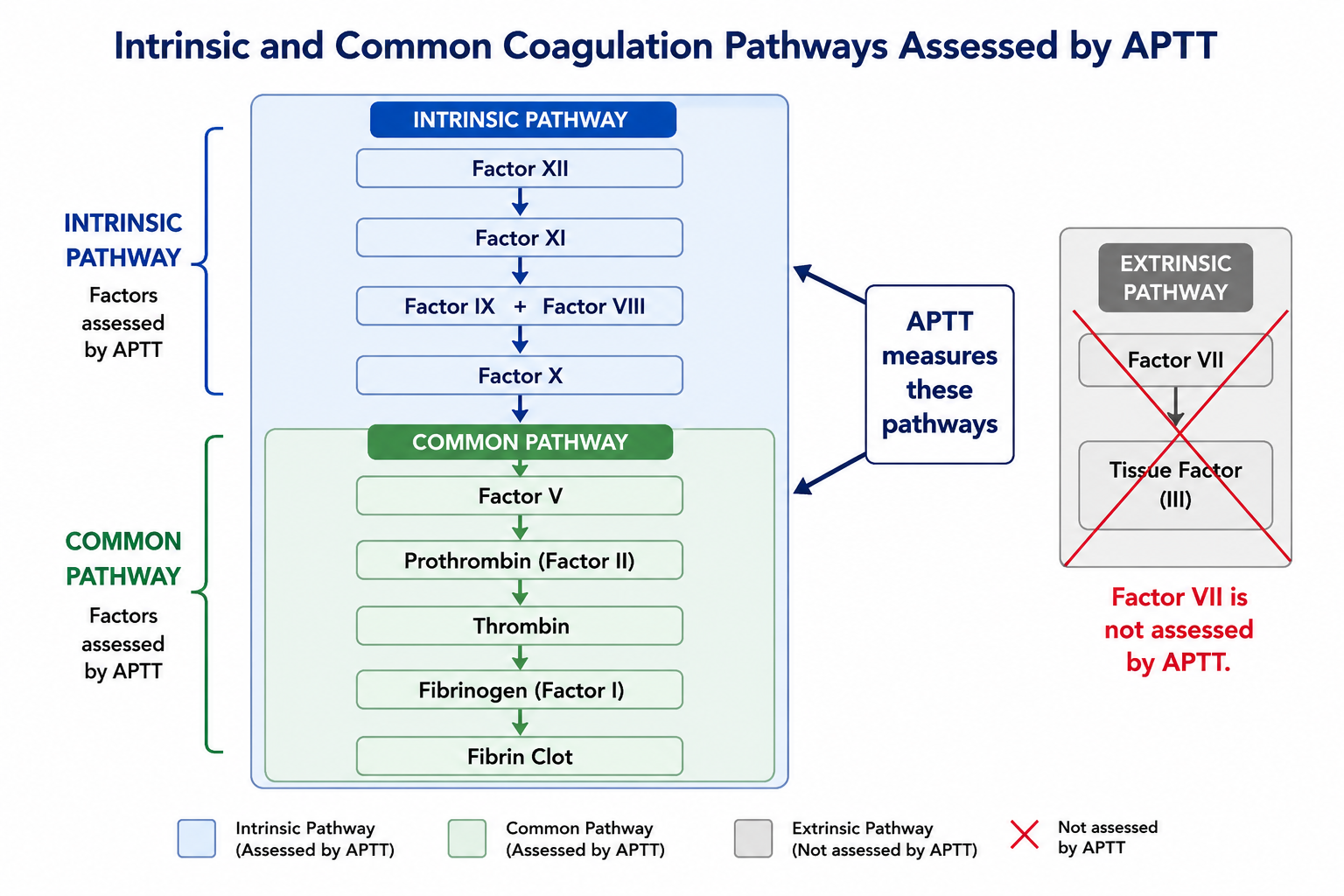
The absence of tissue factor means the extrinsic pathway is not triggered. APTT therefore selectively evaluates the intrinsic pathway (contact activation) and the subsequent common pathway, which both converge to generate thrombin and form a fibrin clot.
Factors assessed by APTT include: XII, XI, IX, VIII (intrinsic pathway) and X, V, II (prothrombin), I (fibrinogen) (common pathway).
Unlike PT, Factor VII does not significantly affect APTT — it is exclusive to the extrinsic pathway. This is the key structural difference between the two tests.
Normal APTT is approximately 25–38 seconds, though the exact reference range varies between laboratories depending on the reagent and analyser used. A prolonged APTT means clotting is taking longer than expected, indicating a deficiency, inhibitor, or anticoagulant effect within the intrinsic or common pathway. Reference ranges vary between laboratories and should always be interpreted using the range printed on the local laboratory report.
Which Coagulation Factors Affect APTT?
Deficiency of any of the following factors will prolong APTT:
| Factor | Name | Pathway | Effect on APTT if Deficient | Clinical Note |
|---|---|---|---|---|
| XII | Hageman factor | Intrinsic | Prolonged (often markedly) | No clinical bleeding despite prolonged APTT |
| XI | Plasma thromboplastin antecedent | Intrinsic | Prolonged | Variable bleeding — severity unpredictable from APTT level |
| IX | Christmas factor | Intrinsic | Prolonged | Deficiency causes Haemophilia B |
| VIII | Antihemophilic factor | Intrinsic | Prolonged | Deficiency causes Haemophilia A — most common severe inherited coagulopathy |
| X | Stuart factor | Common | Prolonged | Also prolongs PT |
| V | Labile factor | Common | Prolonged | Also prolongs PT; not vitamin K dependent |
| II | Prothrombin | Common | Prolonged | Also prolongs PT; vitamin K dependent |
| I | Fibrinogen | Common | Prolonged | Also prolongs PT; severe hypofibrinogenaemia or dysfibrinogenaemia |
- Factor VIII deficiency → Haemophilia A — most common severe inherited bleeding disorder; X-linked recessive
- Factor IX deficiency → Haemophilia B — clinically indistinguishable from Haemophilia A without factor assay; X-linked recessive
- Factor XI deficiency — may cause bleeding of variable and often unpredictable severity
- Factor XII deficiency — markedly prolongs APTT in the laboratory but does not cause clinical bleeding (contact activation is not required for in vivo haemostasis)
Haemophilia A vs Haemophilia B
Haemophilia A and Haemophilia B are clinically similar inherited bleeding disorders. Both typically cause isolated prolonged APTT with normal PT, because Factors VIII and IX belong to the intrinsic pathway. Both are X-linked recessive, predominantly affecting males, and present with deep tissue bleeding, haemarthrosis, and muscle haematomas.
| Feature | Haemophilia A | Haemophilia B |
|---|---|---|
| Deficient factor | Factor VIII | Factor IX |
| Alternative name | Classical haemophilia | Christmas disease |
| Frequency | More common (~1 in 5,000 males) | Less common (~1 in 30,000 males) |
| Inheritance | X-linked recessive | X-linked recessive |
| PT | Normal | Normal |
| APTT | Prolonged | Prolonged |
| Platelet count | Normal | Normal |
| Clinical features | Deep tissue bleeding, haemarthrosis, muscle haematoma | Clinically similar to Haemophilia A |
| Confirmation | Factor VIII assay | Factor IX assay |
APTT cannot distinguish Haemophilia A from Haemophilia B — the result is prolonged in both. Specific factor assays are required to identify which factor is reduced and to quantify severity. A haemophilia APTT result needs factor VIII and IX levels to reach a diagnosis.
APTT vs PT
PT and APTT are complementary tests that together allow localisation of a coagulation defect to the intrinsic, extrinsic, or common pathway. Used in combination, they provide far more diagnostic information than either alone.
| Feature | APTT | PT / INR |
|---|---|---|
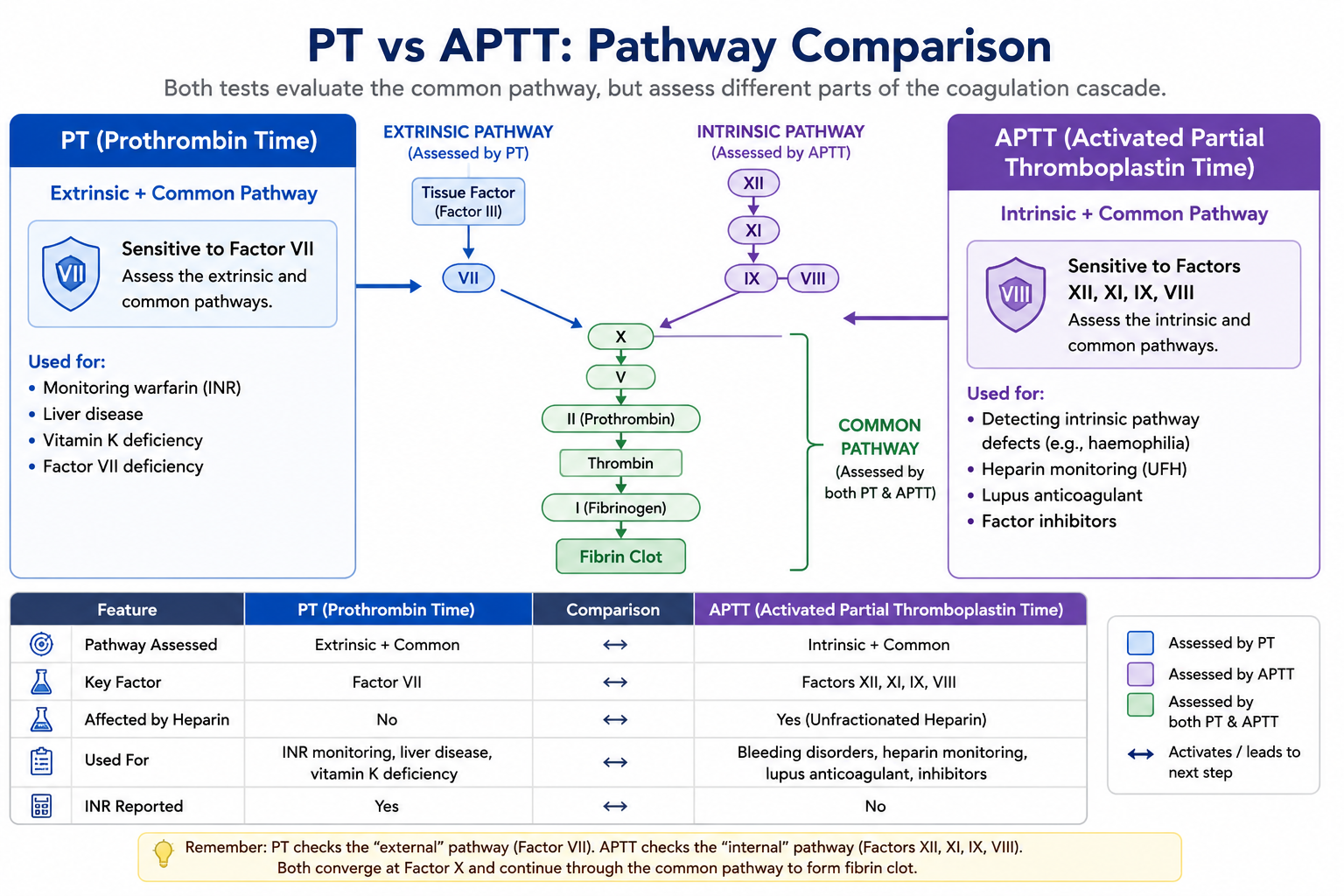
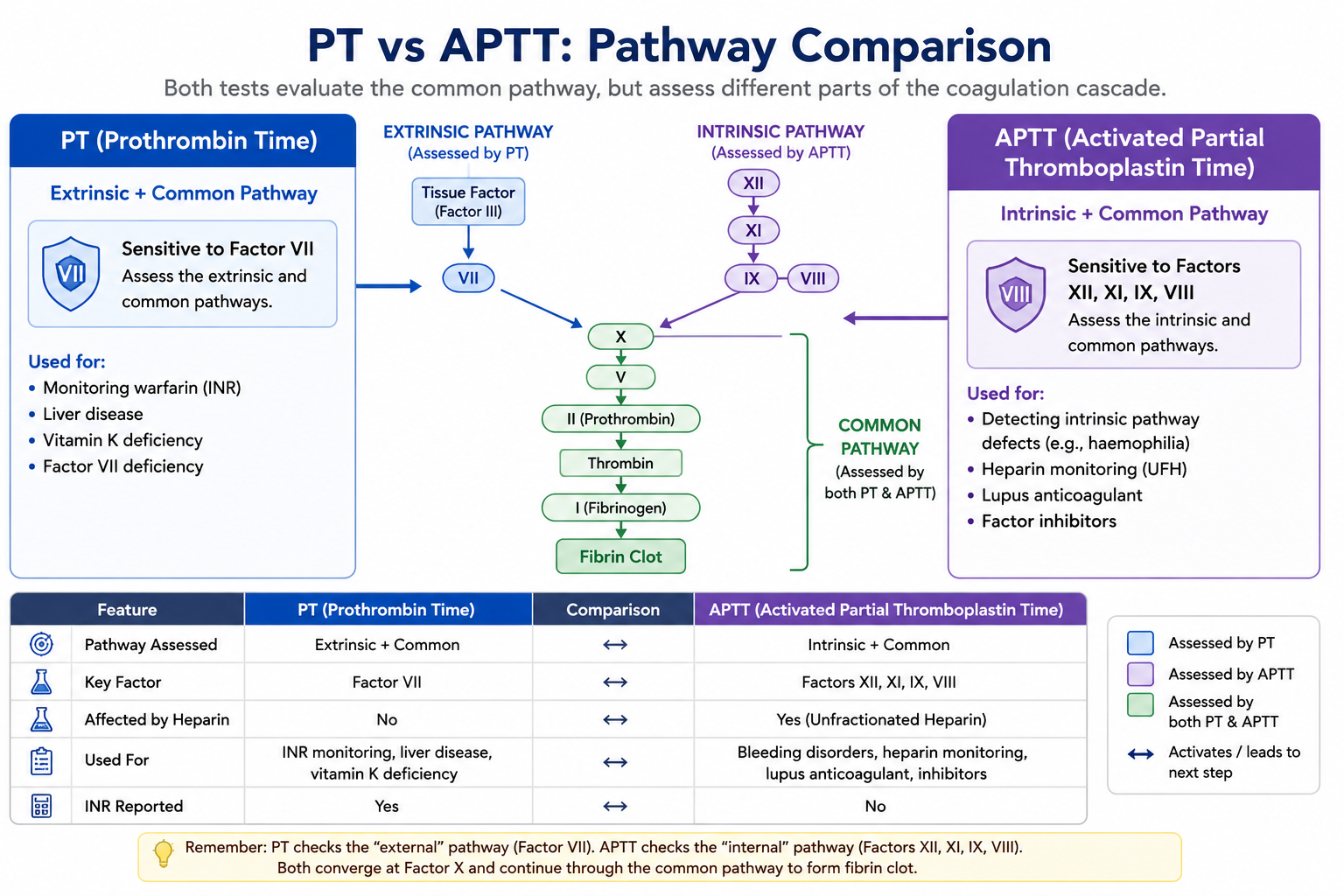
| Pathway tested | Intrinsic + Common | Extrinsic + Common |
| Key factors | XII, XI, IX, VIII, X, V, II, I | VII, X, V, II, I |
| Factor VII | Not assessed | Primary extrinsic factor |
| Factors VIII, IX, XI, XII | Assessed | Not assessed |
| Used to monitor warfarin | No | Yes (via INR) |
| Used to monitor heparin (UFH) | Yes | No |
| Standardised between labs | No (no equivalent of ISI) | Yes (via ISI → INR) |
| Prolonged in haemophilia | Yes | No (if Factor VIII/IX only affected) |
PT = Extrinsic + Common pathway — key factor is Factor VII.
APTT = Intrinsic + Common pathway — key factors are VIII, IX, XI, XII.
Both tests assess the common pathway (Factors X, V, II, I). An abnormality confined to the common pathway prolongs both PT and APTT.
Localising Coagulation Defects Using PT and APTT
PT and APTT are most useful when interpreted together. The pattern of abnormality helps localise the likely site of the coagulation problem before more detailed factor assays are requested.
| PT | APTT | Likely Location | Common Causes |
|---|---|---|---|
| Normal | Normal | No major defect in measured pathways | Does not exclude platelet disorders, von Willebrand disease, Factor XIII deficiency, or mild factor deficiency |
| Normal | Prolonged | Intrinsic pathway | Haemophilia A, Haemophilia B, Factor XI deficiency, Factor XII deficiency, lupus anticoagulant, heparin contamination |
| Prolonged | Normal | Extrinsic pathway | Factor VII deficiency, early warfarin effect, early vitamin K deficiency, early liver disease |
| Prolonged | Prolonged | Common pathway or multiple factor deficiency | DIC, severe liver disease, massive transfusion, severe vitamin K deficiency, supratherapeutic anticoagulation, Factor X/V/II/I deficiency |
A normal PT with prolonged APTT points toward the intrinsic pathway, especially Factors VIII, IX, XI, and XII. A prolonged PT with normal APTT points toward the extrinsic pathway, especially Factor VII. Prolongation of both PT and APTT suggests a common pathway problem or a systemic process affecting multiple clotting factors such as DIC or severe liver disease.
Normal PT + prolonged APTT = intrinsic pathway problem.
Prolonged PT + normal APTT = extrinsic pathway problem.
Both prolonged = common pathway or multiple factor problem.
Causes of Prolonged APTT
A prolonged APTT indicates slower-than-normal clotting via the intrinsic or common pathway. Causes are grouped by mechanism:
1. Factor Deficiencies (Inherited)
- Haemophilia A — Factor VIII deficiency; most common severe inherited bleeding disorder
- Haemophilia B — Factor IX deficiency; clinically similar to Haemophilia A
- Factor XI deficiency — Ashkenazi Jewish population overrepresented; bleeding severity unpredictable
- Factor XII deficiency — prolonged APTT without clinical bleeding
2. Anticoagulants
- Unfractionated heparin (UFH) — enhances antithrombin activity, inhibits thrombin (Factor IIa) and Factor Xa; APTT used for monitoring
- Direct thrombin inhibitors (e.g. argatroban, bivalirudin, dabigatran) — inhibit thrombin directly; variably prolong APTT
3. Inhibitors (Acquired)
- Lupus anticoagulant — antiphospholipid antibody that interferes with phospholipid-dependent coagulation in vitro, prolonging APTT; paradoxically associated with thrombosis in vivo, not bleeding
- Acquired Factor VIII inhibitor — autoantibody against Factor VIII; causes acquired haemophilia A; may develop spontaneously, post-partum, or in malignancy
4. Systemic Disorders
- Disseminated intravascular coagulation (DIC) — consumption of multiple clotting factors; both PT and APTT are typically prolonged alongside low fibrinogen and elevated D-dimers
- Severe liver disease — reduced synthesis of Factors I, II, V, IX, X, XI; typically prolongs both PT and APTT
- Massive transfusion / dilutional coagulopathy — dilution of coagulation factors by large volumes of packed red cells or crystalloid
- Vitamin K deficiency — affects Factors II, VII, IX, X; predominantly prolongs PT early, then APTT as deficiency worsens
5. Pre-Analytical Causes
- Sample contamination with heparin — from heparinised flush lines; common cause of unexpectedly prolonged APTT in inpatients
- Underfilled sample tube — excess citrate anticoagulant relative to plasma dilutes clotting factors
Interpreting an Isolated Prolonged APTT
An isolated prolonged APTT — normal PT with prolonged APTT — strongly suggests a problem confined to the intrinsic pathway, since the extrinsic and common pathways (tested by PT) are functioning normally.
| PT | APTT | Likely Cause |
|---|---|---|
| Normal | Prolonged | Haemophilia A/B, Factor XI or XII deficiency, lupus anticoagulant, heparin contamination |
| Prolonged | Normal | Factor VII deficiency, early warfarin effect, early liver disease |
| Prolonged | Prolonged | DIC, severe liver disease, massive transfusion, common pathway deficiency, supratherapeutic anticoagulation |
| Normal | Normal | Does not exclude platelet disorders, von Willebrand disease, or Factor XIII deficiency |
A patient with recurrent venous thrombosis and prolonged APTT may have lupus anticoagulant rather than a bleeding disorder. Lupus anticoagulant prolongs phospholipid-dependent clotting tests in vitro but is associated with thrombosis in vivo. The clinical picture — thrombosis rather than bleeding — is the key diagnostic clue distinguishing lupus anticoagulant from a factor deficiency.
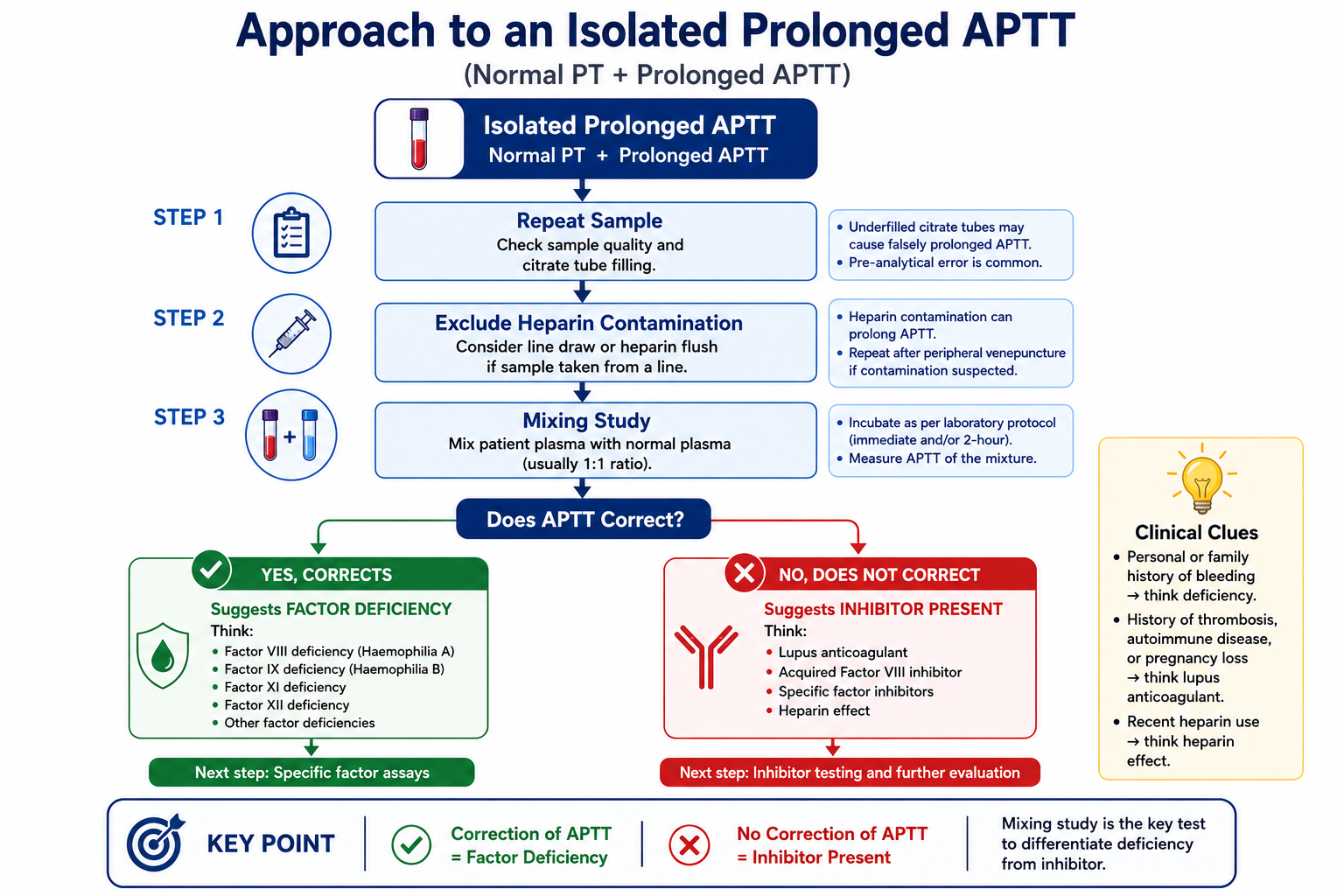
Normal PT with prolonged APTT strongly suggests a problem confined to the intrinsic pathway. The first three diagnoses to consider are Haemophilia A, Haemophilia B, and lupus anticoagulant. Always check for heparin contamination before concluding a clinical cause. A mixing study (see below) is the next diagnostic step.
Mixing Studies Explained
A mixing study is a simple but powerful test used when an unexpectedly prolonged APTT is found. It distinguishes between two fundamentally different causes: a factor deficiency (where clotting factors are simply absent or reduced) and an inhibitor (where an antibody or anticoagulant is actively blocking coagulation).
(prolonged APTT)
(1:1 mix)
Mix equal volumes and re-measure APTT immediately (and after 1–2 hours incubation for time-dependent inhibitors)
Suggests factor deficiency. Normal plasma has provided the missing factor(s), restoring clot formation. Indicates investigation for Haemophilia A, B, Factor XI deficiency, or other factor deficiencies.
Suggests an inhibitor is present. The inhibitor in patient plasma neutralises the normal factors from the added plasma. Indicates lupus anticoagulant, acquired Factor VIII inhibitor, or heparin contamination.
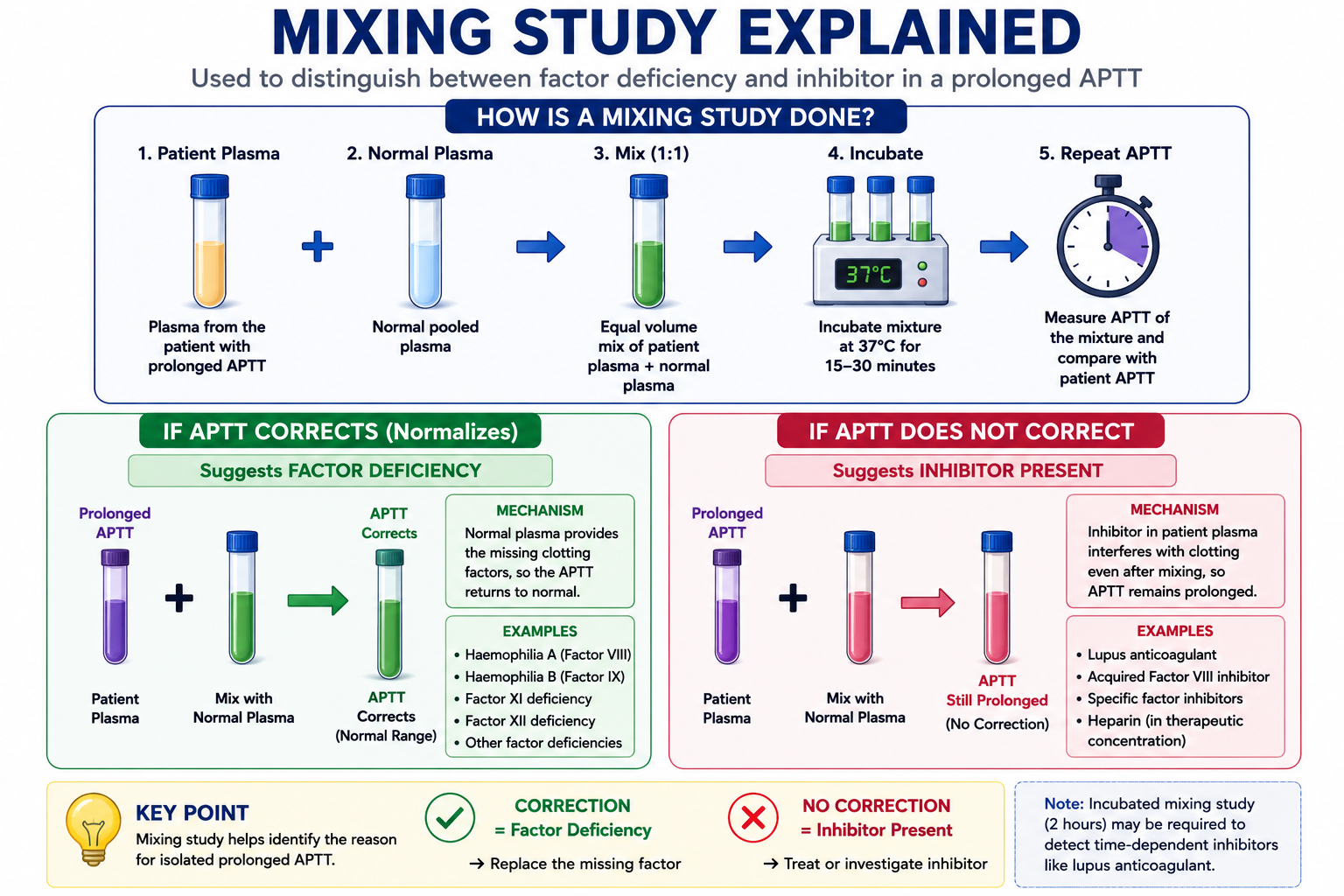
Some inhibitors — notably acquired Factor VIII inhibitors — are time-dependent and temperature-dependent. A mixing study incubated at 37°C for 1–2 hours may show initial apparent correction that subsequently fails as the inhibitor neutralises the added factor. This is why mixing studies are often repeated after incubation as well as immediately after mixing.
Clinical Uses of APTT
In a bleeding patient, APTT should not be interpreted alone. Initial tests usually include:
- Full blood count and platelet count
- PT / INR
- APTT
- Fibrinogen
- D-dimer if DIC is suspected
- Blood film if thrombocytopaenia or haemolysis is suspected
PT and APTT assess coagulation factors only. They do not directly assess platelet function, von Willebrand factor, or vascular causes of bleeding.
1. Investigation of Bleeding Disorders
APTT is part of the initial coagulation screen alongside PT and fibrinogen in any patient presenting with unexplained bleeding, easy bruising, or pre-operative assessment of haemostasis. Used together, PT and APTT help localise the defect to a specific coagulation pathway.
2. Diagnosis of Haemophilia A and B
In a male patient with a history of joint bleeds, easy bruising, or prolonged bleeding after minor trauma, isolated prolonged APTT with normal PT strongly suggests haemophilia. Specific factor VIII and IX assays are required for confirmation and quantification of severity.
3. Monitoring Unfractionated Heparin (UFH)
APTT is the standard test for monitoring therapeutic UFH. The target APTT ratio (patient APTT / mean normal APTT) is typically 1.5–2.5 times normal, though exact targets depend on the clinical indication and local protocol. UFH dose is adjusted based on APTT results measured every 4–6 hours until a stable therapeutic level is reached. Note: LMWH and DOACs are not monitored by APTT.
4. Detection of Lupus Anticoagulant
A persistent isolated prolonged APTT in a patient with a history of recurrent thrombosis, miscarriages, or autoimmune disease should prompt investigation for lupus anticoagulant. Specific phospholipid-sensitive tests (DRVVT, PTTT) are required for formal diagnosis.
5. Evaluation of Acquired Coagulopathies
In acutely unwell patients, APTT combined with PT, fibrinogen, and D-dimers helps diagnose DIC and monitor response to treatment. In liver disease, APTT reflects deficiency of hepatically-synthesised intrinsic pathway factors (IX, XI) alongside PT changes.
Why Is APTT Used to Monitor Unfractionated Heparin?
Unfractionated heparin works by binding to antithrombin and dramatically enhancing its inhibitory activity against thrombin (Factor IIa) and Factor Xa. By slowing the common pathway, heparin predictably prolongs APTT.
Because this prolongation is dose-dependent and reproducible, APTT provides a reliable, real-time measure of the anticoagulant effect of UFH. The APTT is used to titrate UFH infusion rates — if APTT is below target, the dose is increased; if above target, it is reduced or briefly held.
In many protocols, unfractionated heparin is adjusted using the APTT ratio rather than the raw APTT in seconds. A common therapeutic target is approximately 1.5–2.5 times the mean normal APTT, but this range must always be interpreted according to local laboratory calibration and hospital protocol — APTT reagents differ in their sensitivity to heparin, which is why universal targets cannot be applied between institutions.
Therapeutic APTT targets vary between laboratories because APTT reagents differ in heparin sensitivity. Always follow the local heparin protocol rather than applying a universal target blindly. APTT heparin monitoring is also increasingly replaced by anti-Xa monitoring in some centres, particularly where APTT is unreliable due to baseline clotting abnormalities, lupus anticoagulant, or inflammation.
Low molecular weight heparins (LMWH) primarily inhibit Factor Xa rather than thrombin. Because APTT is more sensitive to thrombin inhibition, it does not reliably reflect LMWH activity. Anti-Xa assays are used instead when LMWH monitoring is required. Direct oral anticoagulants (DOACs) variably affect APTT but are not monitored by APTT — specific assays are needed.
Common Misconceptions
False. Factor XII deficiency often causes markedly prolonged APTT — sometimes >100 seconds — but is not associated with clinical bleeding. Contact activation (the Factor XII pathway) is important for clotting in laboratory assays but is not required for effective haemostasis in vivo. Factor XII deficiency is a laboratory finding, not a bleeding disorder. The clinical importance is avoiding unnecessary investigation and treatment.
False. Despite prolonging APTT in the laboratory, lupus anticoagulant is associated with thrombosis rather than bleeding — both arterial and venous. It is a key feature of antiphospholipid syndrome (APS). The paradox arises because lupus anticoagulant interferes with phospholipid-dependent assays in vitro but promotes thrombosis through different mechanisms in vivo.
False. Several clinically significant bleeding disorders are associated with a completely normal APTT. These include von Willebrand disease (mild to moderate), platelet function disorders (e.g. Glanzmann thrombasthenia), Factor XIII deficiency (not tested by APTT), and mild Factor VIII or IX deficiency where factor level is above the threshold for APTT prolongation. A normal APTT therefore does not exclude a clinically significant bleeding disorder.
False. PT and APTT test fundamentally different pathways and are not interchangeable. Haemophilia produces a normal PT and prolonged APTT; early warfarin effect produces a prolonged PT (via Factor VII) with a normal APTT. Using only one test would miss the diagnosis in each scenario.
Exam Tips
- PT evaluates the extrinsic + common pathway; APTT evaluates the intrinsic + common pathway.
- Factor VII is exclusive to the extrinsic pathway — deficiency or early warfarin effect prolongs PT but not APTT.
- Haemophilia A = Factor VIII deficiency; Haemophilia B = Factor IX deficiency. Both cause isolated prolonged APTT.
- Both PT and APTT prolonged → think DIC, severe liver disease, common pathway deficiency, or massive transfusion.
- Mixing study: corrects → factor deficiency; does not correct → inhibitor present.
- Factor XII deficiency: prolonged APTT, no bleeding — contact activation is not required for in vivo haemostasis.
- Lupus anticoagulant: prolonged APTT, increased thrombosis risk — the clue is thrombosis, not bleeding.
- APTT monitors UFH (target ratio 1.5–2.5 × normal); PT/INR monitors warfarin. Neither reliably monitors DOACs or LMWH.
- Normal PT + normal APTT does not exclude bleeding disorders — platelet disorders, vWD, and Factor XIII deficiency are missed by both tests.
Frequently Asked Questions
Key Takeaways
- APTT measures clotting via the intrinsic + common pathway; PT measures via the extrinsic + common pathway
- Factors assessed by APTT: XII, XI, IX, VIII (intrinsic) and X, V, II, I (common); Factor VII is NOT assessed
- Haemophilia A = Factor VIII deficiency; Haemophilia B = Factor IX deficiency — both cause isolated prolonged APTT
- Isolated prolonged APTT (normal PT) → intrinsic pathway problem — haemophilia, lupus anticoagulant, or heparin contamination
- Both PT and APTT prolonged → common pathway, DIC, severe liver disease, or massive transfusion
- Mixing study: correction = factor deficiency; failure to correct = inhibitor present
- Factor XII deficiency: markedly prolonged APTT with no clinical bleeding
- Lupus anticoagulant: prolongs APTT but causes thrombosis, not bleeding
- APTT monitors UFH (target 1.5–2.5 × normal ratio); it cannot reliably monitor LMWH or DOACs
- Normal APTT does not exclude platelet disorders, von Willebrand disease, or Factor XIII deficiency
References
- Lippi G, Favaloro EJ, Franchini M. Diagnostics of coagulation disorders. Semin Thromb Hemost. 2013;39(3):236–243.
- Bain BJ, Bates I, Laffan MA, eds. Dacie and Lewis Practical Haematology. 12th ed. London: Elsevier; 2017.
- Brummel-Ziedins K, Mann KG. Molecular basis of blood coagulation. In: Hoffman R, et al, eds. Hematology: Basic Principles and Practice. 7th ed. Philadelphia: Elsevier; 2018.
- Keeling D, Tait RC, Watson H. Peri-operative management of anticoagulation and antiplatelet therapy. Br J Haematol. 2016;175(4):602–613.
- Baglin T, et al. British Committee for Standards in Haematology guidelines for the investigation and management of antiphospholipid syndrome. Br J Haematol. 2012;157(1):47–58.
- Srivastava A, et al. WFH Guidelines for the Management of Hemophilia. 3rd ed. Haemophilia. 2020;26(Suppl 6):1–158.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist haematological input when investigating and managing coagulation disorders.