The coagulation cascade is a series of enzyme-mediated reactions that produce a stable fibrin clot at the site of vascular injury. Although modern understanding of haemostasis has evolved beyond the traditional cascade model, the intrinsic, extrinsic, and common pathway framework remains one of the most important concepts in medical education for medical students and clinicians who encounter coagulation testing.
Understanding the coagulation cascade allows clinicians to interpret PT and APTT results correctly, understand bleeding disorders such as haemophilia, and recognise the characteristic laboratory patterns seen in conditions such as disseminated intravascular coagulation (DIC) and severe liver disease. Accurate PT and APTT interpretation depends directly on knowing which clotting factors each pathway contains and which test assesses each pathway.
This article should be read alongside PT and INR Explained, APTT Explained, and How INR Is Calculated — together they form a complete picture of coagulation testing and its clinical interpretation.
Extrinsic Pathway + Intrinsic Pathway
↓
Common Pathway
↓
Fibrin Clot
The coagulation cascade is a sequence of clotting factor activations that ultimately generates fibrin and stabilises a blood clot.
Learning Objectives
- Describe the intrinsic pathway and identify its major clotting factors
- Describe the extrinsic pathway and identify its major clotting factors
- Describe the common pathway and explain how it produces a fibrin clot
- Identify which factors belong to each pathway
- Explain how PT and APTT relate to the coagulation cascade
- Understand why haemophilia A and B prolong APTT but not PT
- Explain why Factor VII deficiency prolongs PT but not APTT
- Recognise which conditions prolong both PT and APTT
Why Does the Body Need the Coagulation Cascade?
The coagulation system exists to prevent excessive bleeding following vascular injury. When a blood vessel is damaged, the body must rapidly form a clot to limit blood loss, while simultaneously confining that clot to the site of injury to avoid widespread thrombosis.
The cascade achieves three critical goals:
- Rapid clot formation — the enzyme cascade amplifies a small initial signal into a large, rapid clotting response
- Amplification of the haemostatic response — each activated factor activates many molecules of the next factor, dramatically amplifying the signal
- Localisation of clotting to the site of injury — natural anticoagulants confine clotting to the area of damage, preventing widespread thrombosis
Without a tightly regulated coagulation system, even minor trauma could result in life-threatening haemorrhage, and without equally tight regulation, spontaneous thrombosis would be equally dangerous.
Haemostasis is the broader process of stopping bleeding and includes primary haemostasis (platelet plug formation), secondary haemostasis (the coagulation cascade, which reinforces the platelet plug with fibrin), and fibrinolysis (clot dissolution once healing is complete). This article focuses on secondary haemostasis — the coagulation cascade.
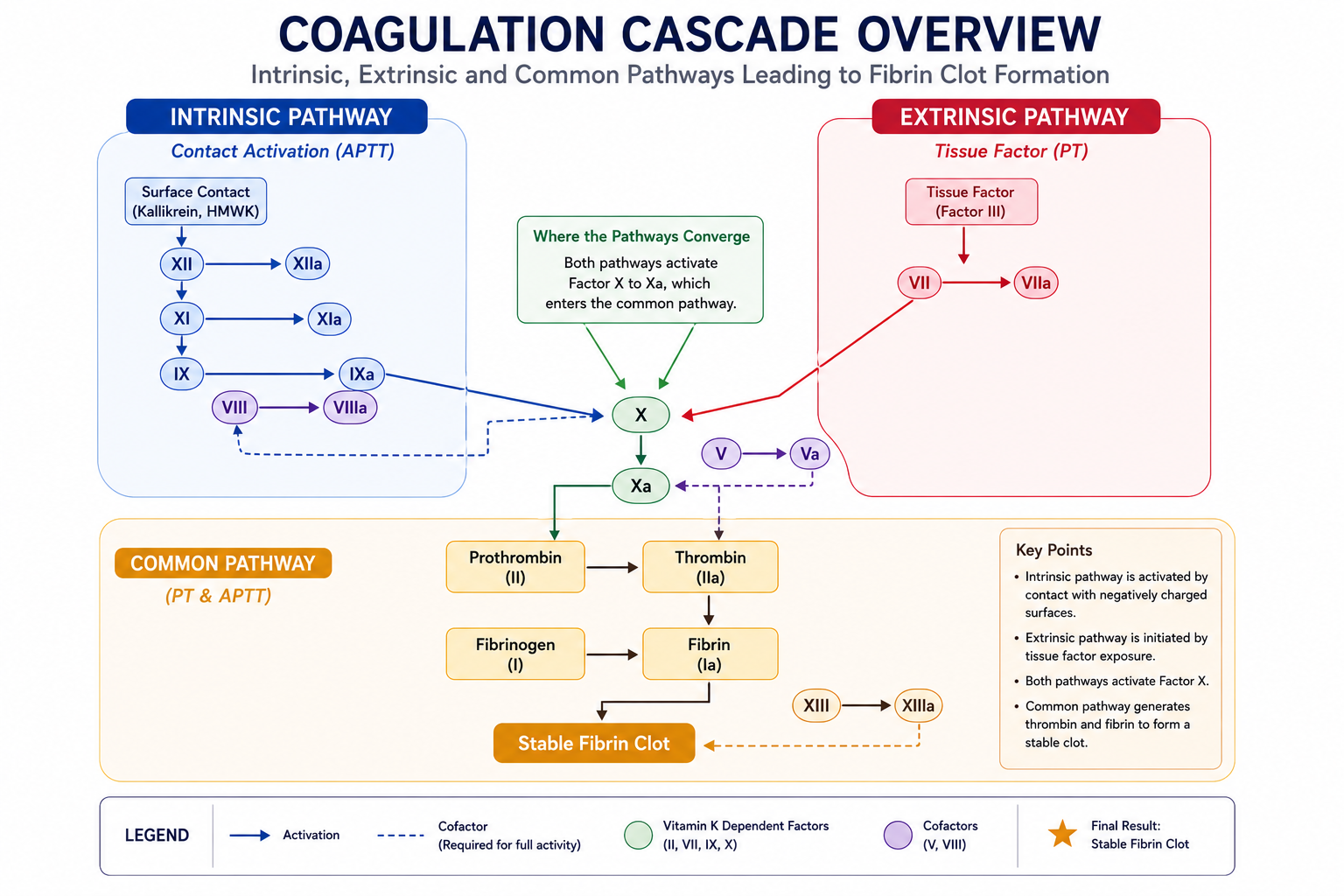
The Traditional Coagulation Cascade
The traditional model divides coagulation into three interconnected pathways:
Assessed by PT
Assessed by APTT
Although this model simplifies a much more complex biological process, it remains extremely useful for understanding coagulation tests and bleeding disorders. The traditional cascade model directly maps onto PT and APTT — the two most commonly requested coagulation tests in clinical practice.
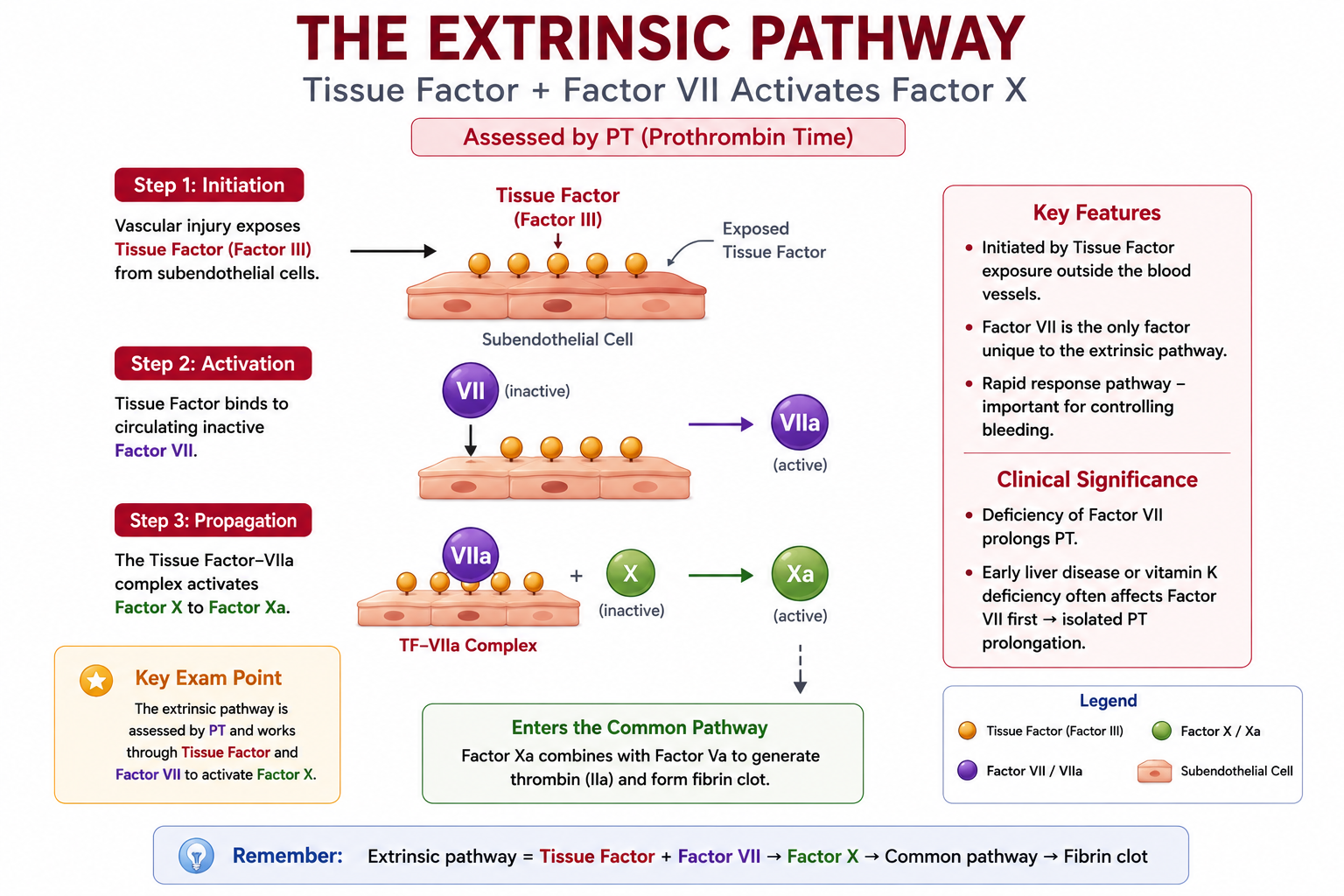
The Extrinsic Pathway
The extrinsic pathway is the primary initiator of coagulation following vascular injury. It is called "extrinsic" because it is triggered by a substance — tissue factor — that originates outside the bloodstream, from the damaged vessel wall and surrounding tissues.
Key Components
The extrinsic pathway involves just two essential components:
- Tissue Factor (TF) — a transmembrane protein expressed on cells beneath the vascular endothelium (fibroblasts, smooth muscle cells). Normally not exposed to circulating blood; exposed when the vessel wall is disrupted.
- Factor VII — a vitamin K-dependent serine protease that circulates in plasma. Binds tissue factor at the site of injury.
The Sequence
The tissue factor–Factor VIIa complex is a powerful activator of Factor X (which begins the common pathway) and also of Factor IX (which links the extrinsic and intrinsic pathways). This cross-activation is one reason why the two-pathway model is a simplification of a more interconnected process.
PT (Prothrombin Time) primarily assesses the extrinsic pathway. Factor VII is the key factor unique to the extrinsic pathway. Early vitamin K deficiency, early warfarin effect, and Factor VII deficiency all prolong PT with a normal APTT — because the intrinsic pathway remains intact.
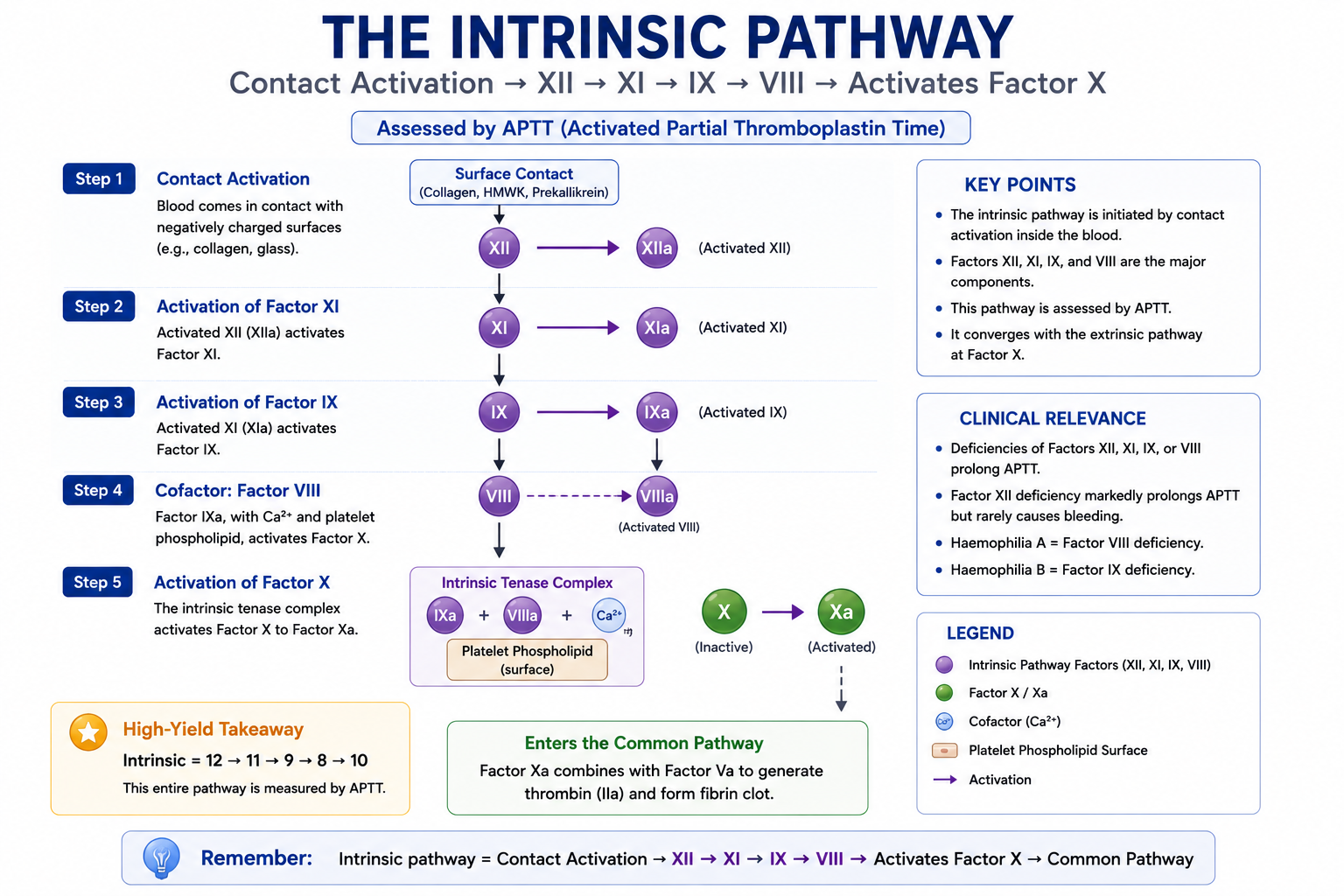
The Intrinsic Pathway
The intrinsic pathway is called "intrinsic" because all the components required to trigger it are found within — intrinsic to — the bloodstream. It is activated by contact activation, which occurs when Factor XII contacts a negatively charged surface such as exposed collagen, glass, or certain foreign materials.
In modern haemostasis, the in vivo role of contact activation is less critical than the extrinsic pathway for initiating clot formation — but Factors VIII and IX within the intrinsic pathway are essential for amplifying and sustaining the coagulation response. This is why haemophilia (affecting Factors VIII or IX) causes significant bleeding despite an intact extrinsic pathway.
Key Factors
The intrinsic pathway involves four major coagulation factors, activated sequentially:
- Factor XII (Hageman Factor) — contact activation initiator. Deficiency causes markedly prolonged APTT but no clinical bleeding.
- Factor XI — activated by Factor XII; activates Factor IX. Deficiency causes variable bleeding (Haemophilia C).
- Factor IX (Christmas Factor) — activated by Factor XI; activates Factor X in conjunction with Factor VIII. Deficiency causes Haemophilia B.
- Factor VIII (Antihemophilic Factor) — acts as a cofactor for Factor IXa, dramatically accelerating activation of Factor X. Deficiency causes Haemophilia A — the most common severe inherited coagulation disorder.
The Sequence
APTT (Activated Partial Thromboplastin Time) primarily assesses the intrinsic pathway. Factors XII, XI, IX, and VIII are the intrinsic pathway factors assessed by APTT. Deficiency of any of these factors (except Factor XII, which does not cause bleeding) may cause significant haemorrhage and will prolong APTT with a normal PT.
Factor XII is important in laboratory coagulation testing but is usually not essential for normal haemostasis in vivo. Factor XII deficiency can cause a markedly prolonged APTT — sometimes very prolonged — but it is not associated with clinical bleeding. This is a classic examination point: a prolonged APTT does not always mean bleeding risk. When APTT is markedly prolonged but the patient has no bleeding history, Factor XII deficiency should be considered alongside lupus anticoagulant. Mixing studies and factor assays are required to clarify the cause.
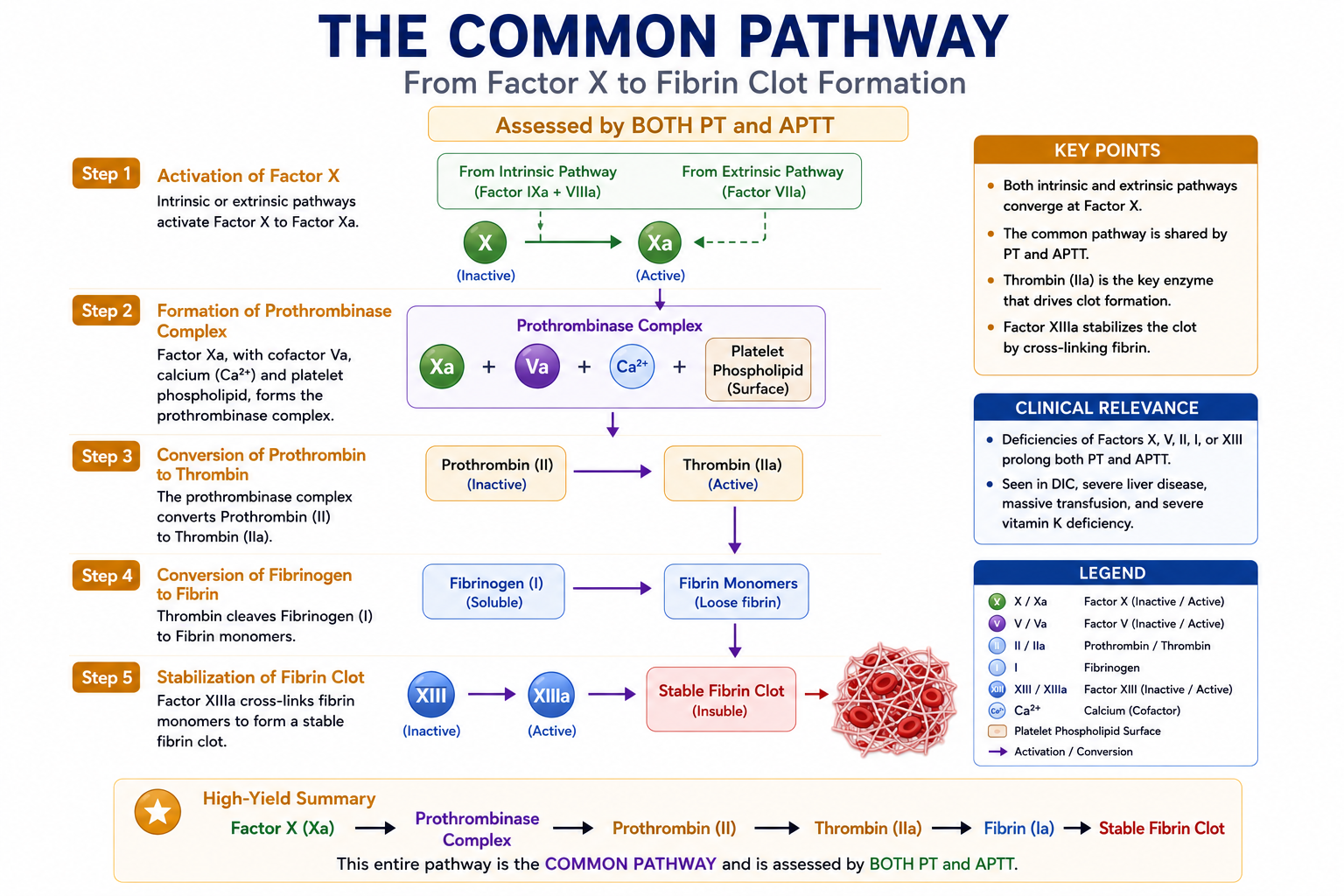
The Common Pathway
Both the extrinsic and intrinsic pathways converge at Factor X, which marks the beginning of the common pathway. The common pathway produces the final clot — converting prothrombin to thrombin, and thrombin to a fibrin mesh that stabilises the platelet plug.
Key Factors
- Factor X (Stuart Factor) — the first factor of the common pathway; activated by both the extrinsic and intrinsic pathways. Factor Xa combines with Factor Va to form the prothrombinase complex.
- Factor V (Labile Factor) — acts as a cofactor for Factor Xa, accelerating conversion of prothrombin to thrombin. Factor V is synthesised in the liver but is not vitamin K dependent; therefore, vitamin K cannot correct Factor V deficiency. This makes Factor V a useful marker of liver synthetic function independent of vitamin K status.
- Factor II (Prothrombin) — a vitamin K-dependent factor converted to thrombin by the prothrombinase complex (Factor Xa + Va). Thrombin is the central enzyme of coagulation.
- Factor I (Fibrinogen) — converted to fibrin by thrombin. Fibrin monomers polymerise to form the fibrin mesh that stabilises the clot.
The Sequence
Thrombin is also a powerful activator in its own right — it amplifies the coagulation cascade by activating Factors V, VIII, and XI, creating a positive feedback loop that rapidly generates more thrombin. Factor XIII, also activated by thrombin, cross-links fibrin strands to form a more mechanically stable clot.
Thrombin (Factor IIa) is the central enzyme of coagulation. Beyond converting fibrinogen to fibrin, thrombin amplifies the cascade by activating Factors V, VIII, and XI; activates platelets; activates Factor XIII (which cross-links fibrin); and activates protein C (a natural anticoagulant). Thrombin is both pro-coagulant and part of the regulation of clotting — its activity is tightly controlled by antithrombin and other inhibitors.
Which Factors Belong to Which Pathway?
The following table provides a high-yield summary of coagulation factors organised by pathway. Memorising this table will allow you to interpret PT and APTT results and localise coagulation defects rapidly.
| Pathway | Factors | Test | Clinically Significant Deficiency |
|---|---|---|---|
| Extrinsic | VII | PT/INR | Factor VII deficiency, early warfarin/vitamin K deficiency |
| Intrinsic | XII, XI, IX, VIII | APTT | Haemophilia A (VIII), Haemophilia B (IX), Factor XI deficiency; Factor XII — prolonged APTT, no bleeding |
| Common | X, V, II, I | Both PT & APTT | DIC, severe liver disease, massive transfusion, vitamin K deficiency (II, X), Factor V deficiency |
Intrinsic = 12 → 11 → 9 → 8 (count down from 12, skip 10)
Extrinsic = 7 (lucky number 7, only one factor)
Common = 10 → 5 → 2 → 1 (Factor X starts the common pathway, ends with fibrin = Factor I)
Vitamin K-Dependent Factors
Several coagulation factors require vitamin K for their synthesis and are affected by vitamin K deficiency and warfarin therapy. These are remembered with the mnemonic "1972" — Factors II, VII, IX, X, plus Protein C and Protein S:
Factor II — Common pathway (prothrombin)
Factor VII — Extrinsic pathway
Factor IX — Intrinsic pathway
Factor X — Common pathway
Protein C — Natural anticoagulant
Protein S — Natural anticoagulant (cofactor for Protein C)
Factor VII has the shortest half-life of all vitamin K-dependent factors, so PT becomes abnormal early in vitamin K deficiency or warfarin therapy — before APTT is affected.
| Vitamin K-Dependent Factors | Pathway | Effect of Deficiency |
|---|---|---|
| Factor II (Prothrombin) | Common | Prolongs both PT and APTT |
| Factor VII | Extrinsic | Prolongs PT only (earliest to fall in vitamin K deficiency) |
| Factor IX | Intrinsic | Prolongs APTT |
| Factor X | Common | Prolongs both PT and APTT |
| Protein C, Protein S | Natural anticoagulants | Deficiency increases thrombosis risk |
Factor VII has the shortest half-life of all coagulation factors (approximately 4–6 hours). When vitamin K is deficient or warfarin is started, Factor VII levels fall first — which is why PT (and hence INR) is the first coagulation test to become abnormal. APTT may initially remain normal while PT is already prolonged.
Factor VII → PT / extrinsic pathway
Factor VIII → Haemophilia A
Factor IX → Haemophilia B
Factor X → start of the common pathway
Factor V → cofactor in prothrombinase complex; liver-synthesised but not vitamin K dependent
Factor II → prothrombin → thrombin
Factor I → fibrinogen → fibrin
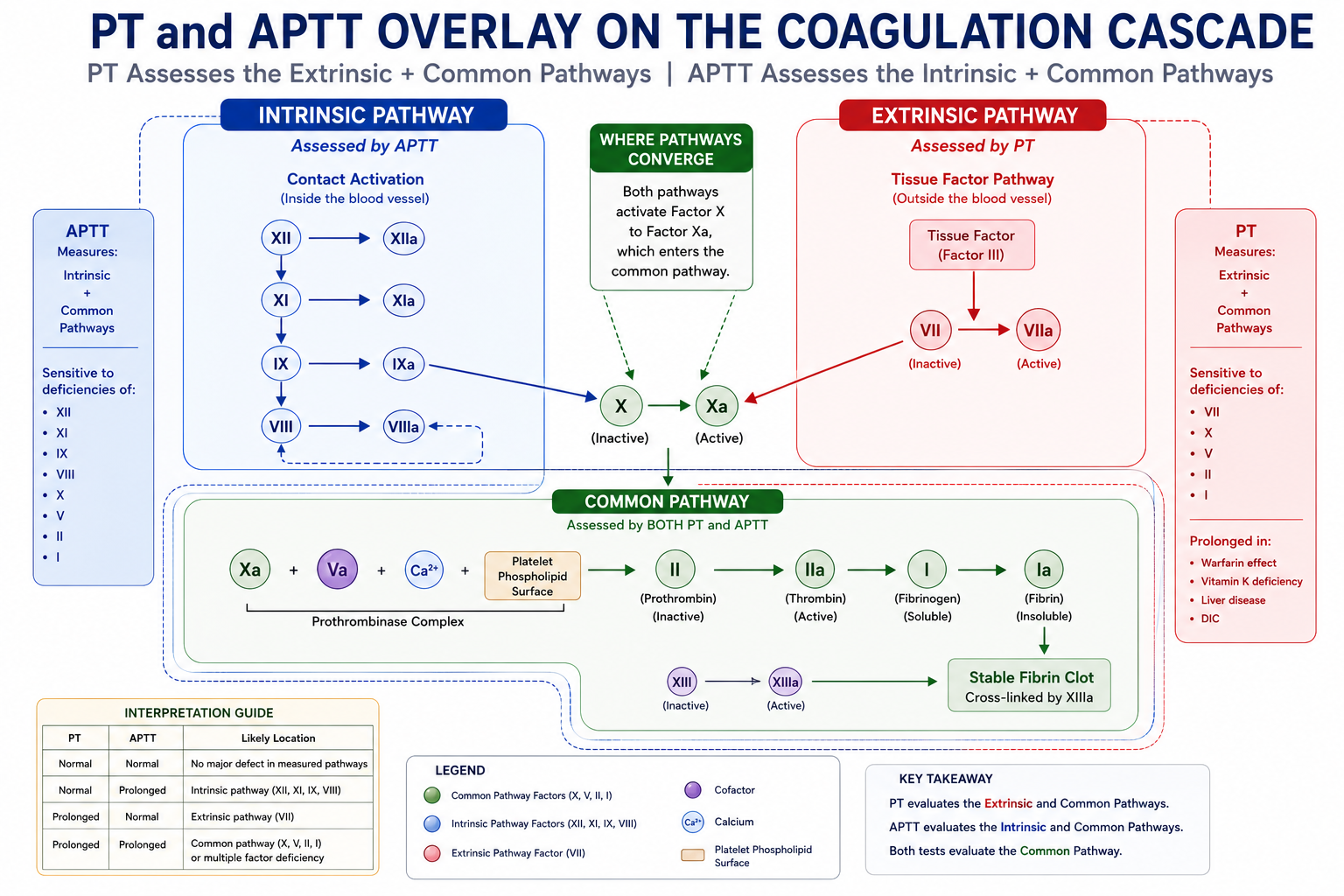
PT and APTT on the Coagulation Cascade
PT and APTT are best understood when viewed directly on the coagulation cascade. Each test selectively activates specific pathways and therefore identifies defects in different groups of clotting factors.
| Test | Pathway Assessed | Key Unique Factors | Clinical Use |
|---|---|---|---|
| PT / INR | Extrinsic + Common | Factor VII | Monitors warfarin; liver disease; vitamin K deficiency |
| APTT | Intrinsic + Common | VIII, IX, XI, XII | Monitors heparin (UFH); haemophilia; lupus anticoagulant |
Interpreting PT and APTT Together
The pattern of PT and APTT abnormality helps localise the defect to a specific pathway before more detailed factor assays are requested:
| PT | APTT | Likely Location | Common Causes |
|---|---|---|---|
| Normal | Normal | No major defect in measured pathways | Does not exclude platelet disorders, vWD, Factor XIII deficiency, or mild factor deficiency |
| Normal | Prolonged | Intrinsic pathway | Haemophilia A/B, Factor XI/XII deficiency, lupus anticoagulant, heparin |
| Prolonged | Normal | Extrinsic pathway | Factor VII deficiency, early warfarin, early vitamin K deficiency |
| Prolonged | Prolonged | Common pathway or multiple factor deficiency | DIC, severe liver disease, massive transfusion, severe vitamin K deficiency, Factor X/V/II/I deficiency |
Normal PT + prolonged APTT = intrinsic pathway problem.
Prolonged PT + normal APTT = extrinsic pathway problem.
Both prolonged = common pathway or multiple factor deficiency (DIC, liver disease, massive transfusion).
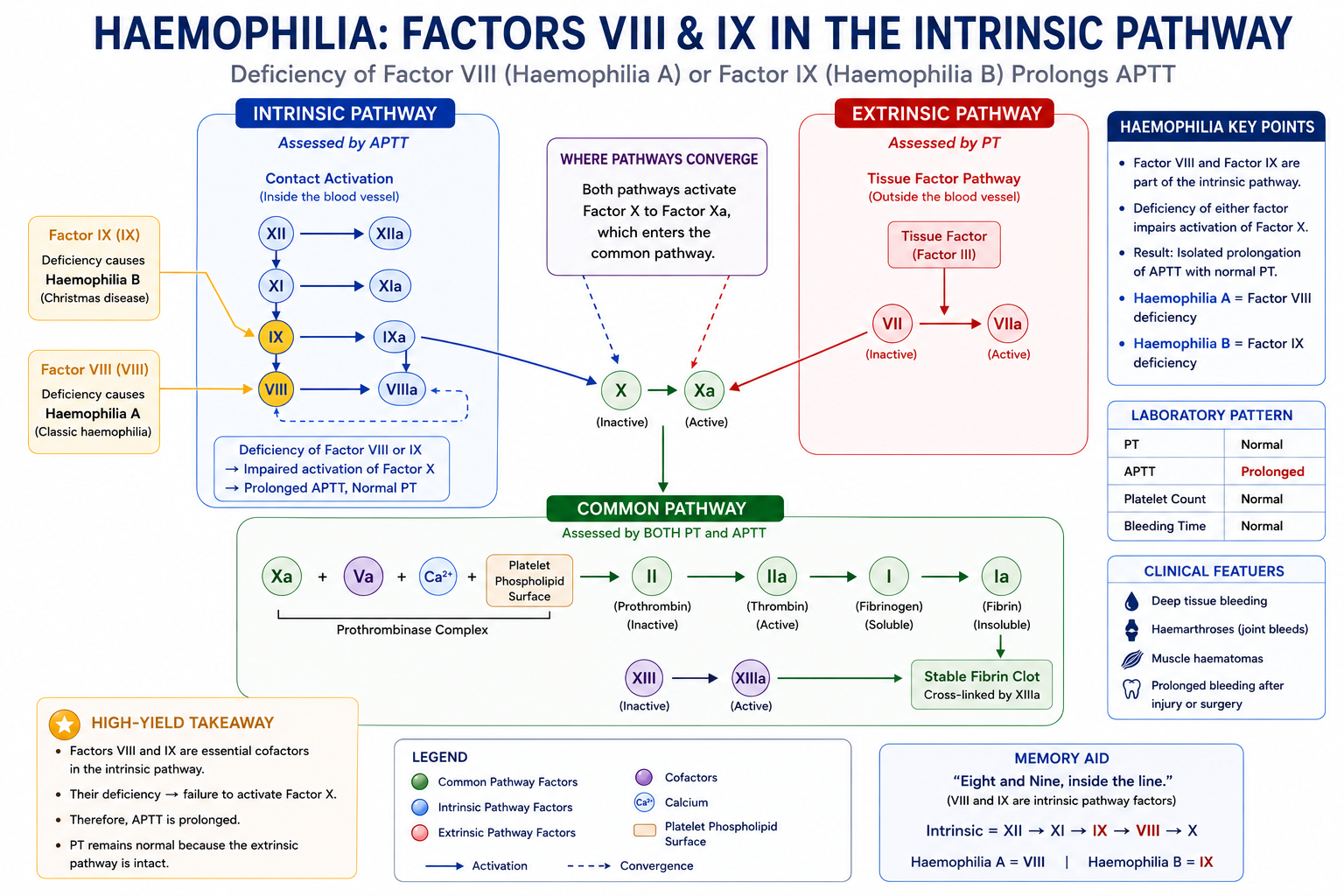
Haemophilia and the Coagulation Cascade
Haemophilia demonstrates perfectly why understanding the cascade is clinically important. It explains a common examination scenario: why does a patient bleed severely despite a normal PT?
Haemophilia A — Factor VIII Deficiency
Factor VIII belongs to the intrinsic pathway. It acts as an essential cofactor for Factor IXa, dramatically accelerating the activation of Factor X. Without Factor VIII, the intrinsic pathway cannot efficiently generate Factor Xa, and clot formation is severely impaired.
Because Factor VIII is intrinsic pathway only, and PT assesses only the extrinsic and common pathways:
- APTT — prolonged (intrinsic pathway impaired)
- PT — normal (extrinsic pathway and common pathway intact)
Haemophilia B — Factor IX Deficiency
Factor IX also belongs to the intrinsic pathway. Without Factor IX, the intrinsic pathway cannot activate Factor X, with the same net result as haemophilia A. The laboratory pattern is identical to Haemophilia A — isolated prolonged APTT — and specific factor assays are required to distinguish the two conditions.
| Condition | Affected Factor | Pathway | PT | APTT |
|---|---|---|---|---|
| Haemophilia A | Factor VIII | Intrinsic | Normal | Prolonged |
| Haemophilia B | Factor IX | Intrinsic | Normal | Prolonged |
| Factor XI deficiency | Factor XI | Intrinsic | Normal | Prolonged |
| Factor XII deficiency | Factor XII | Intrinsic | Normal | Prolonged (no bleeding) |
APTT identifies an abnormality within the intrinsic pathway but cannot distinguish Haemophilia A from Haemophilia B — the APTT result is prolonged in both. Specific factor assays for Factor VIII and Factor IX are required to reach a diagnosis and quantify severity.
Factor VII Deficiency and PT
Factor VII belongs exclusively to the extrinsic pathway. It is the only coagulation factor that can be detected by PT but not by APTT. This makes isolated Factor VII deficiency a distinctive pattern on coagulation testing.
The most common causes of a prolonged PT with normal APTT in clinical practice are not inherited Factor VII deficiency (which is rare) but rather early vitamin K deficiency and early warfarin effect. Factor VII has the shortest half-life of all coagulation factors, so its level falls earliest as vitamin K stores are depleted.
A patient on warfarin or with early liver disease may present with prolonged PT and normal APTT. The explanation is that Factor VII (extrinsic pathway, short half-life) is affected first, while intrinsic pathway factors remain adequate. As vitamin K deficiency or liver disease worsens, APTT also becomes prolonged as Factors IX, XI, and common pathway factors are depleted.
Disorders Affecting the Common Pathway
Conditions that affect the common pathway — or that deplete multiple clotting factors across several pathways — typically prolong both PT and APTT. This pattern is an important clinical clue.
Common Causes of Both PT and APTT Being Prolonged
- Disseminated intravascular coagulation (DIC) — widespread activation of coagulation consumes multiple factors including fibrinogen, Factor V, Factor VIII, and prothrombin. Laboratory findings: prolonged PT and APTT, low fibrinogen, elevated D-dimers, thrombocytopaenia.
- Severe liver disease — the liver synthesises most coagulation factors. Severe liver failure reduces Factors I, II, V, VII, IX, X, and XI. All pathways are affected, producing prolonged PT and APTT alongside low fibrinogen and reduced protein C.
- Massive transfusion / dilutional coagulopathy — large volumes of packed red cells dilute clotting factors. Both PT and APTT are prolonged once significant dilution occurs.
- Severe vitamin K deficiency — initially prolongs PT only (Factor VII, shortest half-life); as deficiency worsens, Factors IX and X are also depleted, prolonging APTT and worsening PT.
- Specific common pathway factor deficiencies — deficiency of Factor X, V, II (prothrombin), or I (fibrinogen/afibrinogenaemia) prolongs both PT and APTT because these factors are shared by both pathways.
DIC is the most important cause of both PT and APTT being prolonged in an acutely unwell patient. The complete laboratory picture of DIC is: prolonged PT + prolonged APTT + low fibrinogen + elevated D-dimers + thrombocytopaenia. All five should be considered together rather than any single result alone.
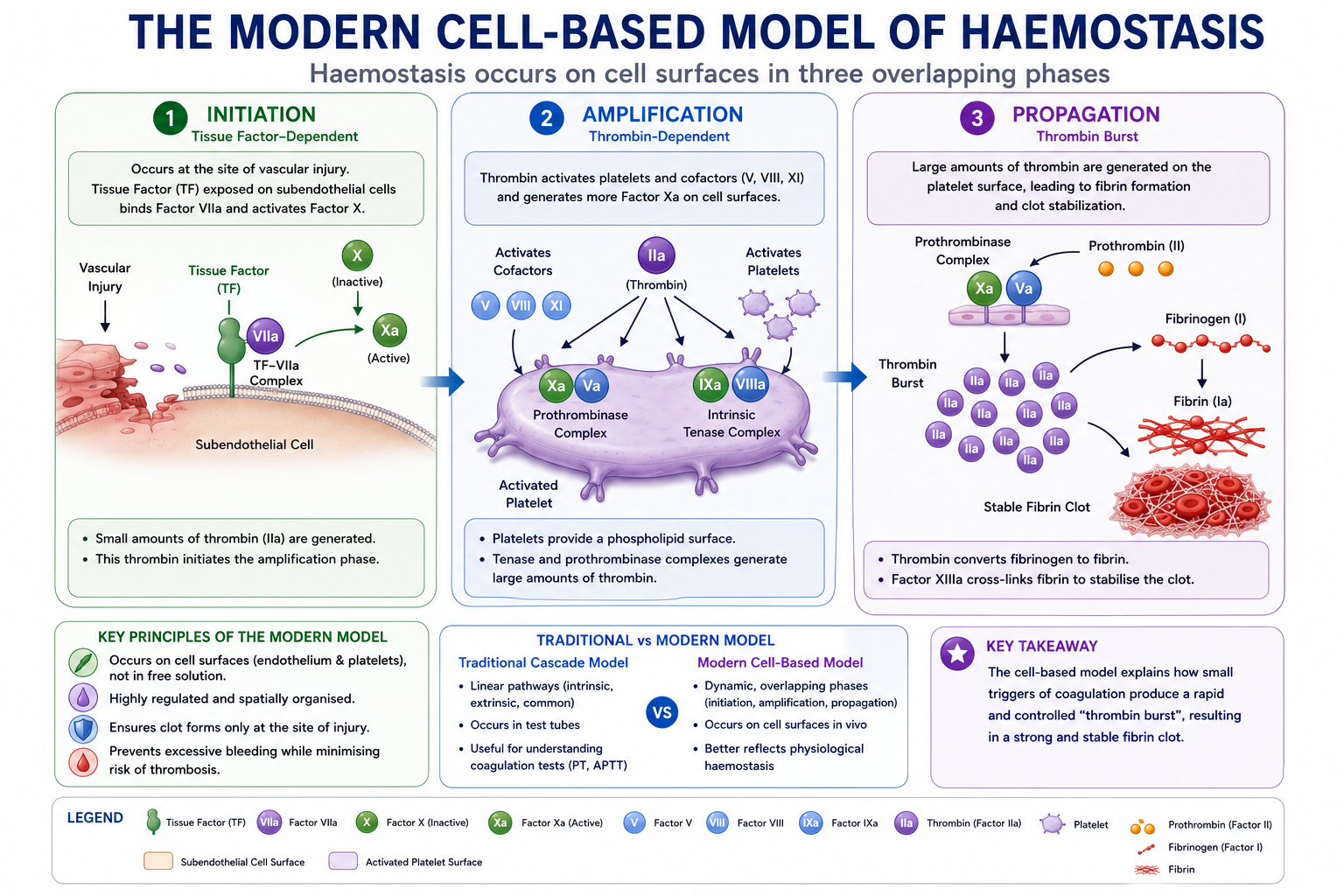
The Modern Cell-Based Model of Haemostasis
The traditional coagulation cascade — intrinsic, extrinsic, and common pathways — remains the most useful framework for understanding coagulation tests and clinical bleeding disorders. However, it does not fully reflect how clotting actually occurs in the body.
Modern understanding describes haemostasis as occurring in three overlapping phases on cellular surfaces, rather than as isolated pathways floating freely in plasma:
Phase 1 — Initiation
Tissue factor on subendothelial cells binds Factor VII. The TF–VIIa complex activates small amounts of Factors X and IX. Initial thrombin is generated, but regulatory mechanisms (TFPI — tissue factor pathway inhibitor) rapidly limit this phase, so only a small amount of clot forms initially.
Phase 2 — Amplification
The small amount of thrombin generated in initiation is enough to amplify the response. Thrombin activates platelets (which adhere to the damaged vessel wall), and activates Factors V, VIII, and XI — powerfully reinforcing the cascade. Activated platelets provide the phospholipid surface on which the coagulation complexes assemble.
Phase 3 — Propagation
Large amounts of thrombin are generated on the surface of activated platelets. The tenase complex (Factor IXa + VIIIa) and the prothrombinase complex (Factor Xa + Va) operate at maximum efficiency on the platelet surface. Massive fibrin generation occurs, producing a stable clot.
The cell-based model explains why Factors VIII and IX (intrinsic pathway) are so important despite the extrinsic pathway being the primary in vivo initiator. Factor VIII and IX activity is critical for the amplification and propagation phases — which generate the large amounts of thrombin needed to form a mechanically strong fibrin clot. This is why haemophilia (Factor VIII or IX deficiency) causes severe bleeding even though the extrinsic pathway is intact.
Common Misconceptions
The term "intrinsic" can be misleading. It was originally coined because all the components of the intrinsic pathway are found within the bloodstream — unlike the extrinsic pathway, which requires tissue factor from outside the blood. It does not mean that the intrinsic pathway is confined to the lumen of blood vessels. In the cell-based model, clotting occurs on cellular surfaces including activated platelets and endothelial cells.
False. Factor XII deficiency often causes markedly prolonged APTT — sometimes exceeding 100 seconds — but is not associated with clinical bleeding. Contact activation (the Factor XII pathway) is important for coagulation in laboratory assays but is not required for effective haemostasis in vivo. This was established by John Hageman, after whom Factor XII is named — he was found incidentally to have undetectable Factor XII with no bleeding history. Always consider Factor XII deficiency when APTT is markedly prolonged without clinical bleeding.
False. PT and APTT assess coagulation factors only — they measure the time for plasma to clot via the respective pathway. They do not directly assess platelet count, platelet function, von Willebrand factor, or vascular integrity. A patient with severe platelet dysfunction may have a completely normal PT and APTT. This is why the initial coagulation screen for a bleeding patient should include both PT/APTT and a platelet count — not PT/APTT alone.
False. In modern understanding, the extrinsic pathway (tissue factor + Factor VII) is the primary initiator of in vivo coagulation. The intrinsic pathway is critical for amplifying and sustaining the clotting response, but the extrinsic pathway starts the process. This is why Factor VII deficiency can cause bleeding despite an intact intrinsic pathway — sufficient thrombin cannot be generated from the extrinsic pathway alone without Factor VII.
Exam Tips
- Factor VII → PT only (shortest half-life; first to fall in vitamin K deficiency)
- Factors VIII, IX, XI, XII → APTT only (intrinsic pathway)
- Factor X = start of the common pathway — deficiency prolongs both PT and APTT
- Haemophilia A = Factor VIII deficiency — isolated prolonged APTT; X-linked recessive
- Haemophilia B = Factor IX deficiency — identical laboratory pattern to Haemophilia A; requires factor assay to distinguish
- Factor XII deficiency — markedly prolonged APTT, no clinical bleeding
- DIC — often prolongs both PT and APTT; also low fibrinogen, high D-dimers, thrombocytopaenia
- Early warfarin/vitamin K deficiency — prolonged PT, normal APTT (Factor VII falls first)
- Thrombin is the key enzyme — converts fibrinogen to fibrin and amplifies the cascade
- PT and APTT do not assess platelets — always check platelet count and function separately
Frequently Asked Questions
One-Minute Coagulation Cascade Revision
This final summary brings together the most important exam points from the coagulation cascade. It is designed as a rapid revision tool before exams or ward teaching.
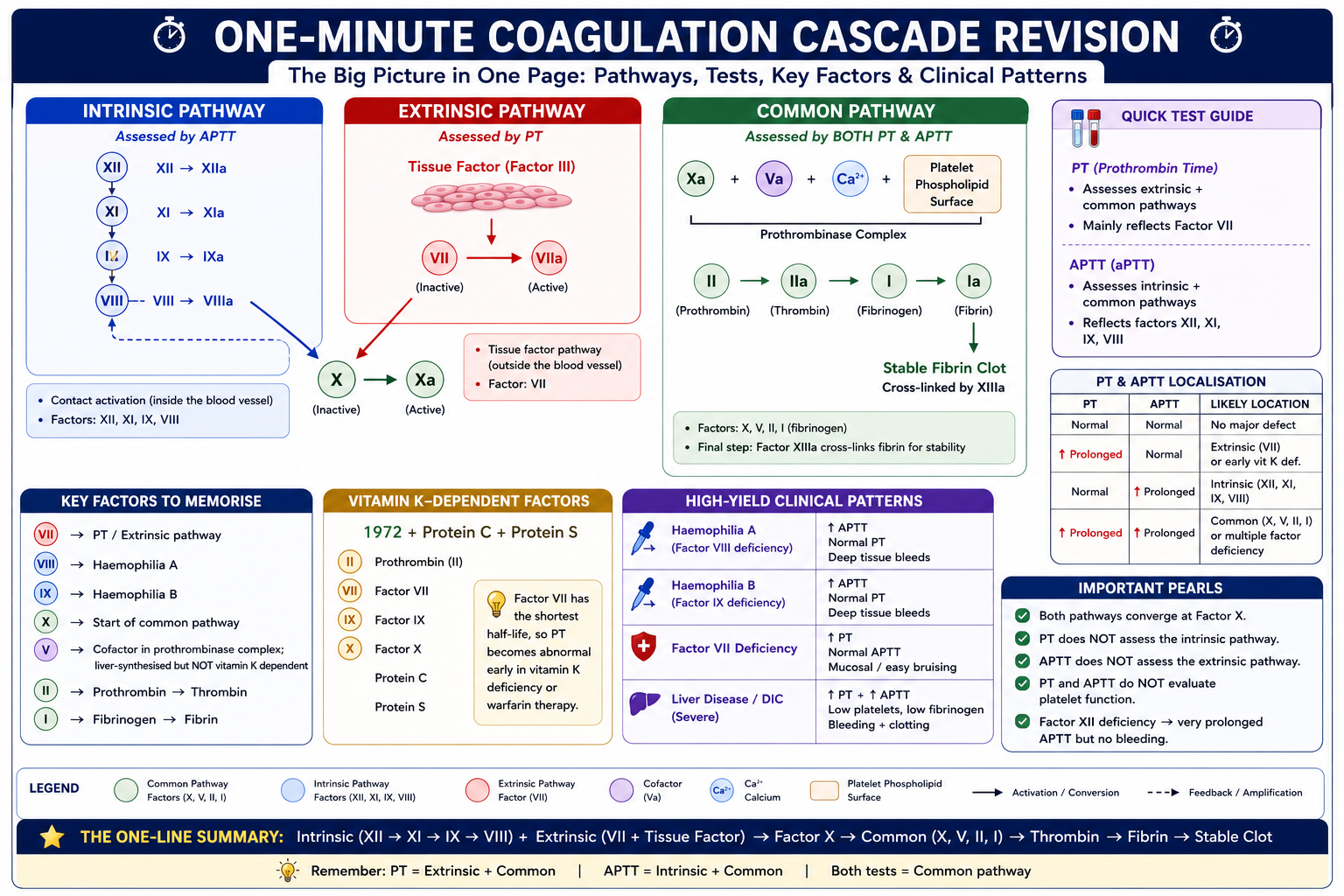
Key Takeaways
- The coagulation cascade consists of three pathways: extrinsic, intrinsic, and common
- The extrinsic pathway is initiated by tissue factor + Factor VII; assessed by PT
- The intrinsic pathway involves Factors XII, XI, IX, VIII; assessed by APTT
- Both pathways converge at Factor X, beginning the common pathway (X, V, II, I)
- PT assesses extrinsic + common; APTT assesses intrinsic + common; both assess common
- Haemophilia A (Factor VIII) and B (Factor IX) cause isolated prolonged APTT — normal PT
- Factor VII deficiency and early vitamin K deficiency cause isolated prolonged PT — normal APTT
- DIC and severe liver disease typically prolong both PT and APTT
- Factor XII deficiency markedly prolongs APTT without causing clinical bleeding
- PT and APTT do not assess platelet function — always check platelets separately
- The modern cell-based model explains why Factors VIII and IX are critical for haemostasis despite the extrinsic pathway being the primary in vivo initiator
References
- Bain BJ, Bates I, Laffan MA, eds. Dacie and Lewis Practical Haematology. 12th ed. London: Elsevier; 2017.
- Hoffman M, Monroe DM. A cell-based model of hemostasis. Thromb Haemost. 2001;85(6):958–965.
- Davie EW, Ratnoff OD. Waterfall sequence for intrinsic blood clotting. Science. 1964;145(3638):1310–1312.
- Mackman N. Triggers, targets and treatments for thrombosis. Nature. 2008;451(7181):914–918.
- Monroe DM, Hoffman M. What does it take to make the perfect clot? Arterioscler Thromb Vasc Biol. 2006;26(1):41–48.
- Srivastava A, et al. WFH Guidelines for the Management of Hemophilia. 3rd ed. Haemophilia. 2020;26(Suppl 6):1–158.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist haematological input when investigating and managing coagulation disorders.
- Why the Cascade Exists
- Traditional Cascade
- Extrinsic Pathway
- Intrinsic Pathway
- Common Pathway
- Factors by Pathway
- Most Important Factors
- PT and APTT on the Cascade
- Haemophilia
- Factor VII Deficiency
- Common Pathway Disorders
- Modern Cell-Based Model
- Common Misconceptions
- Exam Tips
- FAQ
- One-Minute Revision
- Key Takeaways
- References