Disseminated Intravascular Coagulation (DIC) is a serious systemic disorder characterised by uncontrolled activation of coagulation throughout the circulation. The result is widespread microvascular thrombosis, consumption of platelets and coagulation factors, activation of fibrinolysis, and ultimately an increased risk of bleeding.
One of the most important concepts in DIC is that clotting and bleeding occur simultaneously. Understanding this apparent paradox is essential for interpreting the laboratory findings and clinical manifestations of DIC.
Read this article alongside APTT Explained and Coagulation Cascade Explained — together they cover the complete haemostasis cluster.
DIC is often described as a consumptive coagulopathy.
Learning Objectives
- Define disseminated intravascular coagulation
- Explain why clotting and bleeding coexist in DIC
- Recognise common causes of DIC
- Interpret the typical laboratory pattern of DIC
- Explain why D-dimer is elevated in DIC
- Differentiate acute and chronic DIC clinically and in the laboratory
- Understand the ISTH DIC scoring system
What Does DIC Mean?
DIC stands for three words that together describe the nature of the disorder:
Disseminated
Widespread throughout the circulation — not confined to a single site, as in normal haemostasis.
Intravascular
Occurring inside blood vessels — coagulation is activated within the vascular compartment itself.
Coagulation
Activation of the coagulation cascade — the same system that forms protective clots is activated pathologically throughout the body.
Unlike normal haemostasis, which is localised to the site of vascular injury, DIC activates coagulation throughout the body. This systemic, uncontrolled activation is what makes DIC so dangerous and diagnostically distinctive.
Why Do Clotting and Bleeding Coexist?
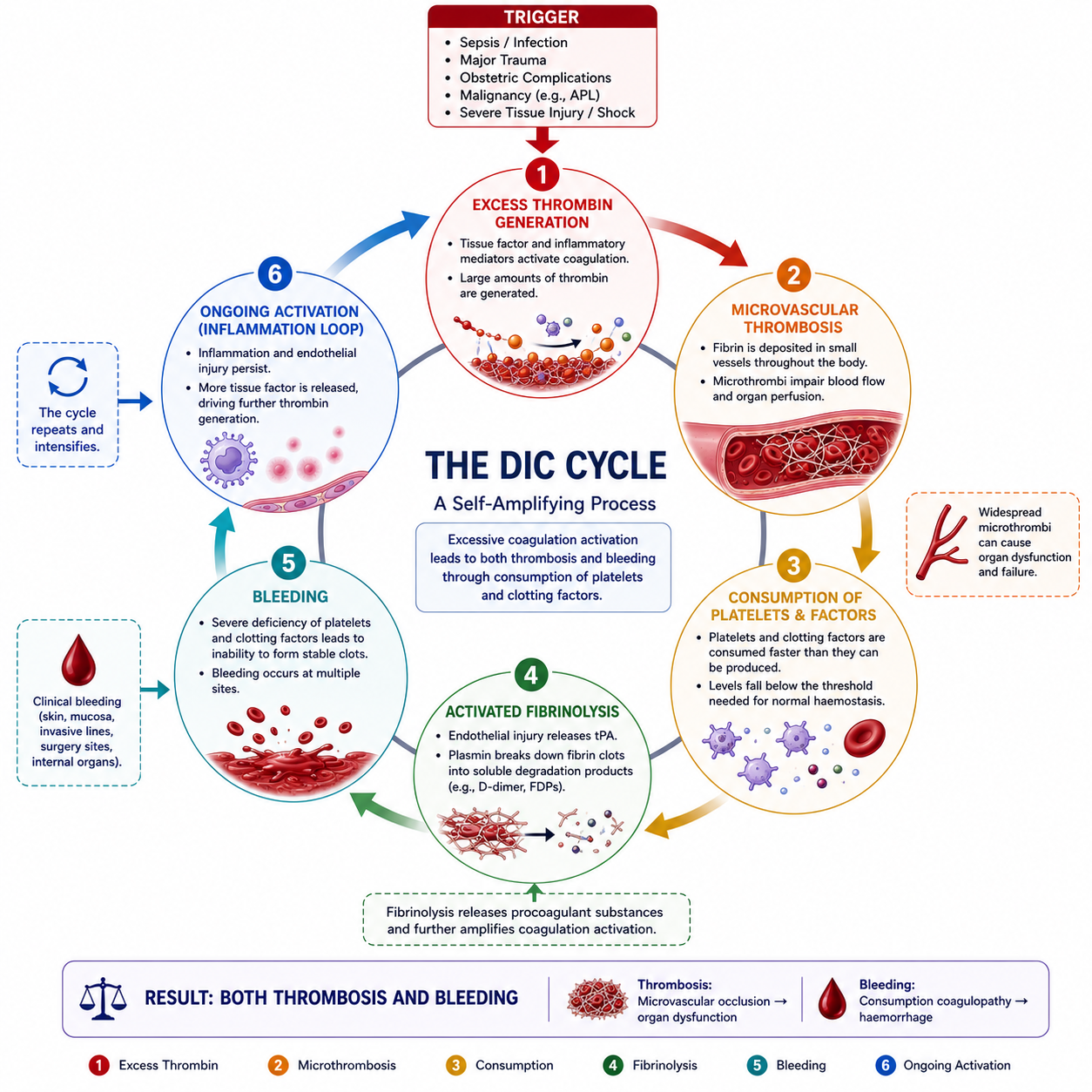
This is the central concept in DIC. The sequence of events explains the apparent paradox:
- 1A trigger causes excessive thrombin generation. Triggers include sepsis, major trauma, obstetric emergencies, and malignancy. Thrombin is the key amplifying enzyme of the coagulation cascade.
- 2Microvascular thrombi form throughout the circulation. Thrombin converts fibrinogen to fibrin, producing widespread microvascular clots that impair organ perfusion.
- 3Platelets are consumed. Platelets are incorporated into the forming microthrombi faster than they can be replaced by the bone marrow, resulting in thrombocytopenia.
- 4Clotting factors are consumed. Fibrinogen and other coagulation factors are depleted during widespread clot formation — a process termed consumptive coagulopathy.
- 5Fibrinolysis becomes activated. The fibrinolytic system is triggered to break down the extensive fibrin deposits, generating fibrin degradation products (FDPs) and D-dimer.
- 6The patient develops bleeding. With platelets depleted and coagulation factors exhausted, the haemostatic system becomes unable to form protective clots at sites of injury — and bleeding results.
DIC is not simply a clotting disorder.
DIC is not simply a bleeding disorder.
DIC is a disorder of uncontrolled coagulation leading to both thrombosis and bleeding.
Common Causes of DIC
DIC is always secondary to an underlying disorder that triggers systemic coagulation activation. The most clinically important causes include:
Sepsis
The most common cause of acute DIC in many clinical settings. Bacterial endotoxins and pro-inflammatory cytokines stimulate massive thrombin generation via tissue factor expression on monocytes and endothelial cells.
Major Trauma
Extensive tissue injury releases large amounts of tissue factor into the circulation, triggering systemic coagulation activation. Traumatic DIC may be further exacerbated by hypothermia and acidosis — the lethal triad of trauma.
Obstetric Emergencies
Several obstetric conditions can trigger DIC, including:
- Placental abruption
- Amniotic fluid embolism
- Retained dead fetus syndrome
- Severe postpartum haemorrhage
- Pre-eclampsia / HELLP syndrome
Malignancy
Particularly acute promyelocytic leukaemia (APL), where granules released from leukaemic cells are powerfully pro-coagulant. Advanced solid tumours can also cause chronic DIC through sustained low-level coagulation activation.
Shock and Severe Tissue Injury
Circulatory collapse, extensive burns, and crushing injuries can all trigger systemic coagulation activation through ischaemic tissue damage and endothelial injury.
| Major Category | Examples |
|---|---|
| Infection | Sepsis (bacterial, viral, fungal) |
| Trauma | Major trauma, burns, crush injury |
| Obstetric | Placental abruption, amniotic fluid embolism, retained dead fetus |
| Malignancy | Acute promyelocytic leukaemia (APL), metastatic cancer |
| Shock | Severe circulatory collapse, anaphylaxis |
In acute promyelocytic leukaemia (APL), the DIC may be more dangerous than the leukaemia itself in the early stages. Urgent recognition and prompt initiation of all-trans retinoic acid (ATRA) therapy can reverse the coagulopathy. APL must always be excluded in any young patient with unexplained DIC and a high white cell count.
Laboratory Findings in DIC
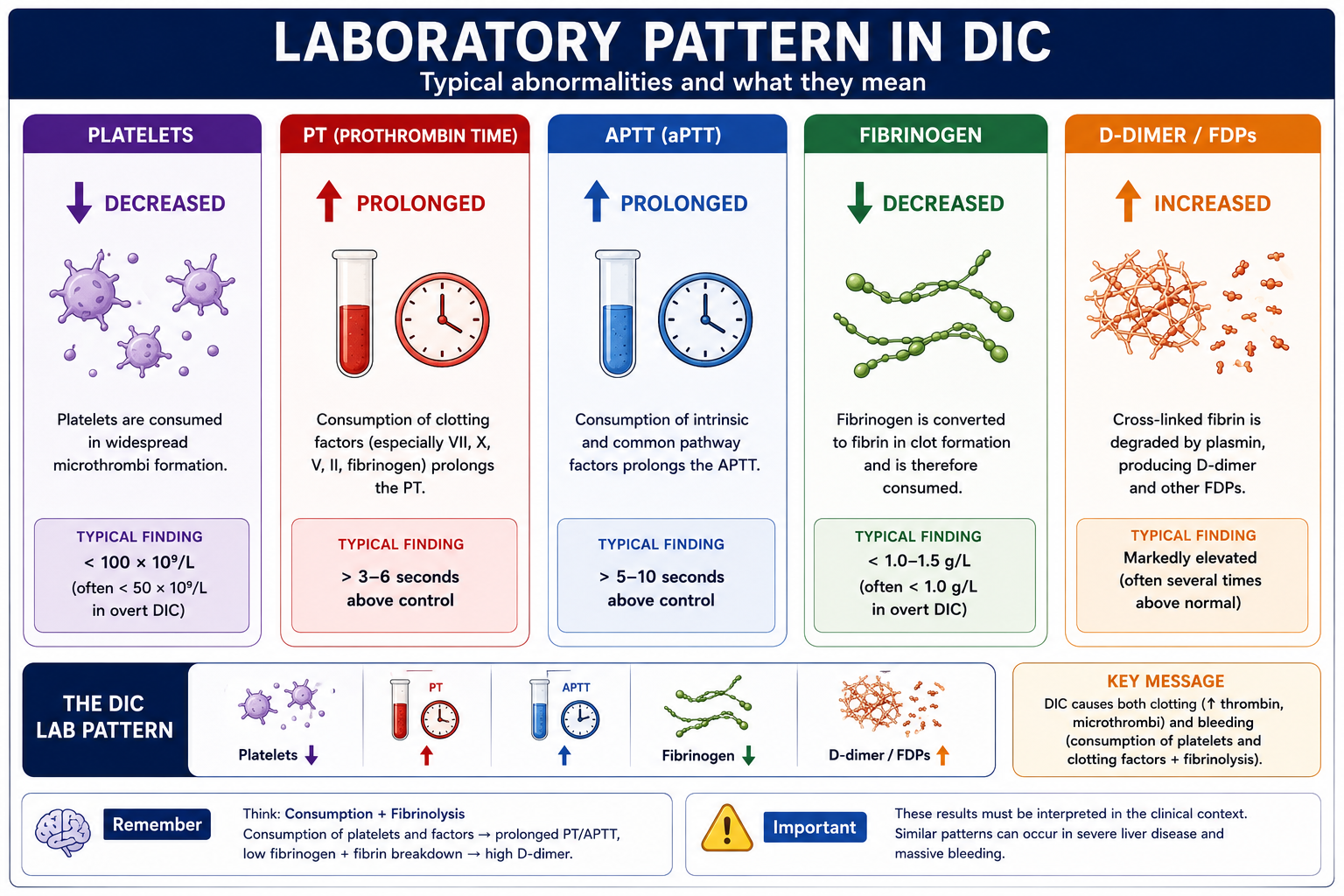
The characteristic laboratory pattern of DIC reflects ongoing coagulation activation, consumption of platelets and clotting factors, and activation of the fibrinolytic system.
Platelet Count
Decreased. Platelets are consumed during widespread clot formation faster than the bone marrow can replace them. Thrombocytopenia is one of the earliest and most consistent findings in DIC.
Prothrombin Time (PT)
Prolonged. The extrinsic and common pathway factors (including fibrinogen, Factor V, Factor X, and Factor II) are consumed during ongoing coagulation, slowing clot formation in the PT assay.
Activated Partial Thromboplastin Time (APTT)
Prolonged. Intrinsic pathway factors are similarly consumed, prolonging APTT alongside PT. Both tests are typically prolonged together in established DIC.
Fibrinogen
Decreased. Fibrinogen is consumed as thrombin converts it to fibrin during widespread clot formation. Low fibrinogen is a hallmark of DIC and is also an important prognostic indicator — very low fibrinogen (<1.0 g/L) contributes significantly to bleeding risk.
D-dimer
Increased. D-dimer is a fibrin degradation product generated when plasmin breaks down cross-linked fibrin. Its elevation confirms that fibrin has been both formed and subsequently broken down — the hallmark of active fibrinolysis in DIC.
| Test | Typical Finding | Mechanism |
|---|---|---|
| Platelet count | ↓ Decreased | Consumption during microthrombus formation |
| PT | ↑ Prolonged | Consumption of extrinsic and common pathway factors |
| APTT | ↑ Prolonged | Consumption of intrinsic and common pathway factors |
| Fibrinogen | ↓ Decreased | Consumed during widespread fibrin formation |
| D-dimer | ↑ Increased | Fibrinolysis generating fibrin degradation products |
| FDPs | ↑ Increased | Breakdown products of fibrin and fibrinogen |
Platelets ↓ — consumed in microthrombi
PT ↑ — factor consumption
APTT ↑ — factor consumption
Fibrinogen ↓ — consumed forming fibrin
D-dimer ↑ — fibrin formation then breakdown
Why Is D-dimer Elevated?
Many students memorise elevated D-dimer as a DIC finding without understanding its origin. The step-by-step process is:
D-dimer therefore indicates that both clot formation and clot breakdown have occurred. It is specific for cross-linked fibrin degradation — which is why it is elevated in DIC but not in pure fibrinogenolysis (where fibrinogen is broken down without first forming a cross-linked clot).
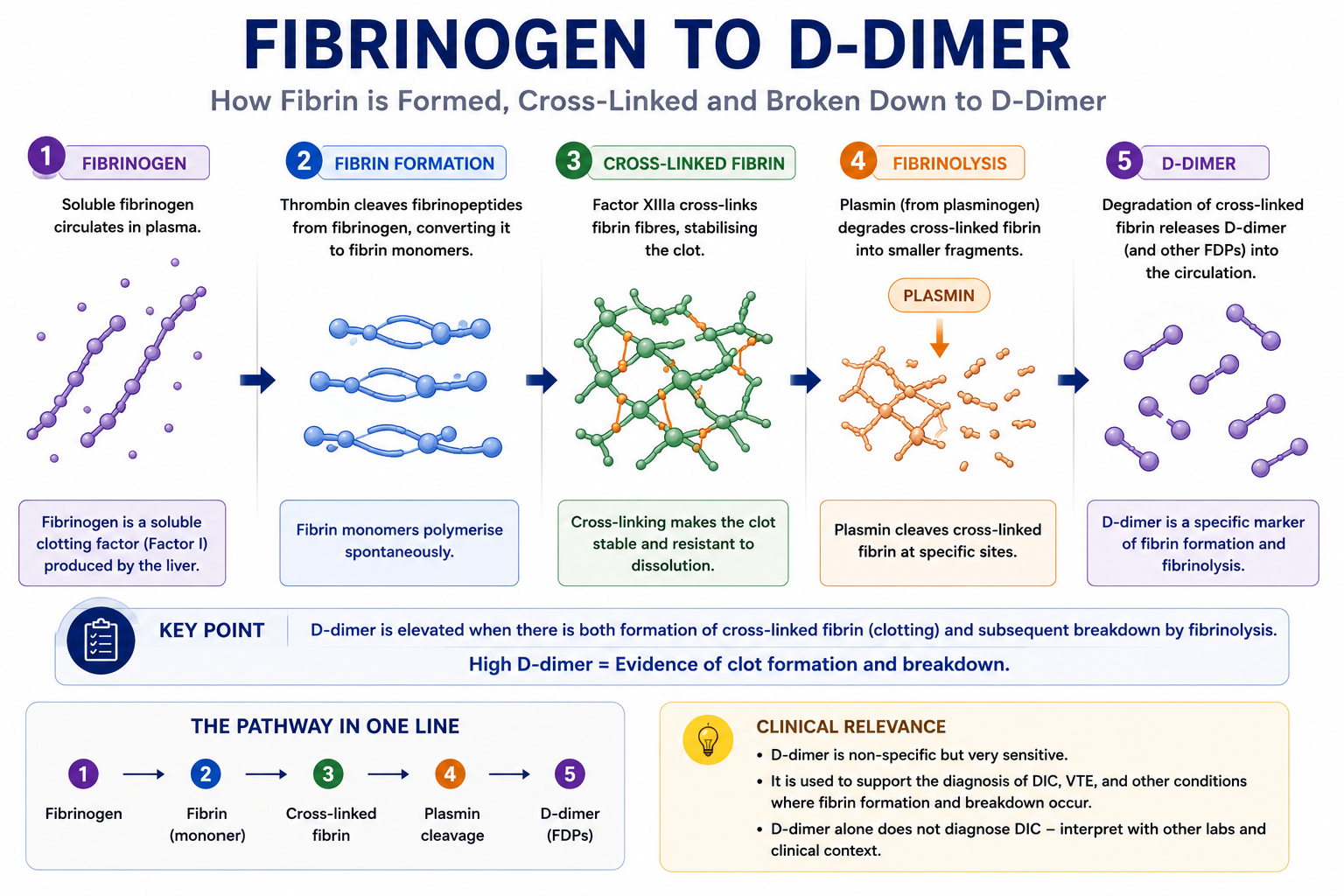
D-dimer is a sensitive but non-specific marker. Many conditions can elevate D-dimer: venous thromboembolism, pregnancy, surgery, trauma, infection, malignancy, and advancing age. A raised D-dimer alone does not diagnose DIC. Diagnosis requires an appropriate clinical context with supporting laboratory findings — and should be scored formally using the ISTH scoring system.
Acute vs Chronic DIC
Not all DIC behaves in the same way. The speed of onset and the ability of the body to compensate differ considerably between acute and chronic presentations.
Acute DIC
Typically triggered by sepsis, major trauma, or obstetric catastrophe. Coagulation is activated rapidly and overwhelms hepatic and bone marrow compensatory capacity.
- Rapid onset with marked factor consumption
- Bleeding is often the dominant clinical presentation
- Laboratory abnormalities are marked and diagnostically clear
- Platelet count, PT, APTT, and fibrinogen all typically show obvious abnormalities
Chronic DIC
Typically associated with malignancy or large aortic aneurysms. Coagulation is activated gradually at a rate that allows partial compensation by the liver (synthesising more clotting factors) and bone marrow (producing more platelets).
- Gradual onset with sustained low-level coagulation activation
- Thrombosis may predominate over bleeding
- Laboratory abnormalities can be subtle or within the normal range
- D-dimer and FDPs are often the most reliably elevated markers
| Feature | Acute DIC | Chronic DIC |
|---|---|---|
| Onset | Rapid | Gradual |
| Common causes | Sepsis, major trauma, obstetric emergencies | Malignancy, large aortic aneurysm |
| Bleeding | Common — often the dominant feature | Less prominent |
| Thrombosis | Present | Often dominant |
| Compensation | Poor — system overwhelmed | Better — partial hepatic and marrow compensation |
| Laboratory abnormalities | Marked | Often milder |
In chronic DIC, fibrinogen may be normal or even elevated (as an acute phase reactant) despite active DIC, because the liver is compensating. D-dimer and FDPs remain elevated even when other markers appear relatively normal. This is why D-dimer and FDPs are the most sensitive markers in chronic DIC.
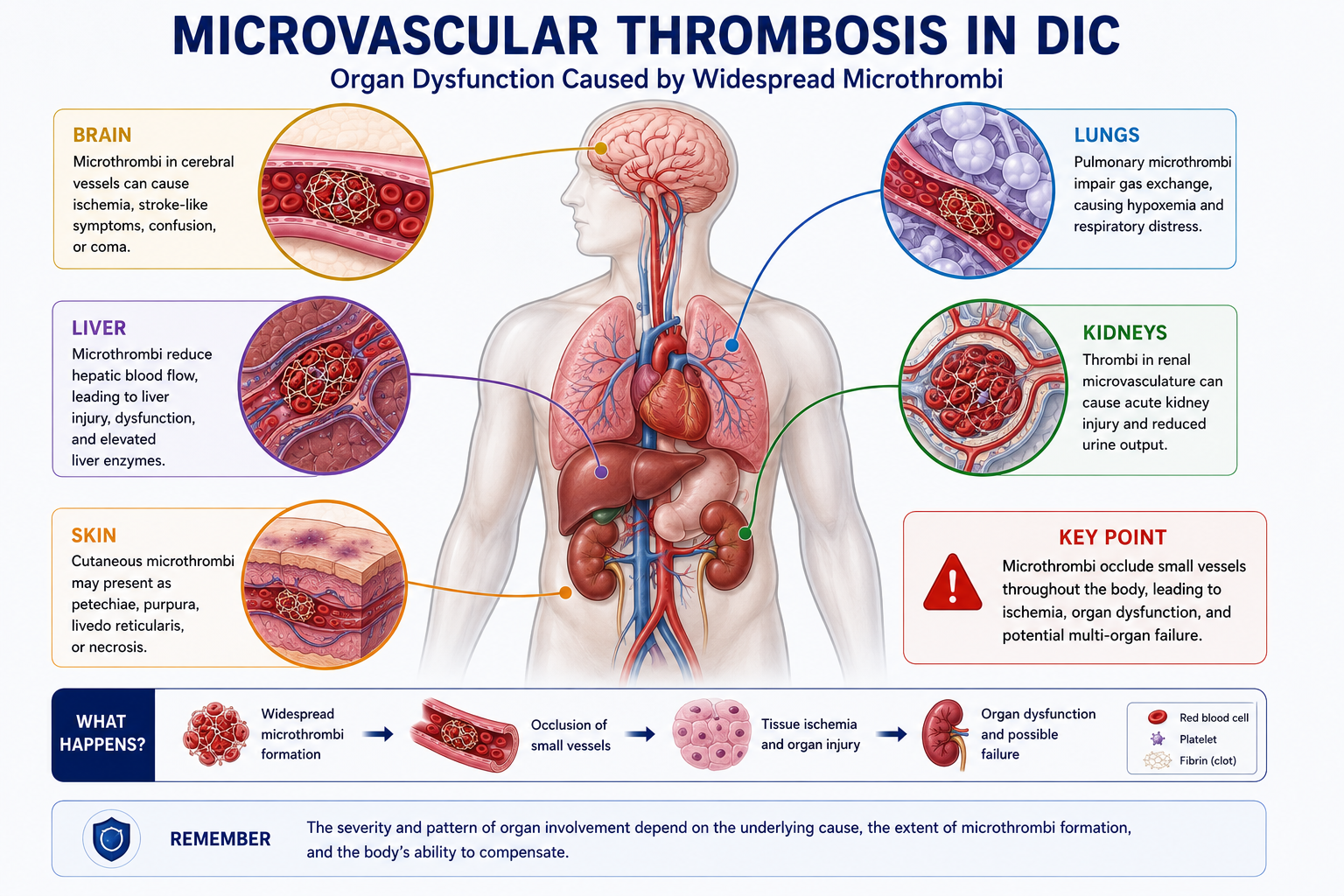
Organ Damage in DIC
Microvascular thrombi may impair blood flow to multiple organs, causing ischaemic dysfunction independent of the bleeding complications. Affected organs may include:
- Kidneys — acute kidney injury from glomerular microthrombi and cortical ischaemia
- Lungs — pulmonary microthrombi may contribute to hypoxia and acute respiratory distress syndrome (ARDS)
- Brain — neurological dysfunction from cerebral microvascular occlusion
- Liver — hepatocellular ischaemia further reduces synthesis of coagulation factors, worsening the coagulopathy
- Skin — purpura fulminans, acral necrosis, and skin infarction from cutaneous microthrombi
Clinical manifestations vary considerably depending on which organs are most severely affected and the pace of the underlying disease.
The ISTH DIC Score
The International Society on Thrombosis and Haemostasis (ISTH) developed a validated scoring system to support the diagnosis of overt DIC. It incorporates four laboratory parameters — each scored based on the degree of abnormality — to generate a total score.
Components of the ISTH Score
The four parameters are: platelet count, D-dimer or fibrin degradation products (FDPs), PT prolongation, and fibrinogen level.
| Parameter | Finding | Points |
|---|---|---|
| Platelets (×10⁹/L) | >100 | 0 |
| 50–100 | 1 | |
| <50 | 2 | |
| D-dimer / FDP | No increase | 0 |
| Moderate increase | 2 | |
| Strong increase | 3 | |
| PT prolongation | <3 seconds | 0 |
| 3–6 seconds | 1 | |
| >6 seconds | 2 | |
| Fibrinogen | >1.0 g/L | 0 |
| ≤1.0 g/L | 1 |
Interpretation
A score of 5 or above is compatible with overt DIC. In this setting, DIC is likely to be clinically significant and treatment of the underlying trigger is the priority, supported by haematological management of the coagulopathy.
A score below 5 does not exclude DIC, particularly early or chronic forms. Serial scoring over time may be more informative than a single measurement. In non-overt DIC, treatment is directed at the underlying condition while monitoring the coagulation profile closely.
The ISTH score does not replace clinical judgement. DIC must always be diagnosed within the context of an underlying disease capable of triggering systemic coagulation activation. A score of ≥5 in a patient with no plausible trigger should prompt reconsideration of the diagnosis.
Common Misconceptions
False. Microvascular thrombosis is a fundamental and early component of DIC pathophysiology. Organ damage from microthrombi can occur even before bleeding becomes clinically apparent. Treating only the bleeding without addressing the underlying pro-coagulant state may be insufficient.
False. Consumption of platelets and coagulation factors, combined with activation of fibrinolysis, results in a bleeding tendency that may be profound. DIC simultaneously drives both thrombosis and haemorrhage — which is precisely what makes it so challenging to manage.
False. Early or mild DIC may show only subtle laboratory abnormalities. In chronic DIC, hepatic compensation may keep PT near normal. Serial monitoring of the full panel — including D-dimer, fibrinogen, and platelet count — is required rather than relying on any single test.
False. D-dimer is sensitive but non-specific. It is elevated in venous thromboembolism, pregnancy, surgery, trauma, infection, malignancy, and with increasing age. DIC requires an appropriate clinical context and a supporting pattern of laboratory abnormalities — not a single elevated D-dimer in isolation.
Exam Tips
DIC = Consumptive coagulopathy
Platelets ↓
PT ↑
APTT ↑
Fibrinogen ↓
D-dimer ↑
Microthrombi + bleeding
ISTH score ≥5 = overt DIC
- DIC = consumptive coagulopathy — this single phrase captures the pathophysiology.
- Both PT and APTT prolonged in DIC — unlike haemophilia, which causes isolated APTT prolongation.
- D-dimer elevated + fibrinogen low = fibrin formed and broken down — the signature of active DIC.
- Sepsis is the most common cause of acute DIC in clinical practice.
- APL causes DIC — always exclude APL in unexplained DIC with leukaemia; treat urgently with ATRA.
- Chronic DIC may have normal fibrinogen (acute phase reactant compensates) — D-dimer is more sensitive.
- Acute DIC → bleeding predominates; Chronic DIC → thrombosis often predominates.
- ISTH score ≥5 = overt DIC — four parameters: platelets, D-dimer/FDP, PT prolongation, fibrinogen.
- Microthrombi cause organ damage — kidneys, lungs, brain, liver, and skin are all at risk.
Frequently Asked Questions
Key Takeaways
- DIC is a consumptive coagulopathy
- Clotting and bleeding occur simultaneously
- Microvascular thrombosis is central to the pathophysiology
- Platelet count decreases
- PT and APTT become prolonged
- Fibrinogen decreases
- D-dimer increases
- Acute and chronic DIC differ clinically — acute presents with bleeding; chronic often presents with thrombosis
- ISTH score ≥5 supports the diagnosis of overt DIC
References
- Levi M, Ten Cate H. Disseminated intravascular coagulation. N Engl J Med. 1999;341(8):586–592.
- Levi M, Toh CH, Thachil J, Watson HG. Guidelines for the diagnosis and management of disseminated intravascular coagulation. Br J Haematol. 2009;145(1):24–33.
- Taylor FB Jr, Toh CH, Hoots WK, Wada H, Levi M. Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb Haemost. 2001;86(5):1327–1330.
- Bain BJ, Bates I, Laffan MA, eds. Dacie and Lewis Practical Haematology. 12th ed. London: Elsevier; 2017.
- Wada H, Matsumoto T, Yamashita Y. Diagnosis and treatment of disseminated intravascular coagulation (DIC) according to four DIC guidelines. J Intensive Care. 2014;2(1):15.
- Gando S, Levi M, Toh CH. Disseminated intravascular coagulation. Nat Rev Dis Primers. 2016;2:16037.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist haematological input when investigating and managing suspected DIC.