Ascites is the abnormal accumulation of fluid within the peritoneal cavity. It is one of the most important complications of portal hypertension and cirrhosis, and often represents the transition from compensated to decompensated liver disease.
Understanding ascites requires understanding portal hypertension, splanchnic vasodilation, neurohormonal activation, and sodium retention. These four concepts together explain why fluid accumulates — and why simply restricting water is not the correct approach to management.
This article builds directly on Portal Hypertension Explained. Read it first if you are new to liver disease. Ascites Explained also sets up the subsequent articles on SAAG, Spontaneous Bacterial Peritonitis, and Hepatorenal Syndrome.
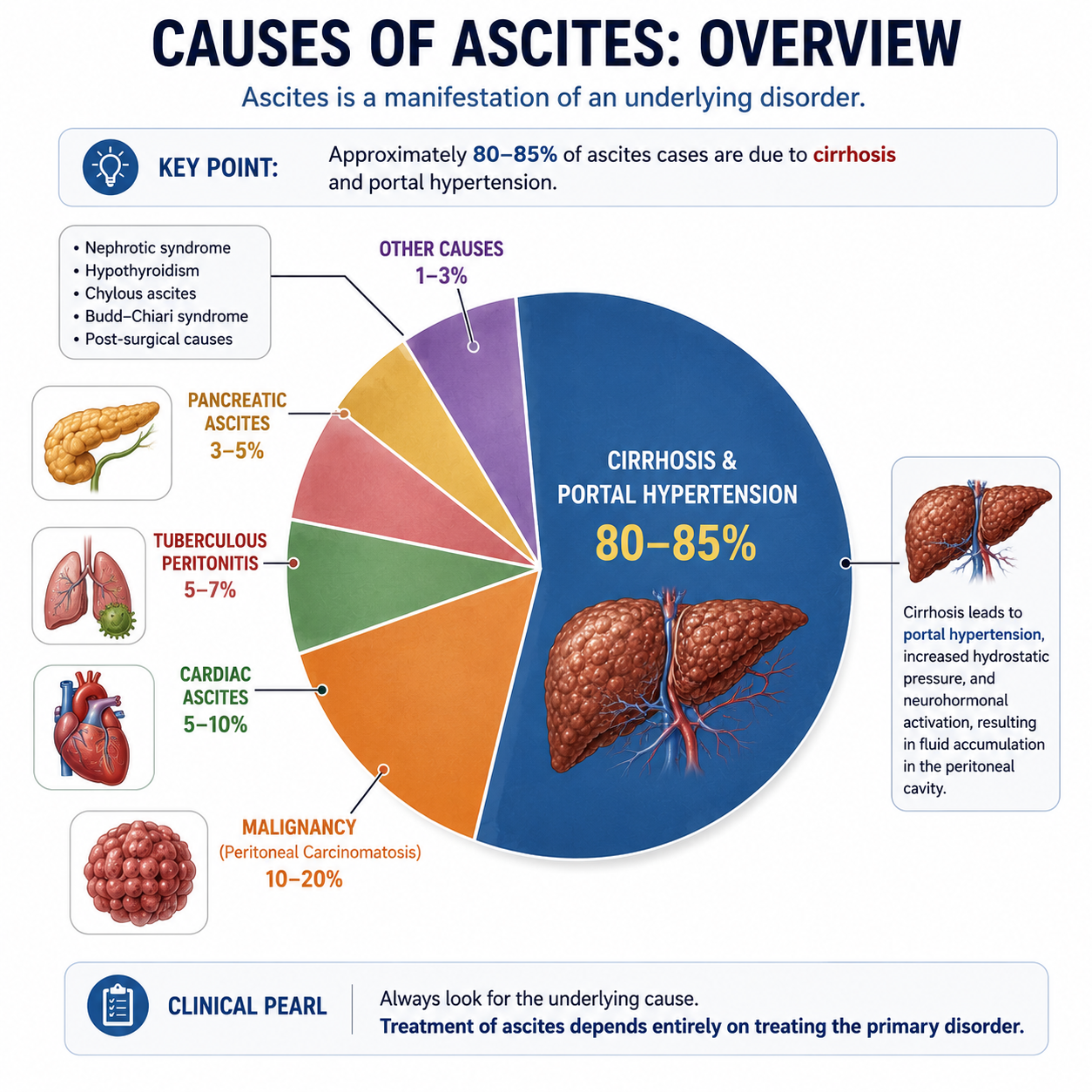
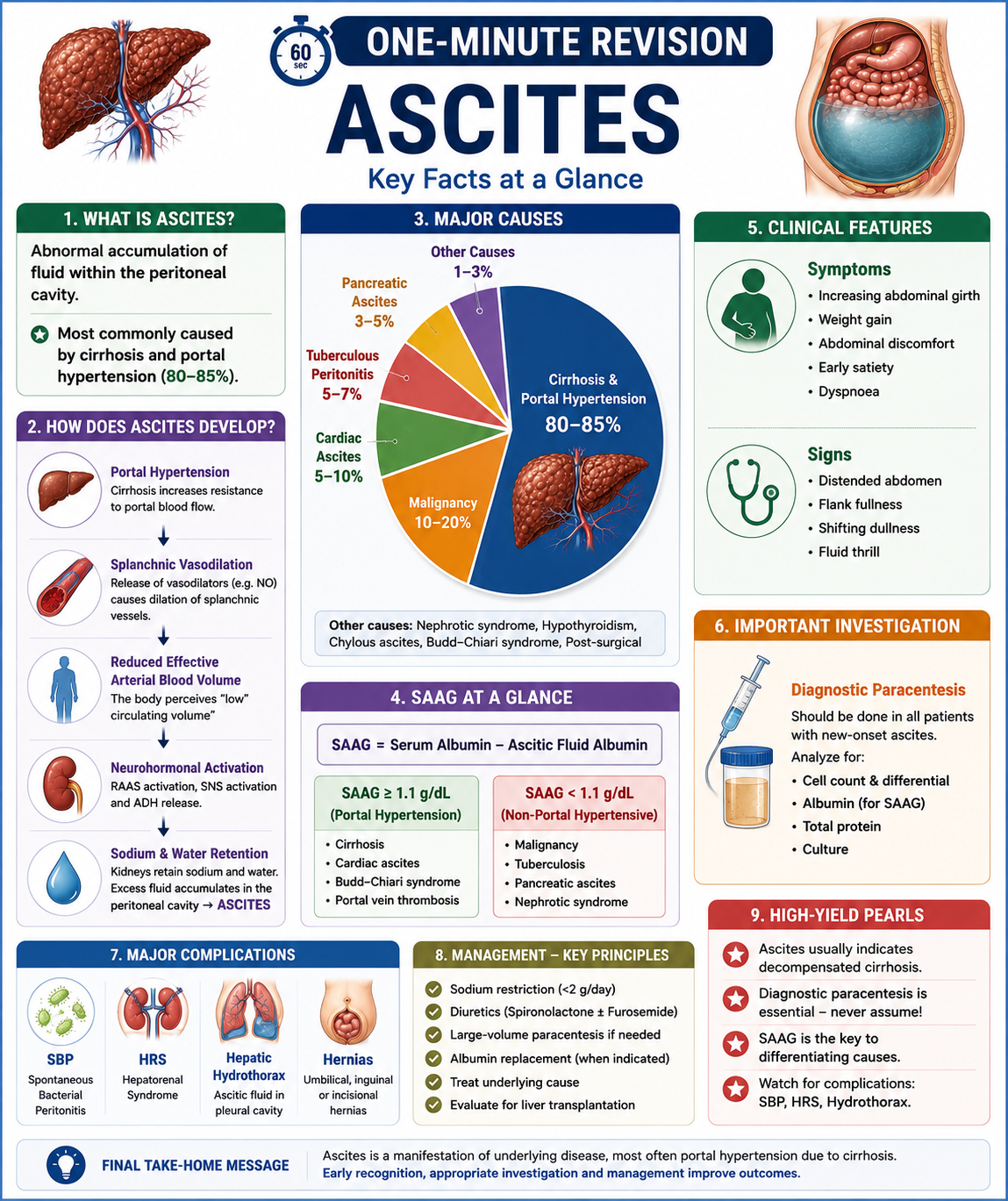
Approximately 80–85% of ascites cases are caused by cirrhosis and portal hypertension.
Learning Objectives
- Define ascites and its clinical significance
- Explain the four-step pathophysiology of ascites in portal hypertension
- Understand the role of RAAS, ADH, and sodium retention
- List the major causes of ascites
- Describe the clinical features and examination signs of ascites
- Explain the role of diagnostic paracentesis
- Interpret SAAG and understand its clinical use
- Recognise the major complications of ascites
What Is Ascites?
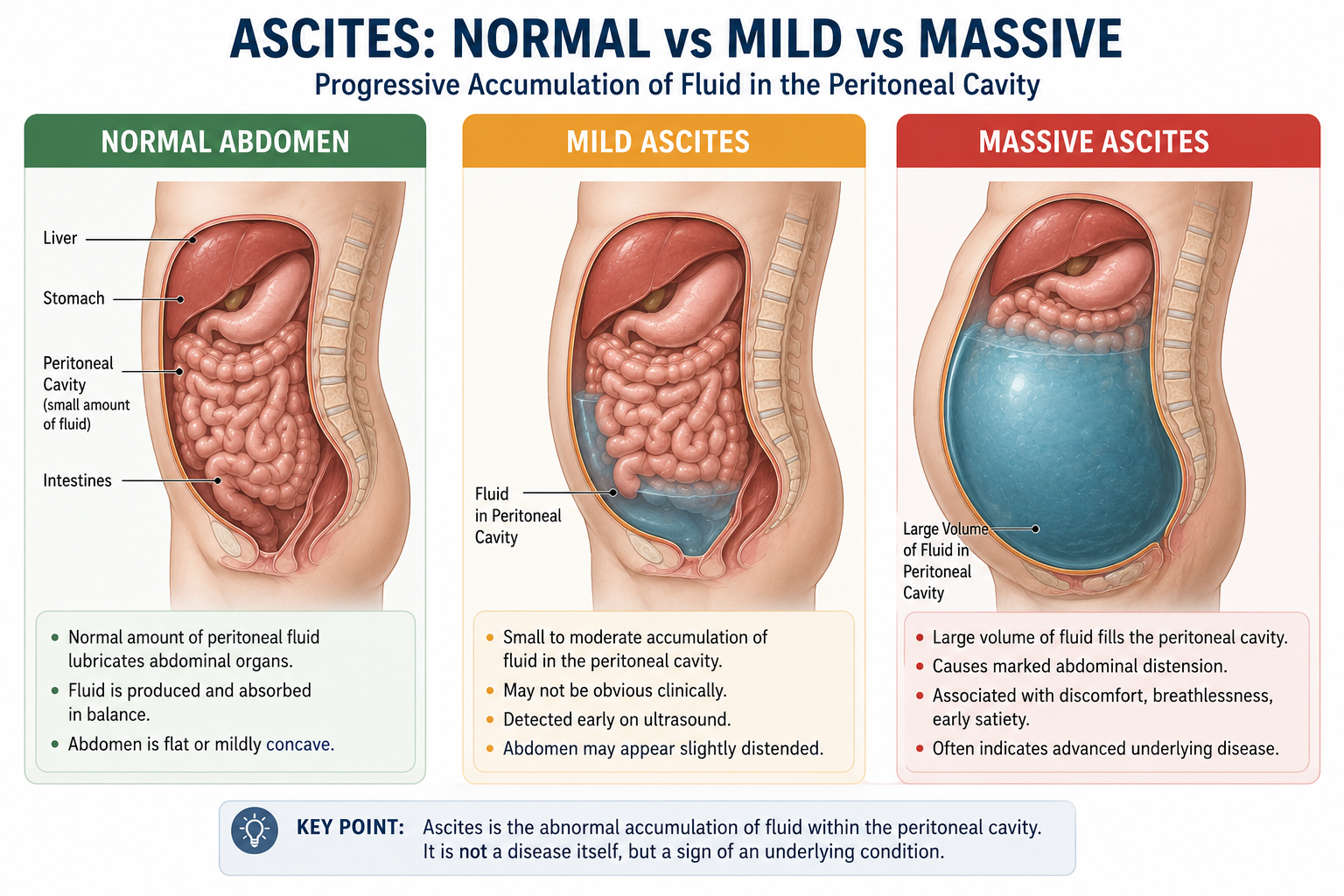
Ascites refers to the pathological accumulation of fluid within the peritoneal cavity. Small amounts of peritoneal fluid are normally present to lubricate abdominal organs. When fluid production exceeds fluid removal, clinically detectable ascites develops.
Ascites is not a disease in itself. Rather, it is a manifestation of an underlying disorder — most commonly advanced liver disease with portal hypertension.
Why Is Ascites Important?
Development of ascites is a major milestone in chronic liver disease. It usually indicates that the disease has progressed from compensated to decompensated cirrhosis.
The appearance of ascites is associated with:
- Transition to decompensated cirrhosis
- Increased risk of spontaneous bacterial peritonitis (SBP)
- Increased risk of hepatorenal syndrome (HRS)
- Significantly reduced long-term survival
Ascites usually marks the transition from compensated cirrhosis to decompensated cirrhosis. Decompensation also includes variceal bleeding, hepatic encephalopathy, and jaundice. Once a patient decompensates, prognosis worsens significantly and liver transplantation assessment becomes relevant.
How Does Ascites Develop?
The pathophysiology of ascites is best understood as a four-step cascade. Each step follows logically from the one before it.
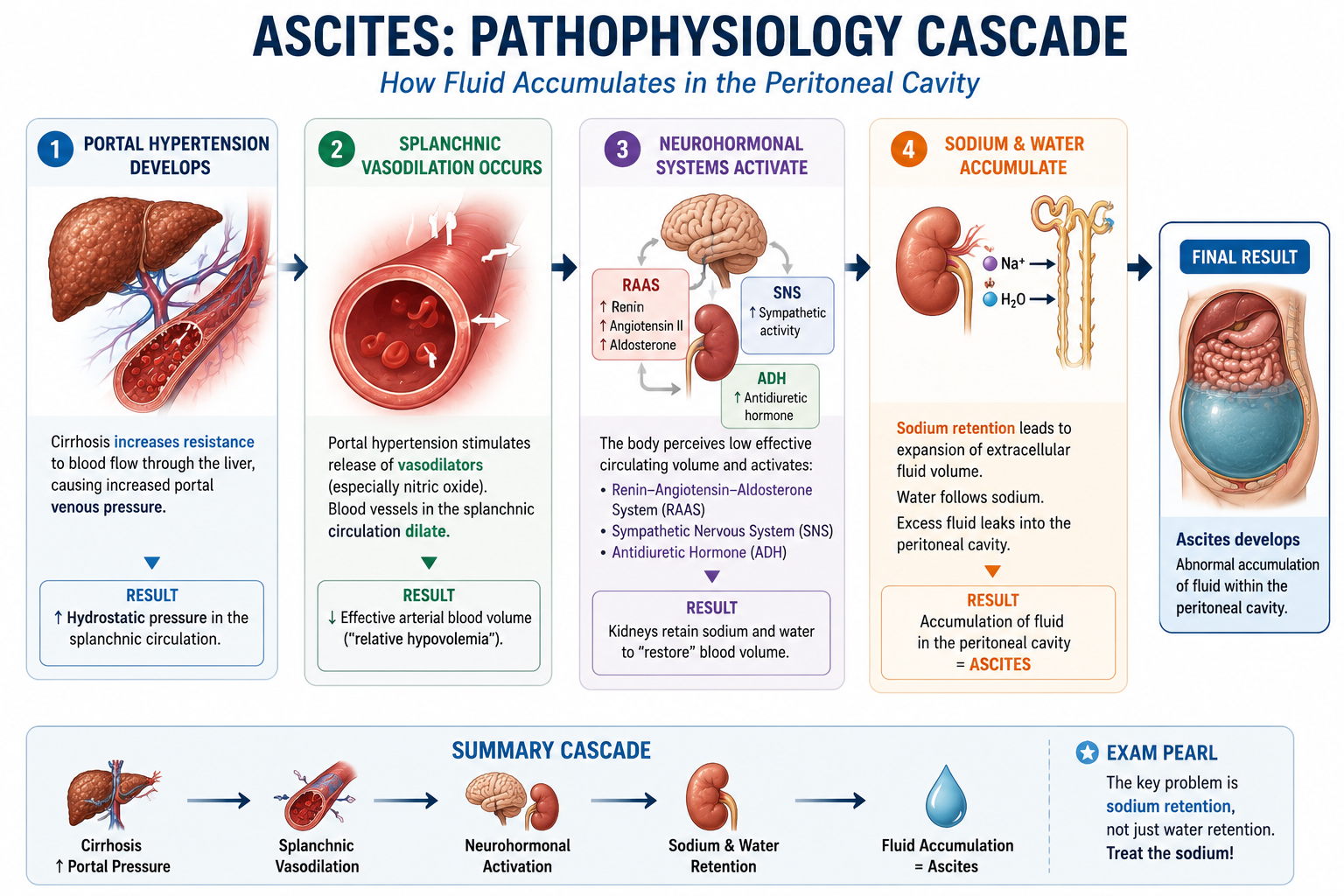
Step 1: Portal Hypertension Develops
Cirrhosis increases resistance to blood flow through the liver. As blood struggles to pass through the fibrosed, nodular liver, portal venous pressure rises.
This increased hydrostatic pressure in the portal and mesenteric venous system promotes movement of fluid from blood vessels into surrounding tissues and the peritoneal cavity.
Additional Factor: Hypoalbuminaemia Reduces Oncotic Pressure
In cirrhosis, reduced hepatic synthetic function may lower serum albumin. Albumin normally helps retain fluid within the vascular compartment by maintaining plasma oncotic pressure.
When albumin is low, oncotic pressure falls. This makes it easier for fluid to leave the vascular space and enter the interstitial and peritoneal spaces.
However, hypoalbuminaemia alone does not fully explain cirrhotic ascites. The dominant mechanisms are portal hypertension, splanchnic vasodilation, neurohormonal activation, and renal sodium retention.
Do not explain ascites only as "low albumin causing fluid leakage." In cirrhosis, ascites is mainly a haemodynamic and renal sodium-retention problem. Hypoalbuminaemia contributes, but portal hypertension and RAAS activation are central.
Step 2: Splanchnic Vasodilation Occurs
Portal hypertension stimulates release of vasodilators — particularly nitric oxide — from the mesenteric and splanchnic vascular endothelium. Blood vessels supplying the abdominal organs become dilated.
Although total blood volume is normal or even increased, the vasodilated splanchnic bed sequester a large proportion of circulating volume. Effective arterial blood volume — the volume actually perfusing vital organs — becomes reduced. The body interprets this as relative hypovolaemia.
Step 3: Neurohormonal Systems Activate
To compensate for perceived hypovolaemia, three major neurohormonal systems activate simultaneously.
- ARenin-Angiotensin-Aldosterone System (RAAS) — Reduced renal perfusion pressure triggers renin release from the kidneys. Renin converts angiotensinogen to angiotensin I, which is converted to angiotensin II. Angiotensin II stimulates aldosterone release from the adrenal cortex. Aldosterone promotes renal sodium retention in the distal nephron.
- BSympathetic Nervous System — Activation causes systemic vasoconstriction and further promotes renal sodium and water conservation by reducing renal blood flow and increasing tubular reabsorption.
- CAntidiuretic Hormone (ADH) — Released from the posterior pituitary in response to perceived low effective circulating volume. ADH promotes free water reabsorption in the renal collecting ducts, contributing to dilutional hyponatraemia in advanced disease.
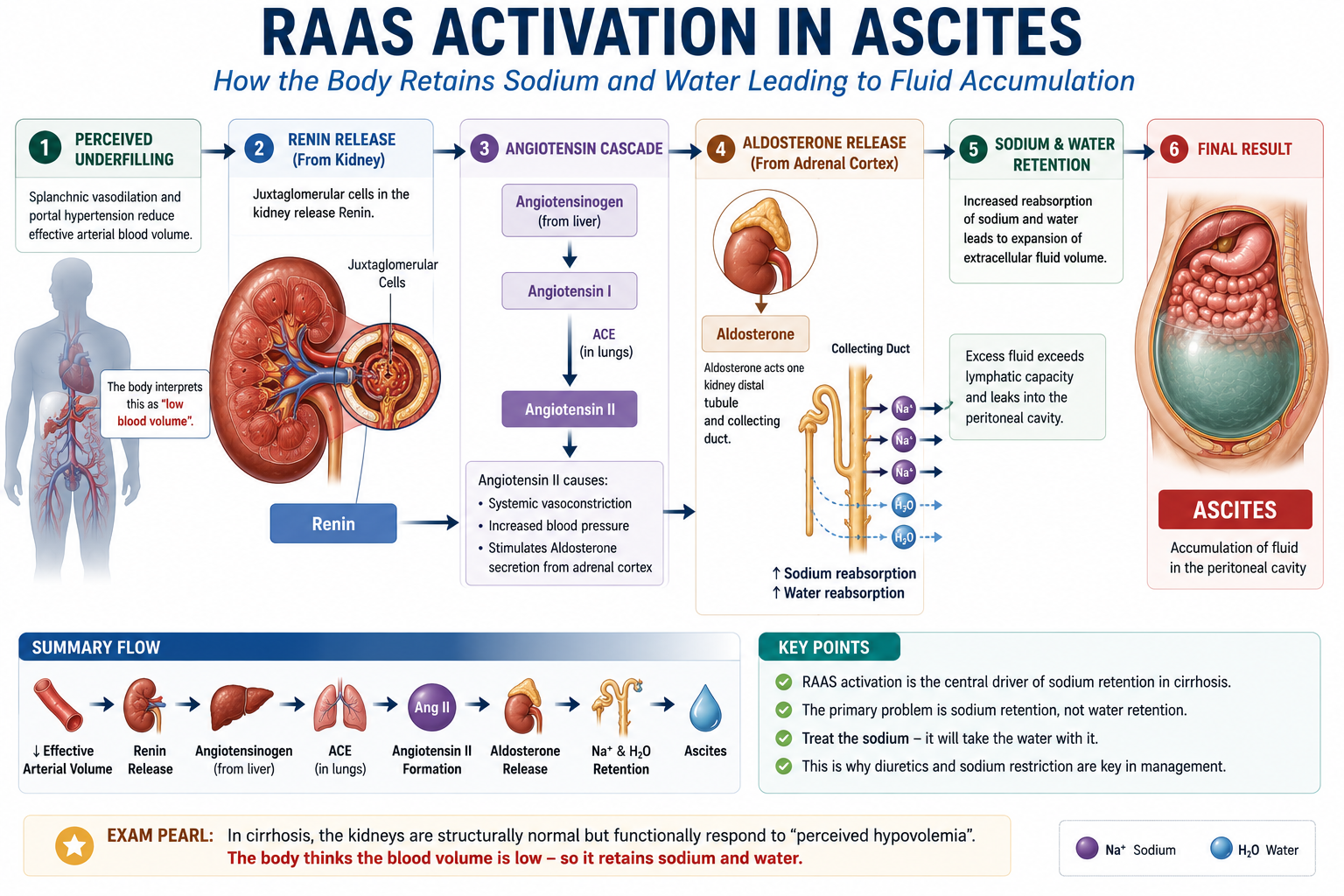
Step 4: Sodium and Water Accumulate
Retention of sodium by aldosterone leads to expansion of the extracellular fluid volume. Water follows sodium osmotically. However, rather than restoring effective arterial volume (because the underlying splanchnic vasodilation persists), the retained fluid leaks into the peritoneal cavity via the portal hypertensive capillary bed.
Ascites develops and accumulates as this cycle continues.
The primary physiological abnormality in cirrhotic ascites is sodium retention — not isolated water retention. This is why sodium restriction and diuretics targeting aldosterone (e.g. spironolactone) are the cornerstones of management, not simple fluid restriction. Restricting fluid without addressing sodium balance will not resolve ascites.
What Causes Ascites?
Although cirrhosis is responsible for approximately 80–85% of cases, ascites may arise from several other conditions. Understanding the non-cirrhotic causes is important both clinically and for examinations.
| Cause | Mechanism | Key Feature |
|---|---|---|
| Cirrhosis | Portal hypertension, RAAS activation, sodium retention | Most common — 80–85% of cases |
| Malignancy | Peritoneal deposits, lymphatic obstruction, hepatic metastases | Low SAAG; ovarian, gastric, pancreatic cancers |
| Heart failure | Raised venous back-pressure, secondary RAAS activation | High SAAG; peripheral oedema, raised JVP |
| Tuberculous peritonitis | Peritoneal inflammation and lymphatic obstruction | Low SAAG; endemic regions |
| Pancreatic ascites | Leakage of pancreatic secretions into the peritoneal cavity | High amylase in ascitic fluid |
Always consider non-cirrhotic causes when ascitic fluid analysis suggests a non-portal hypertensive aetiology (SAAG <1.1 g/dL). Malignancy and tuberculous peritonitis are the most important non-cirrhotic diagnoses to exclude.
Clinical Features of Ascites
Symptoms and signs depend on the volume of fluid accumulated. Small volumes may be clinically undetectable; large volumes produce florid abdominal findings.
Symptoms
- Increasing abdominal girth and weight gain
- Abdominal discomfort or pressure
- Early satiety from diaphragmatic splinting
- Dyspnoea from raised intra-abdominal pressure and diaphragmatic elevation
Signs
- Distended abdomen — generalised fullness
- Flank fullness — dullness at the flanks on percussion
- Shifting dullness — dullness shifts as the patient rolls to the side; the most sensitive clinical sign
- Fluid thrill — detectable when ascites is massive; tap one flank and feel a fluid impulse transmitted across the abdomen
- Shifting dullness — the most sensitive physical examination sign for ascites
- Fluid thrill — present only in massive (large-volume) ascites
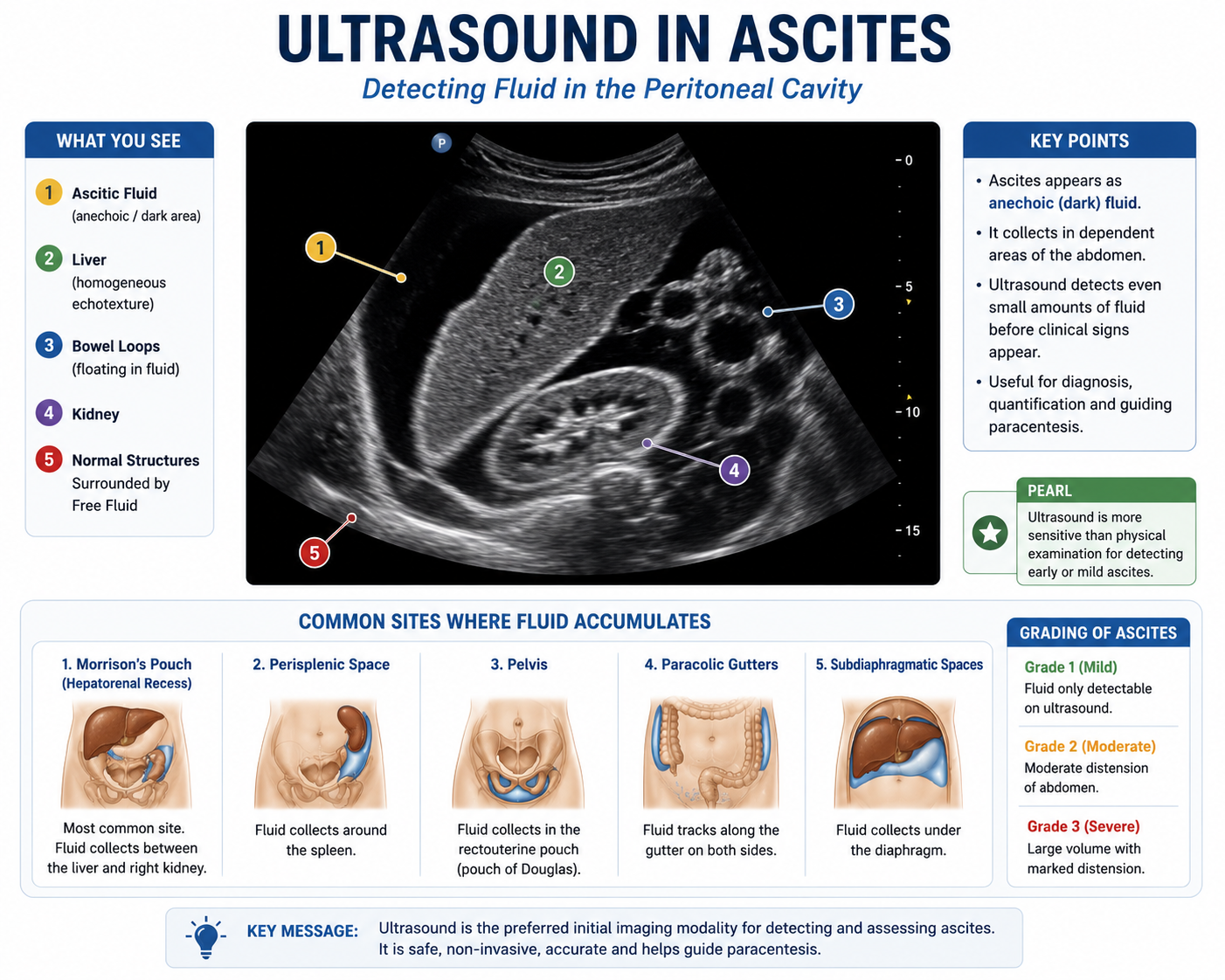
- Ultrasound detects ascites earlier and more sensitively than clinical examination
Grading of Ascites
Ascites is commonly graded clinically according to volume and detectability. Grading guides management decisions — particularly when to proceed to large-volume paracentesis.
| Grade | Description | Clinical Findings |
|---|---|---|
| Grade 1 | Mild ascites | Detectable only by ultrasound; no clinical signs |
| Grade 2 | Moderate ascites | Symmetrical abdominal distension; shifting dullness present |
| Grade 3 | Large / tense ascites | Marked abdominal distension; patient often uncomfortable or breathless |
Grade 1 ascites may not be detected clinically — it is identified only on ultrasound. This is why ultrasound is more sensitive than physical examination for diagnosing ascites in early liver disease.
How Is Ascites Diagnosed?
Clinical Examination
History and physical examination remain the first step. Flank fullness and shifting dullness are the most reliable clinical signs.
Abdominal Ultrasound
Ultrasound is the investigation of first choice. It detects even small volumes of ascitic fluid before they become clinically apparent, and can visualise the liver, spleen, and portal vasculature simultaneously. It also guides paracentesis safely.
Diagnostic Paracentesis
Every patient with new-onset ascites should undergo diagnostic paracentesis unless contraindicated. Analysis of ascitic fluid is essential to determine the cause and exclude infection.
The fluid should be analysed for:
- Cell count and differential — to detect spontaneous bacterial peritonitis (neutrophil count ≥250 cells/mm³)
- Albumin — to calculate SAAG
- Protein — to classify exudate vs. transudate (though SAAG is now preferred)
- Culture and sensitivity — even if cell count is not elevated
Never assume ascites is uncomplicated cirrhotic ascites without ascitic fluid analysis. Spontaneous bacterial peritonitis can be present with minimal clinical signs. An unexplained deterioration in a cirrhotic patient with ascites should always prompt diagnostic paracentesis.
Introduction to SAAG
The Serum-Ascites Albumin Gradient (SAAG) is one of the most clinically useful tools in ascites evaluation. It helps determine whether portal hypertension is the underlying cause.
SAAG = Serum Albumin − Ascitic Fluid Albumin
Both samples must be taken on the same day. The result in g/dL reflects the oncotic-hydrostatic pressure balance across the portal capillary membrane.
SAAG ≥ 1.1 g/dL — Portal Hypertension
A high SAAG indicates that portal hypertension is driving fluid accumulation. High portal pressure forces fluid with relatively low protein content into the peritoneal cavity, creating a large gradient between serum and ascitic albumin.
- Cirrhosis
- Cardiac ascites (heart failure, constrictive pericarditis)
- Budd–Chiari syndrome
SAAG < 1.1 g/dL — Non-Portal Hypertensive
A low SAAG suggests fluid is accumulating through mechanisms other than raised portal pressure — typically peritoneal disease or lymphatic obstruction producing protein-rich fluid.
- Peritoneal malignancy
- Tuberculous peritonitis
- Pancreatic ascites
- Nephrotic syndrome
| SAAG | Mechanism | Examples |
|---|---|---|
| ≥ 1.1 g/dL | Portal hypertension | Cirrhosis, cardiac failure, Budd–Chiari |
| < 1.1 g/dL | Non-portal hypertensive | Malignancy, tuberculosis, pancreatic ascites |
A dedicated SAAG Explained article follows with a deeper exploration of ascitic fluid interpretation, SAAG worked examples, protein-based grading, and step-by-step ascitic fluid analysis.
Major Complications of Ascites
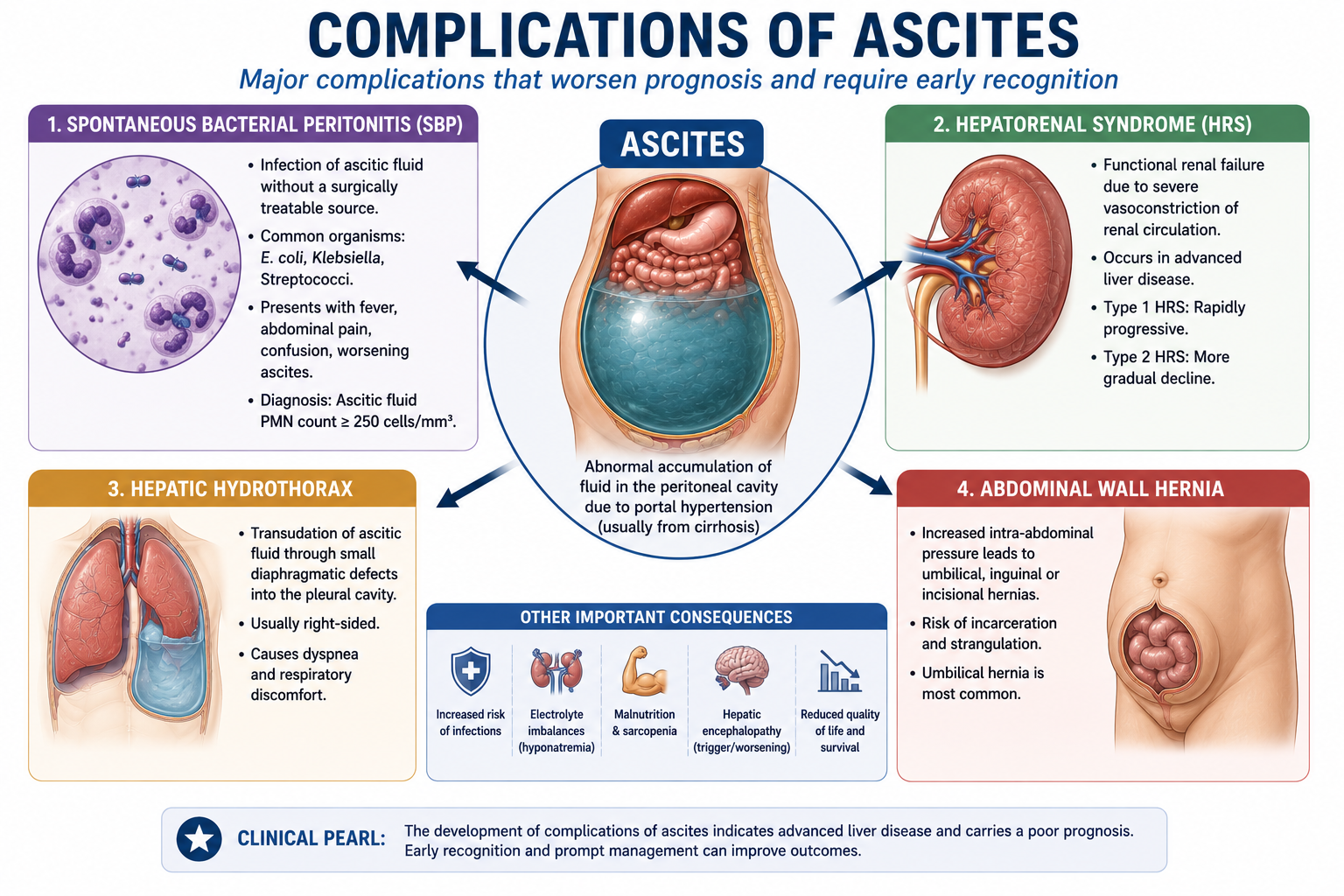
Spontaneous Bacterial Peritonitis (SBP)
Infection of ascitic fluid without a surgically treatable intra-abdominal source. Diagnosis is made when the ascitic fluid neutrophil count reaches ≥250 cells/mm³. SBP is potentially life-threatening and must be excluded in any patient with ascites who develops fever, abdominal pain, or unexplained deterioration.
Hepatorenal Syndrome (HRS)
Functional renal failure occurring in the setting of advanced liver disease and ascites. HRS develops because extreme splanchnic vasodilation and RAAS activation cause intense renal vasoconstriction, reducing GFR. The kidneys themselves are structurally normal — the disorder is haemodynamic. HRS carries a very poor prognosis without liver transplantation.
Hepatorenal syndrome can be understood as an extreme continuation of the same circulatory problem that produces ascites. Progressive splanchnic vasodilation reduces effective arterial blood volume, causing intense RAAS and sympathetic activation. Eventually renal vasoconstriction becomes severe enough to reduce GFR, even though the kidneys are structurally normal.
Hepatic Hydrothorax
Ascitic fluid passes through small diaphragmatic defects into the pleural cavity — most commonly the right side. Patients develop a pleural effusion without underlying cardiac or pulmonary disease. Hepatic hydrothorax may cause significant dyspnoea and is difficult to manage.
Umbilical Hernias
Increased intra-abdominal pressure from tense ascites predisposes to umbilical herniation. Umbilical hernias in cirrhotic patients carry a significant risk of incarceration and skin breakdown, and surgical repair has high perioperative risk.
Management Overview
Detailed management is beyond the scope of this introductory article. The key principles reflect the underlying pathophysiology:
- Sodium restriction — target <88 mmol/day (2 g/day sodium). This addresses the primary physiological problem of sodium retention.
- Diuretics — spironolactone (aldosterone antagonist) is first-line, targeting the RAAS activation. Furosemide is often added for additional diuresis.
- Large-volume paracentesis (LVP) — used for tense or refractory ascites. Albumin infusion is given alongside LVP to prevent post-paracentesis circulatory dysfunction (PPCD).
- Albumin replacement — when indicated (e.g. after LVP, or in SBP treatment to reduce HRS risk).
- Transjugular intrahepatic portosystemic shunt (TIPS) — for refractory ascites, reduces portal pressure directly.
Refractory ascites is ascites that cannot be mobilised, or that recurs rapidly after therapeutic paracentesis, despite appropriate sodium restriction and maximal tolerated diuretic therapy.
It indicates advanced decompensated cirrhosis and poor prognosis. Patients with refractory ascites should be considered for liver transplantation assessment, and selected patients may benefit from TIPS.
- Management of underlying disease — treating the cause of cirrhosis where possible (e.g. abstinence from alcohol, antiviral therapy for hepatitis B/C).
- Liver transplantation assessment — ascites indicates decompensation and should prompt transplant referral assessment.
Student Memory Table
| Finding | Key Association |
|---|---|
| Ascites + Cirrhosis | Portal hypertension — SAAG ≥1.1 |
| Ascites + Fever / Abdominal pain | Spontaneous Bacterial Peritonitis (SBP) |
| Ascites + Rising creatinine | Hepatorenal Syndrome (HRS) |
| Ascites + Right-sided pleural effusion | Hepatic hydrothorax |
| Ascites + Low SAAG (<1.1) | Malignancy or Tuberculosis |
| Ascites + High SAAG + raised JVP | Cardiac ascites (heart failure) |
| Ascites + High ascitic amylase | Pancreatic ascites |
Exam Tips
Most common cause = cirrhosis (80–85%)
Key mechanism = portal hypertension → splanchnic vasodilation → RAAS + ADH → sodium retention
Shifting dullness = most sensitive sign
Fluid thrill = massive ascites only
SAAG ≥1.1 = portal hypertension
SAAG <1.1 = malignancy / TB / pancreatic
Neutrophils ≥250/mm³ in ascitic fluid = SBP
- Always do diagnostic paracentesis in new-onset ascites — don't assume it's cirrhotic.
- SAAG ≥1.1 = portal hypertension — cirrhosis, cardiac failure, Budd–Chiari.
- SAAG <1.1 = non-portal — malignancy, TB, pancreatic.
- SBP diagnosis = neutrophil count ≥250/mm³ in ascitic fluid.
- Spironolactone is first-line because it blocks aldosterone, which is the key driver of sodium retention.
- Fluid restriction is NOT the primary treatment — sodium restriction and diuretics are.
- Ascites = decompensated cirrhosis — begin transplant assessment.
One-Minute Ascites Revision
Use this summary as a rapid pre-examination revision aid.
Key Takeaways
- Ascites is abnormal fluid accumulation in the peritoneal cavity
- 80–85% of cases are caused by cirrhosis and portal hypertension
- Core mechanism: portal hypertension → splanchnic vasodilation → RAAS/ADH → sodium retention → ascites
- Ascites marks the transition from compensated to decompensated cirrhosis
- Shifting dullness is the most sensitive clinical sign; fluid thrill indicates massive ascites
- Diagnostic paracentesis is essential for all new-onset ascites
- SAAG ≥1.1 g/dL suggests portal hypertension; SAAG <1.1 suggests malignancy or tuberculosis
- SBP is diagnosed by ascitic fluid neutrophil count ≥250 cells/mm³
- Management targets sodium retention: spironolactone first-line, sodium restriction, LVP for tense ascites
- Ascites should prompt liver transplantation assessment
- Hypoalbuminaemia contributes to ascites, but portal hypertension and sodium retention are the central mechanisms
- Refractory ascites indicates advanced decompensated cirrhosis and should prompt transplant/TIPS consideration
Frequently Asked Questions
References
- Runyon BA; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013;57(4):1651–1653.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460.
- Gines P, Quintero E, Arroyo V, et al. Compensated cirrhosis: natural history and prognostic factors. Hepatology. 1987;7(1):122–128.
- Arroyo V, Ginès P, Gerbes AL, et al. Definition and diagnostic criteria of refractory ascites and hepatorenal syndrome in cirrhosis. Hepatology. 1996;23(1):164–176.
- Cardenas A, Ginès P. Management of patients with cirrhosis awaiting liver transplantation. Gut. 2011;60(4):527–535.
- Moore KP, Aithal GP. Guidelines on the management of ascites in cirrhosis. Gut. 2006;55(Suppl 6):vi1–12.
- Sort P, Naveau M, Arroyo V, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. N Engl J Med. 1999;341(6):403–409.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist hepatological input when investigating and managing patients with ascites.