Many students memorise that a neutrophil count of 250 cells/mm³ or more diagnoses spontaneous bacterial peritonitis. However, SBP is much more than a laboratory cutoff.
SBP represents bacterial infection of ascitic fluid in a patient whose immune defences are already severely impaired by advanced liver disease. It is often the event that precipitates acute kidney injury, hepatorenal syndrome, decompensation and death — even when symptoms are minimal.
This article builds on Ascites Explained and SAAG Explained. Understanding why ascites forms and how to analyse ascitic fluid is essential background before studying SBP in depth.
SBP is not simply infected ascites. It is a major decompensation event in cirrhosis that can trigger acute kidney injury, hepatorenal syndrome and death — often before clear abdominal signs develop. Early paracentesis and treatment are essential.
Learning Objectives
- Define Spontaneous Bacterial Peritonitis
- Explain bacterial translocation and why cirrhotic patients develop SBP
- Diagnose SBP using PMN count
- Differentiate culture-positive SBP, culture-negative neutrocytic ascites, and bacterascites
- Differentiate SBP from secondary bacterial peritonitis
- Explain why intravenous albumin is used in SBP treatment
- Recognise the major complications of SBP
- Understand the rationale for secondary prophylaxis
What Is Spontaneous Bacterial Peritonitis?
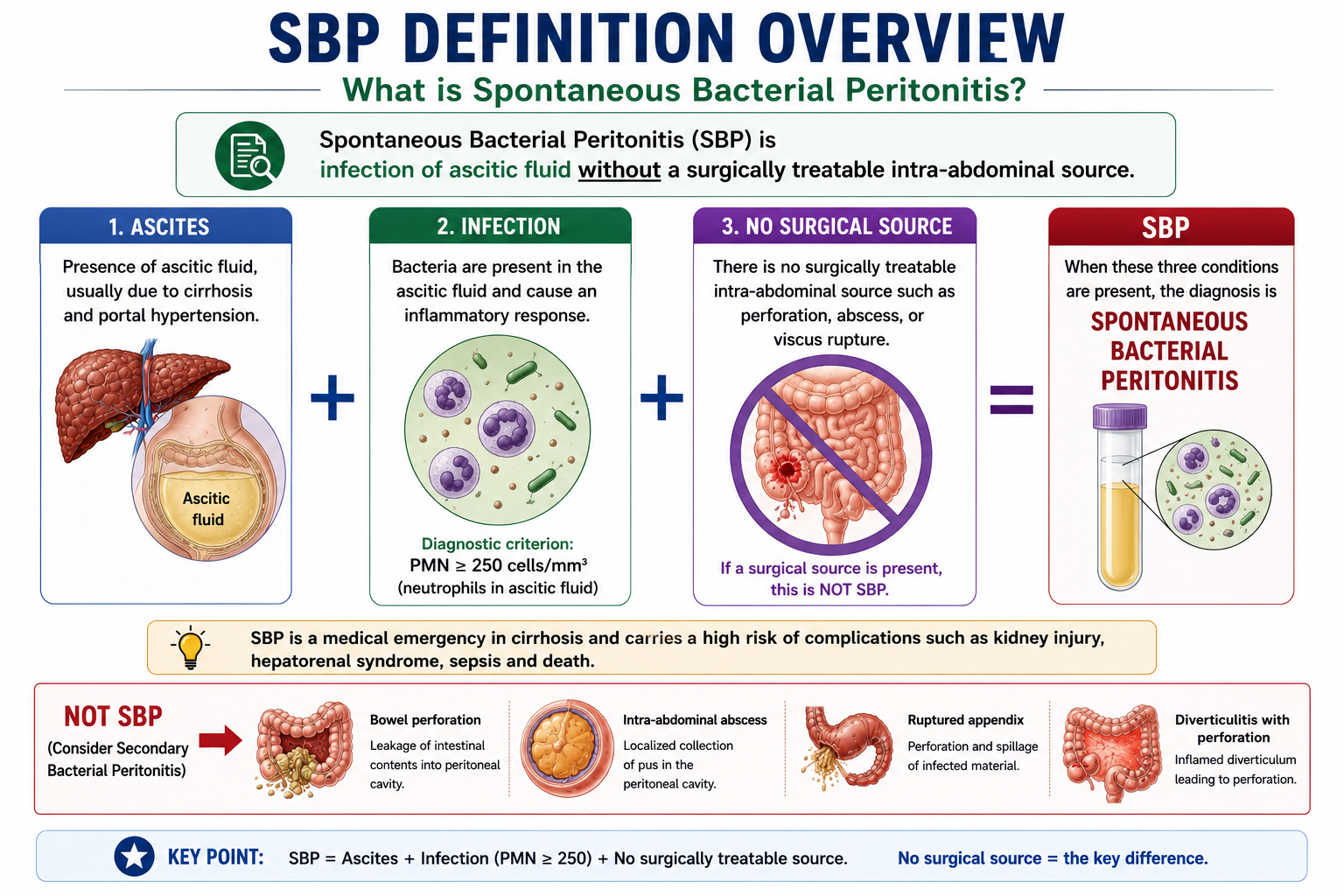
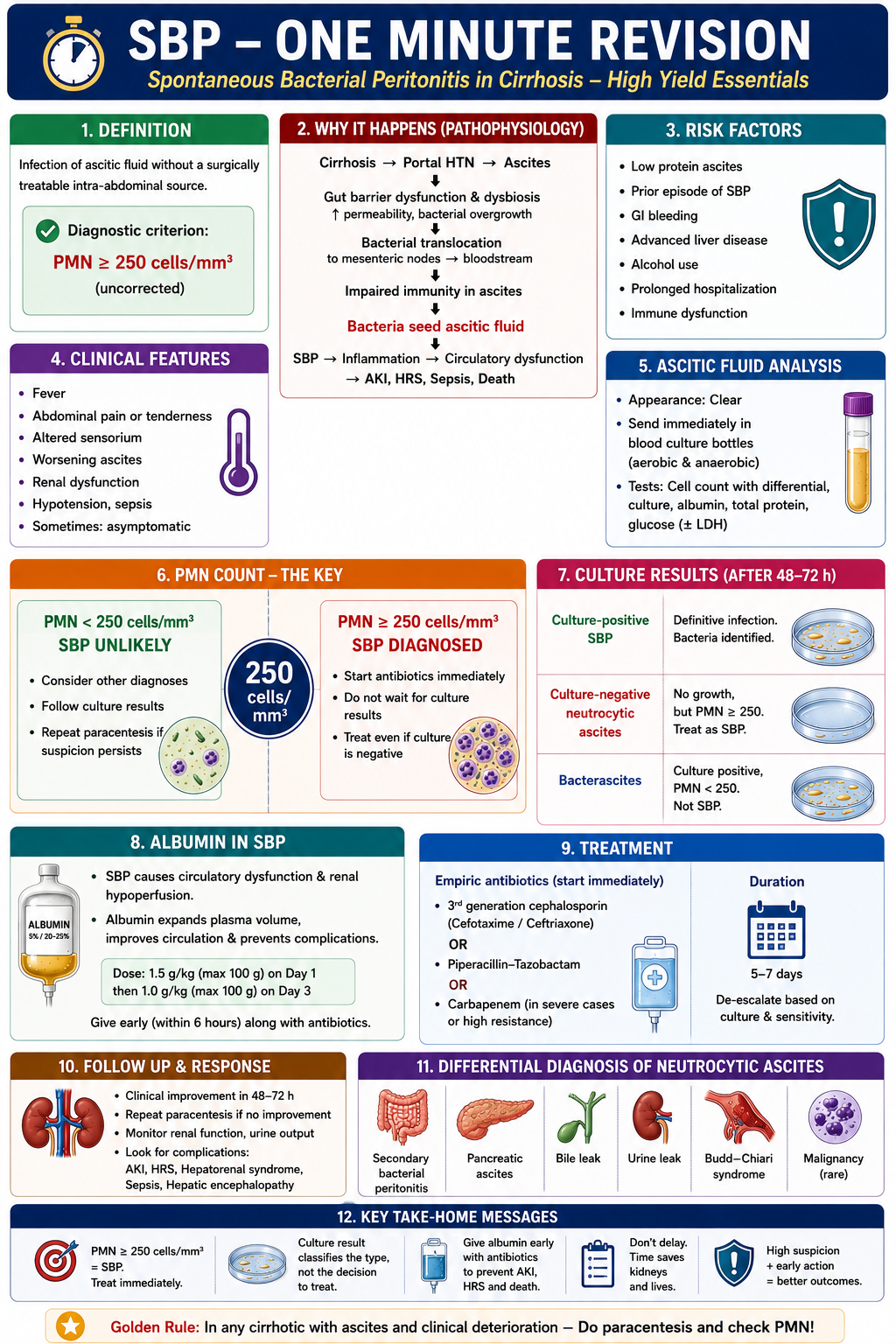
Spontaneous Bacterial Peritonitis is defined as infection of ascitic fluid without a surgically treatable intra-abdominal source.
The word "spontaneous" is critical. There is:
- No bowel perforation
- No ruptured appendix
- No intra-abdominal abscess
- No other identifiable surgical source
When an obvious surgical source is present, the condition is secondary bacterial peritonitis — an entirely different and surgically managed entity.
Why Does SBP Occur?
SBP occurs because cirrhosis causes profound immune dysfunction at multiple levels simultaneously. Portal hypertension alters intestinal function and increases bacterial translocation, while ascitic fluid often has reduced antibacterial activity. Together, these changes allow bacteria to enter and survive within ascitic fluid.
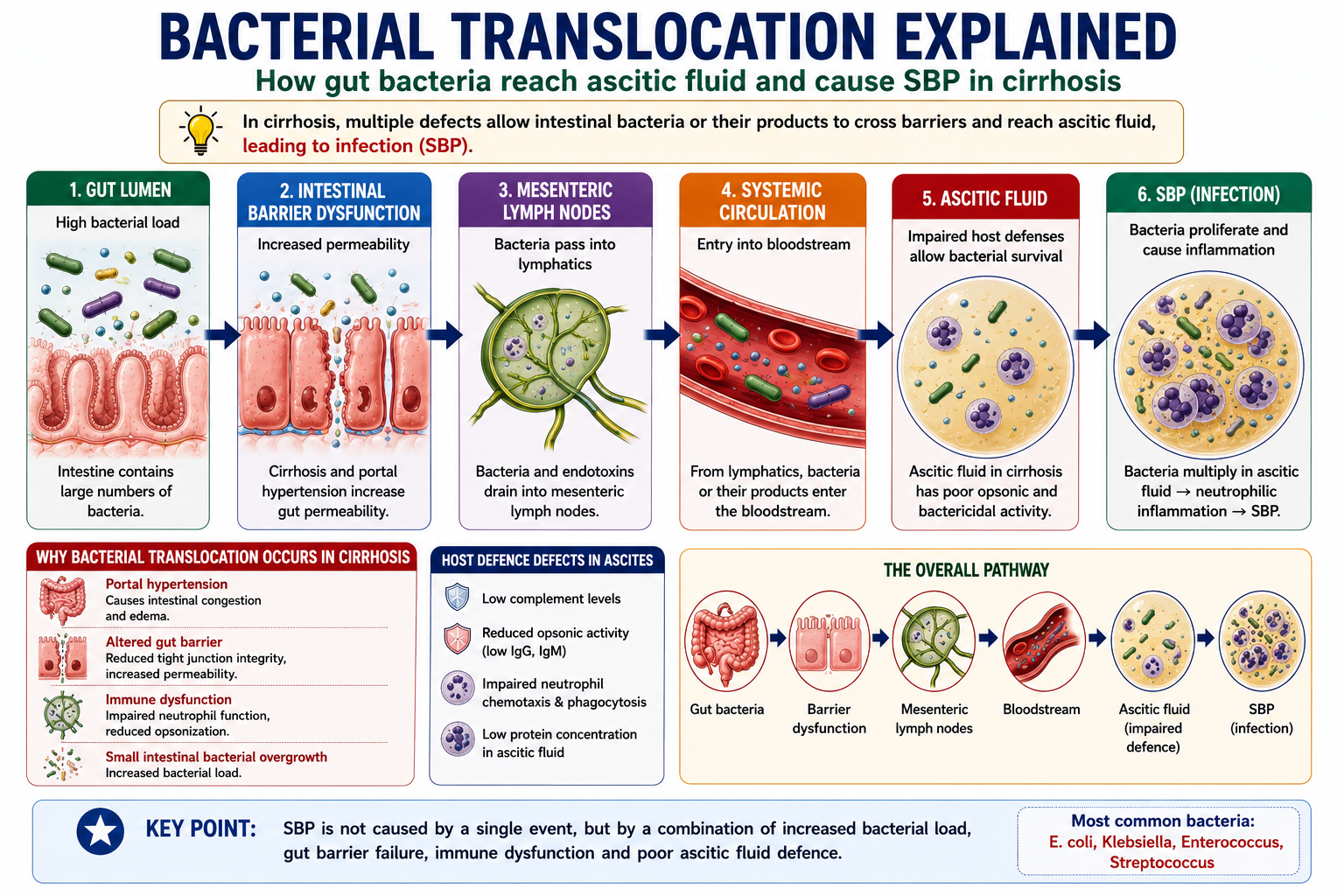
Bacterial Translocation
Bacterial translocation is the passage of viable bacteria — predominantly gut-derived Gram-negative organisms — across the intestinal wall into the mesenteric lymph nodes, portal circulation, and eventually the ascitic fluid.
In a healthy individual, the intact gut mucosal barrier prevents this. In cirrhosis, portal hypertension causes intestinal congestion, dysmotility, and increased permeability. Bacterial overgrowth in the small intestine further increases the microbial load available to translocate.
Pathophysiology of SBP
SBP develops because cirrhosis impairs multiple defence mechanisms simultaneously. Four key defects combine to allow bacterial infection of ascitic fluid to establish and progress:
- 1Altered gut permeability — Portal hypertension and intestinal congestion increase gut mucosal permeability, allowing bacteria and their products to cross the intestinal wall more easily.
- 2Reduced reticuloendothelial function — The reticuloendothelial system (particularly Kupffer cells in the liver) normally clears portal bacteraemia. In cirrhosis, extensive portosystemic shunting allows bacteria to bypass hepatic clearance, increasing systemic bacteraemia.
- 3Impaired neutrophil function — Cirrhosis impairs neutrophil chemotaxis, phagocytosis, and oxidative burst. Even when neutrophils reach the ascitic fluid, their killing ability is reduced.
- 4Reduced opsonic activity in ascitic fluid — Ascitic fluid complement levels and total protein are often low in cirrhosis. Opsonins — proteins that coat bacteria to facilitate phagocytosis — are deficient. This is why patients with low ascitic fluid protein are at highest risk of SBP.

Patients with ascitic fluid total protein <15 g/L are at highest risk of SBP because of low opsonic activity. This is the basis for primary antibiotic prophylaxis in selected high-risk patients with low-protein ascites.
Which Patients Are at Highest Risk of SBP?
SBP does not occur randomly in all patients with ascites. It is most likely when cirrhosis is advanced, ascitic fluid defence is poor, or bacterial translocation is increased.
Recognising high-risk patients is clinically important because some groups benefit from antibiotic prophylaxis.
| Risk Factor | Why It Increases SBP Risk |
|---|---|
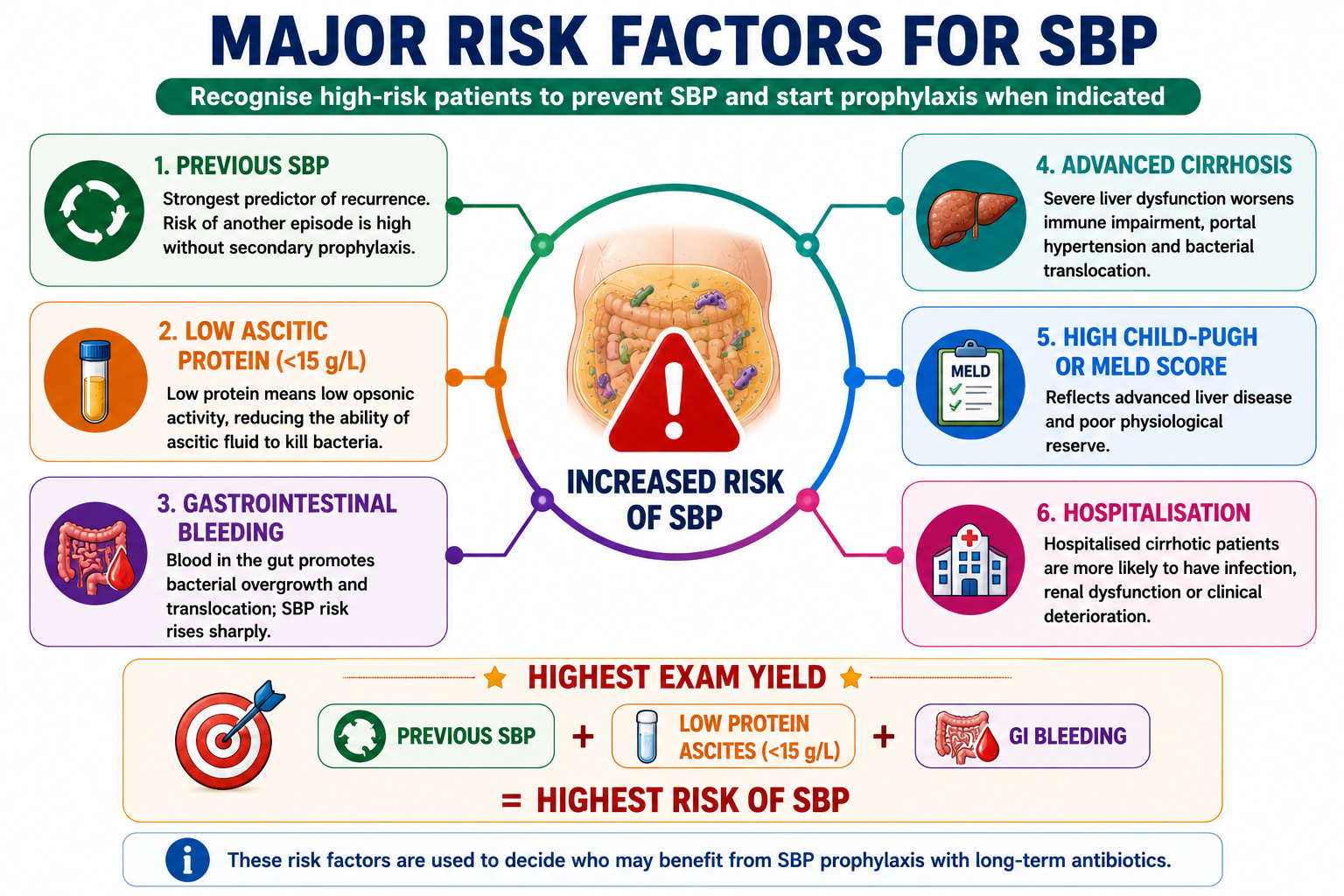
| Previous SBP | Strongest predictor of recurrence; recurrence risk is high without secondary prophylaxis. |
| Low ascitic fluid protein (<15 g/L) | Low protein means low opsonic activity, reducing the ability of ascitic fluid to kill bacteria. |
| Gastrointestinal bleeding | Blood in the gut promotes bacterial overgrowth and translocation; SBP risk rises sharply. |
| Advanced cirrhosis | Severe liver dysfunction worsens immune impairment, portal hypertension and bacterial translocation. |
| High Child-Pugh or MELD score | Reflects advanced liver disease and poor physiological reserve. |
| Hospitalisation | Hospitalised cirrhotic patients are more likely to have infection, renal dysfunction or clinical deterioration. |
The three highest-yield SBP risk factors for exams are: previous SBP, low ascitic fluid protein (<15 g/L), and gastrointestinal bleeding.
Clinical Features
One of the most important clinical teaching points about SBP is that it is often subtle. Classic signs of peritonitis — severe abdominal pain, rigidity, rebound tenderness — may be absent or minimal in cirrhotic patients.
Symptoms and Signs
- Fever — most common feature, though may be low-grade or absent
- Abdominal discomfort — often mild, not peritonitic
- Worsening or new-onset ascites
- Hepatic encephalopathy — confusion or altered behaviour
- Acute kidney injury — rising creatinine
- Hypotension or sepsis in severe cases
Some patients with SBP have no abdominal pain at all. Always suspect SBP in any patient with cirrhosis and ascites who has unexplained deterioration — including new confusion, rising creatinine, fever, or haemodynamic instability — even without abdominal symptoms. The diagnosis can only be confirmed by paracentesis.
Diagnostic Paracentesis
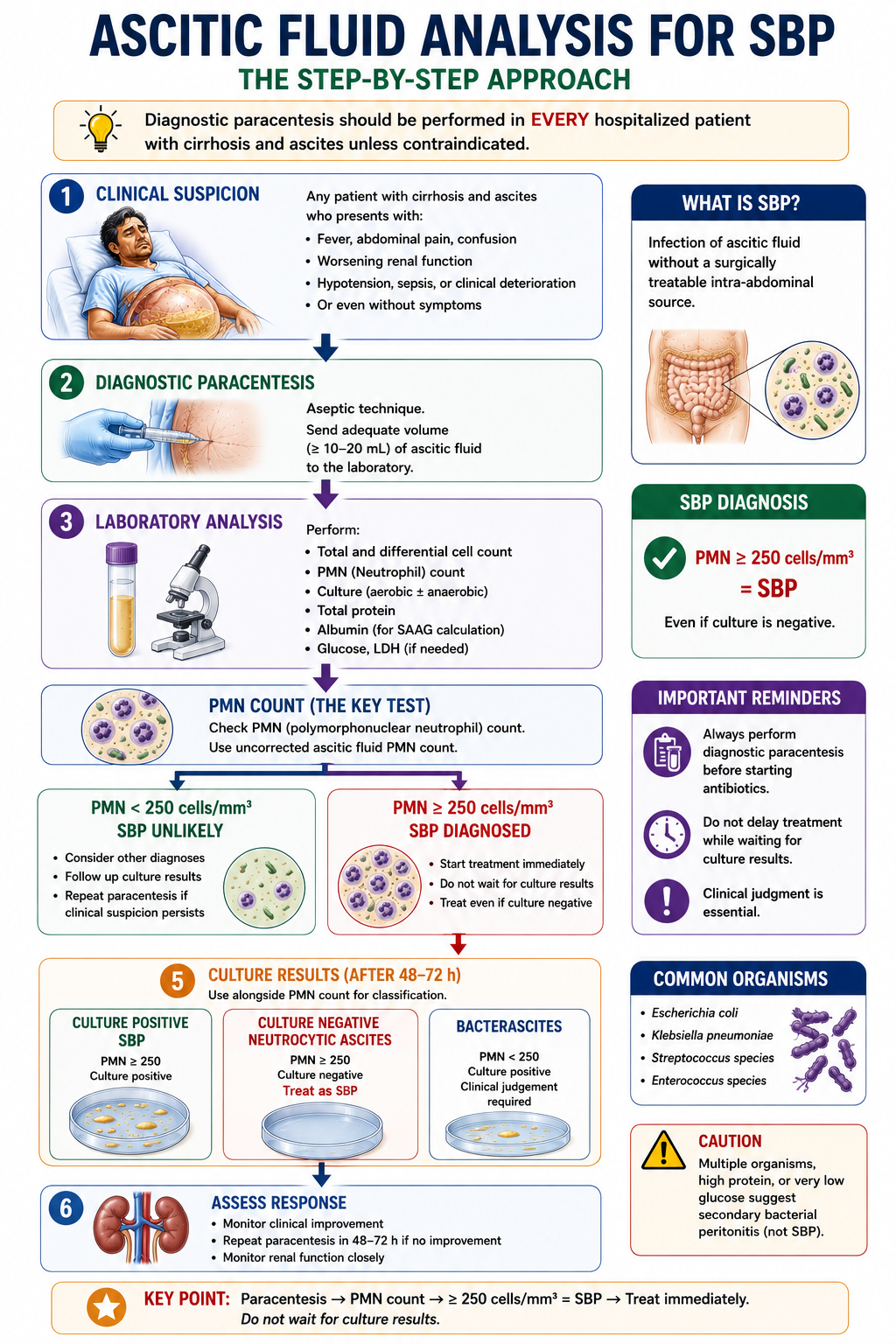
Because clinical features alone are unreliable, every hospitalised patient with ascites should undergo diagnostic paracentesis unless a clear contraindication exists.
Paracentesis should be performed at admission and repeated whenever the patient deteriorates. Delaying paracentesis in favour of empirical treatment without fluid analysis is a clinical error.
PMN Count: The Most Important Diagnostic Criterion
A polymorphonuclear neutrophil (PMN) count of 250 cells/mm³ or more in ascitic fluid diagnoses SBP. This threshold applies regardless of whether culture is positive or negative.
The PMN count is the single most important result in ascitic fluid analysis for SBP. Treatment should not be delayed waiting for culture results — if PMN is ≥250, treat immediately.
| PMN Count | Interpretation | Action |
|---|---|---|
| <250 cells/mm³ | SBP not diagnosed | Monitor; consider other diagnoses |
| ≥250 cells/mm³ | SBP diagnosed | Start antibiotics and albumin immediately |
PMN count makes the diagnosis. Culture result classifies the type. If PMN is ≥250 cells/mm³, treat as SBP even if culture is negative.
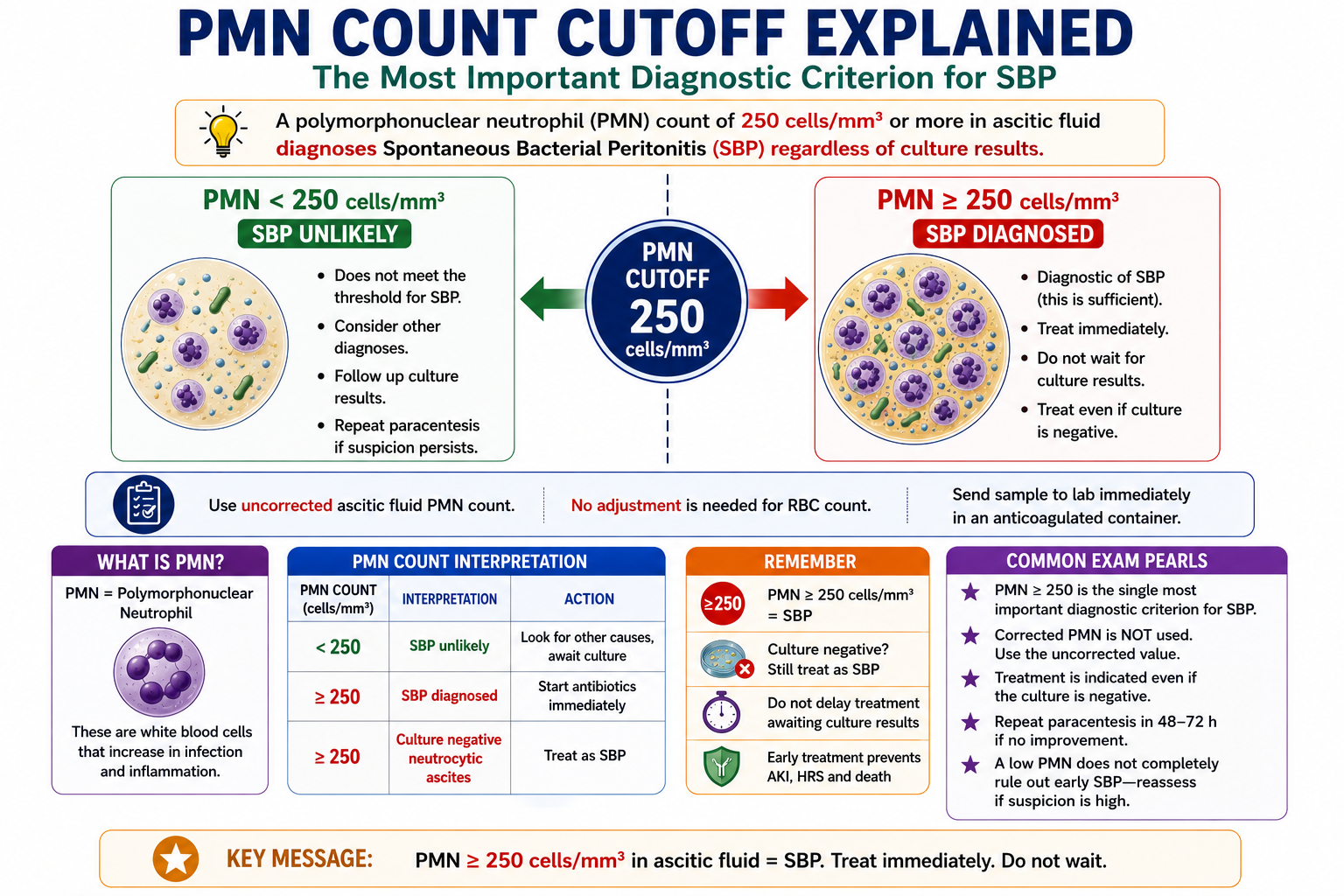
The PMN cutoff is 250 cells/mm³, not 500. Some sources quote total WBC ≥500/mm³ — but PMN ≥250 is the standard diagnostic criterion. Always state "PMN ≥250" in examinations.
Culture Results and SBP Classification
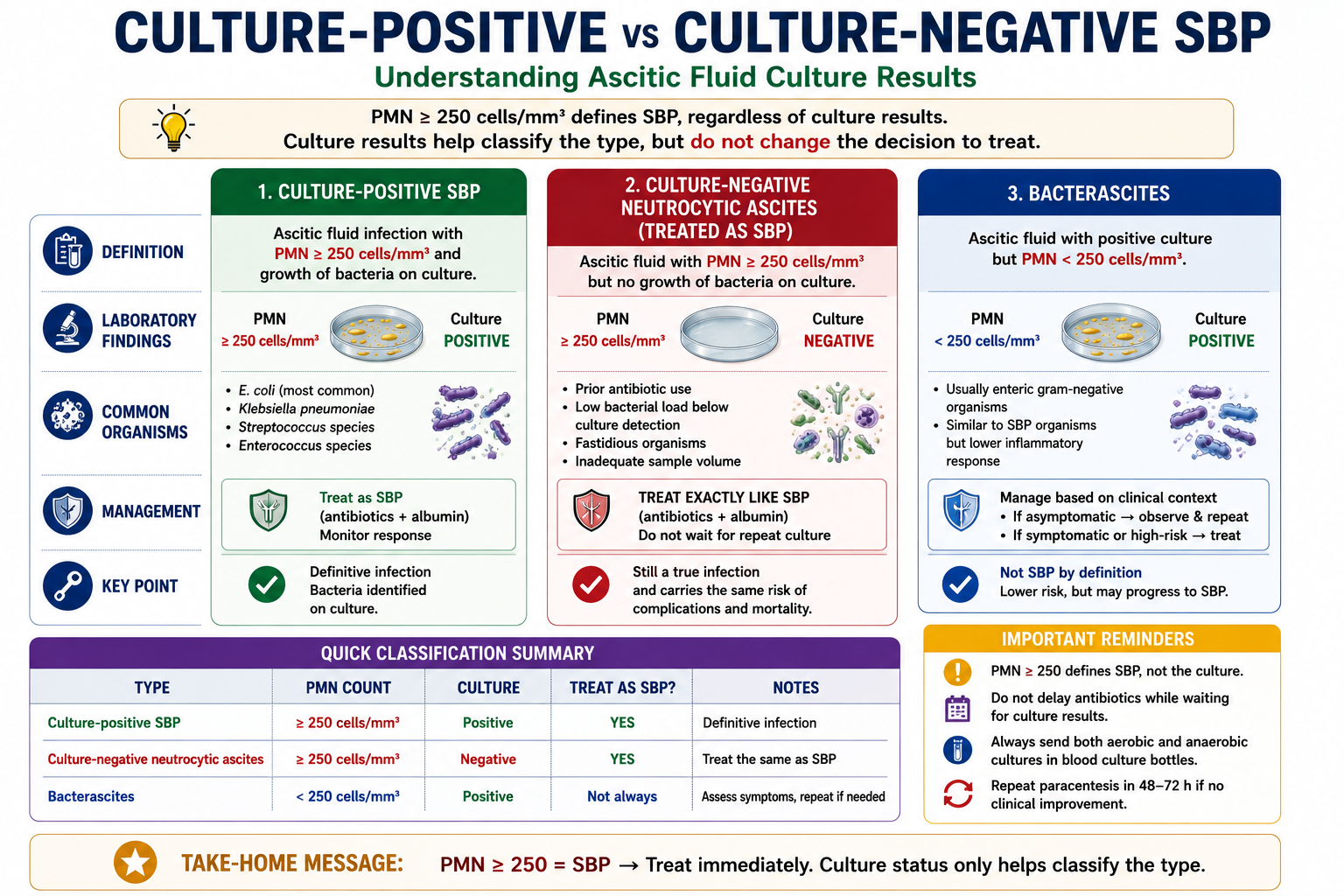
Not all cases of infected ascites are the same. Three distinct conditions are defined by the combination of PMN count and culture result.
| Condition | PMN Count | Culture | Management |
|---|---|---|---|
| SBP | ≥250 cells/mm³ | Positive | Antibiotics + albumin |
| Culture-negative neutrocytic ascites (CNNA) | ≥250 cells/mm³ | Negative | Treat as SBP |
| Bacterascites | <250 cells/mm³ | Positive | Depends on symptoms; repeat paracentesis |
Culture-Negative Neutrocytic Ascites (CNNA)
CNNA occurs when PMN is ≥250 cells/mm³ but culture is negative. This is common — cultures are negative in up to 60% of SBP cases due to low bacterial concentrations in ascitic fluid. CNNA is treated exactly like SBP. The negative culture does not mean the patient does not have infection.
Bacterascites
Bacterascites occurs when culture is positive but PMN remains below 250 cells/mm³. This may represent early colonisation rather than established infection. Management depends on clinical context: if the patient is symptomatic, treatment is usually warranted; if asymptomatic, repeat paracentesis within 48 hours guides the decision.
Common Organisms in SBP
SBP usually arises from enteric organisms that translocate across the gut wall. It is usually monomicrobial. Polymicrobial growth should raise concern for secondary bacterial peritonitis.
| Organism | Clinical Note |
|---|---|
| Escherichia coli | Most common organism; gut-derived Gram-negative bacillus. |
| Klebsiella pneumoniae | Common Gram-negative organism; also enteric in origin. |
| Streptococcus species | Common Gram-positive cause; especially in community-acquired infection. |
| Enterococcus species | Increasingly important, especially in healthcare-associated or nosocomial SBP. |
SBP is usually caused by a single gut-derived organism. Multiple organisms suggest secondary bacterial peritonitis and should prompt imaging and surgical review.
If PMN ≥250 — treat as SBP, regardless of culture. A negative culture does not exclude SBP. Most common organisms are Escherichia coli and Klebsiella pneumoniae — both gut-derived Gram-negative organisms consistent with the bacterial translocation mechanism.
SBP vs Secondary Bacterial Peritonitis
Distinguishing SBP from secondary bacterial peritonitis is an important clinical and examination skill. Secondary peritonitis has a surgical source and requires a fundamentally different management approach.
| Feature | SBP | Secondary Bacterial Peritonitis |
|---|---|---|
| Source | No surgical source | Surgical source present (perforation, abscess) |
| Organisms | Usually single organism | Often polymicrobial (multiple organisms) |
| Ascitic protein | Often low | Often very high (>10 g/L) |
| Ascitic glucose | Normal | Often low (<2.8 mmol/L) |
| Ascitic LDH | Below serum LDH | Above serum LDH |
| Treatment | Medical — antibiotics + albumin | Surgical intervention often required |
Multiple organisms on culture should always raise suspicion for secondary bacterial peritonitis, not SBP. SBP is almost always monomicrobial. Polymicrobial growth suggests bowel perforation or another surgical source — imaging and surgical review are essential.
Why Is Albumin Given in SBP?
Most students memorise "give albumin in SBP" without understanding why. The physiology is straightforward and important.
SBP triggers a profound systemic inflammatory response. This worsens the circulatory dysfunction already present in advanced cirrhosis — splanchnic vasodilation intensifies, effective arterial blood volume falls further, and the kidneys become increasingly underperfused.
Without intervention, this progression leads to acute kidney injury (AKI) and hepatorenal syndrome (HRS) — the most serious complications of SBP, significantly increasing mortality.
How Albumin Helps
Intravenous albumin expands the intravascular volume, improves effective arterial circulation, and reduces renal hypoperfusion. The landmark Sort et al. (1999) trial demonstrated that albumin infusion alongside antibiotics significantly reduced the incidence of AKI and HRS, and improved survival.
| Without Albumin | With Albumin |
|---|---|
| Higher risk of AKI | Reduced AKI incidence |
| Higher risk of HRS | Reduced HRS incidence |
| Higher in-hospital mortality | Improved survival |
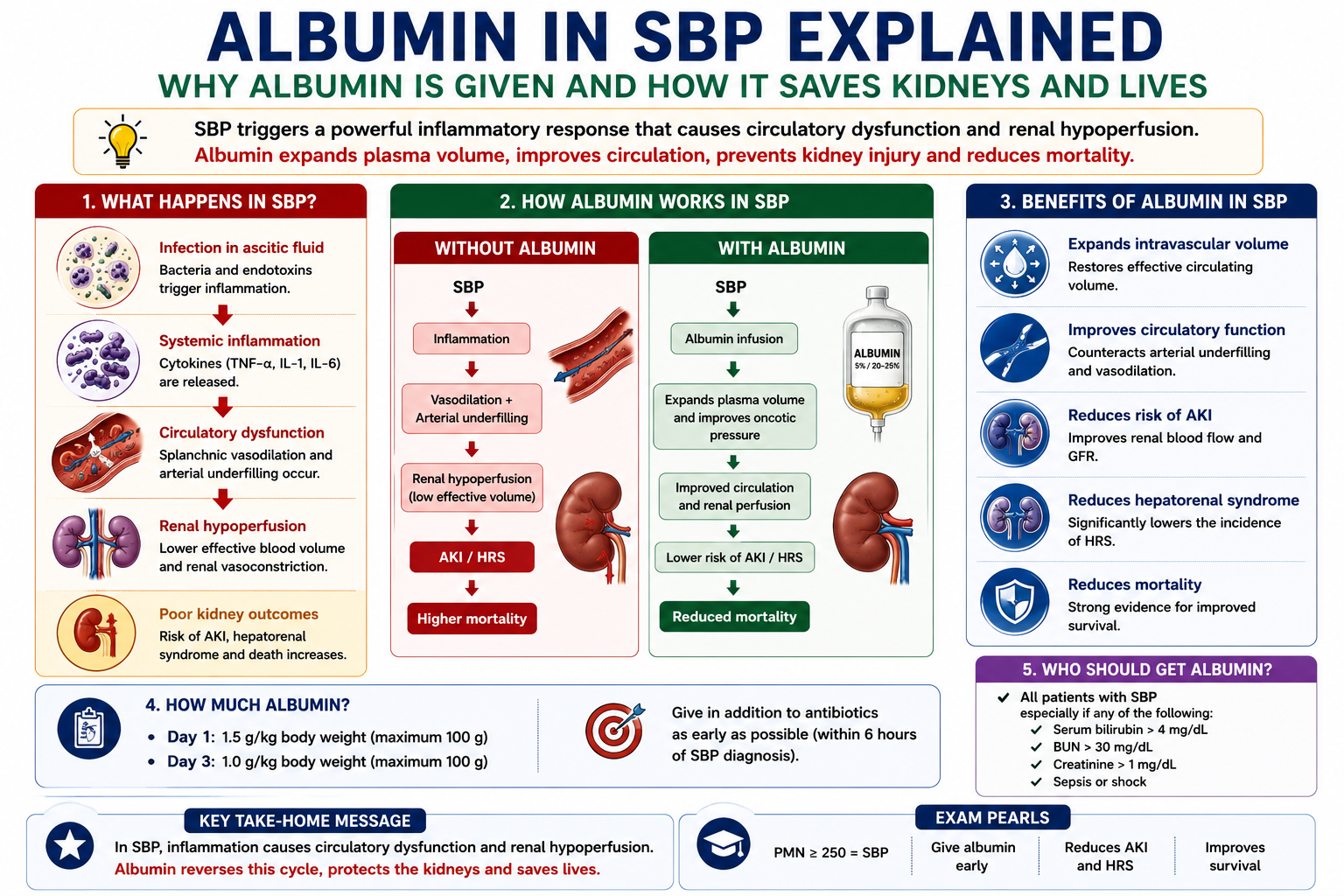
Crystalloid fluids (e.g. normal saline) can worsen ascites and hyponatraemia without effectively expanding the intravascular oncotic volume. Albumin, as a colloid, remains within the intravascular compartment for longer, providing sustained haemodynamic benefit. This is why albumin — not saline — is the specific intervention shown to reduce HRS in SBP.
Management Overview
Detailed antibiotic protocols are beyond the scope of this article. The key principles of SBP management reflect the underlying pathophysiology:
- Immediate antibiotics — Start as soon as PMN ≥250 is confirmed. Do not wait for culture results. Third-generation cephalosporins (e.g. cefotaxime) are the standard first-line choice in most guidelines.
- Intravenous albumin — At diagnosis and on day 3. Reduces AKI and HRS risk. Evidence-based intervention (Sort et al. 1999).
- Monitor renal function — Creatinine, urea, and electrolytes daily. Early recognition of AKI is essential.
- Repeat paracentesis at 48 hours — To confirm treatment response (PMN should fall by >25%).
- Identify and manage precipitating cause — GI bleed, recent procedure, new medication.
The renal consequences of SBP — including hepatorenal syndrome — will be covered in detail in the forthcoming Hepatorenal Syndrome Explained article.
Complications of SBP
SBP is associated with serious complications that collectively account for its high mortality.
- Acute kidney injury (AKI) — develops in up to 30% of SBP episodes without albumin therapy
- Hepatorenal syndrome (HRS) — functional renal failure triggered by the circulatory dysfunction of SBP
- Hepatic encephalopathy — precipitated by systemic infection and metabolic derangement
- Septic shock — when systemic inflammatory response and circulatory dysfunction progress
- Death — in-hospital mortality of SBP remains significant, particularly when complicated by HRS
Among all complications of SBP, hepatorenal syndrome is particularly important. SBP is one of the most common precipitants of HRS in cirrhosis. The mechanism — worsening circulatory dysfunction and renal vasoconstriction — is a direct continuation of the same haemodynamic cascade described in Ascites Explained. This is why albumin — which interrupts this cascade — significantly reduces HRS incidence when given with antibiotics.
Prevention
Patients who survive an episode of SBP have a high risk of recurrence — historically up to 70% within one year without prophylaxis. Secondary antibiotic prophylaxis significantly reduces recurrence risk.
Primary prophylaxis is also given to selected high-risk patients who have not yet had SBP — particularly those with low ascitic fluid protein (<15 g/L) or patients hospitalised with a gastrointestinal bleed, in whom the risk of SBP is markedly elevated.
Know the two clinical scenarios that warrant primary SBP prophylaxis: (1) ascitic fluid protein <15 g/L with advanced liver disease (low Child-Pugh / high MELD), and (2) acute gastrointestinal bleeding in a cirrhotic patient. Secondary prophylaxis is given to all patients who survive a first SBP episode.
One-Minute SBP Revision
High-Yield Exam Pearls
PMN ≥250 cells/mm³ = SBP
Culture-negative neutrocytic ascites = treat as SBP
Every hospitalised patient with ascites → diagnostic paracentesis
Albumin reduces AKI and HRS
Most common organisms: E. coli, Klebsiella
SBP may occur without abdominal pain
Multiple organisms → suspect secondary bacterial peritonitis
Ascitic protein <15 g/L → highest SBP risk
- PMN cutoff is 250 — not 500, not 200. State this clearly in exams.
- Treat CNNA as SBP — negative culture does not exclude infection.
- Albumin mechanism — improves effective arterial volume, reduces renal hypoperfusion and HRS. Albumin is not just a protein supplement.
- PMN is diagnosis; culture is classification — culture-negative neutrocytic ascites is still treated as SBP.
- Polymicrobial culture suggests secondary bacterial peritonitis and should trigger imaging/surgical review.
- Previous SBP is the strongest indication for secondary prophylaxis.
- Multiple organisms on culture — always think secondary peritonitis, not SBP.
- SBP without abdominal pain — classic exam scenario; any deterioration in cirrhosis = paracentesis.
- Low ascitic protein (<15 g/L) = highest SBP risk due to reduced opsonic activity.
- Prophylaxis indications — post-SBP (secondary), GI bleed, low ascitic protein (primary).
Key Takeaways
- SBP is infection of ascitic fluid without a surgically treatable intra-abdominal source
- SBP is a major decompensation event — not simply infected ascites
- Bacterial translocation from the gut is the primary mechanism
- Cirrhosis impairs gut barrier function, reticuloendothelial clearance, neutrophil function, and ascitic opsonic activity
- PMN ≥250 cells/mm³ diagnoses SBP regardless of culture result
- Highest-risk patients include those with previous SBP, low ascitic fluid protein, GI bleeding and advanced cirrhosis
- PMN count makes the diagnosis; culture result classifies the infection pattern
- SBP is usually monomicrobial; polymicrobial culture suggests secondary bacterial peritonitis
- Culture-negative neutrocytic ascites is treated the same as SBP
- Multiple organisms on culture suggest secondary bacterial peritonitis, not SBP
- Albumin reduces AKI and HRS by improving effective arterial circulation
- Most common organisms: E. coli and Klebsiella pneumoniae
- SBP may occur without abdominal pain — always paracentese on clinical deterioration
- Secondary prophylaxis is given after every SBP episode to prevent recurrence
Frequently Asked Questions
References
- Sort P, Naveau M, Arroyo V, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. N Engl J Med. 1999;341(6):403–409.
- Runyon BA; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013;57(4):1651–1653.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460.
- Wiest R, Garcia-Tsao G. Bacterial translocation in cirrhosis. Hepatology. 2005;41(3):422–433.
- Fernández J, Naveau S, Colmenero J, et al. Bacterial infections in cirrhosis: epidemiological changes with healthcare-associated and nosocomial infections. J Hepatol. 2012;56(suppl 1):S1–12.
- Moreau R, Naveau S, Thévenot T, et al. Diagnosis, management, and prognosis of spontaneous bacterial peritonitis. Liver Int. 2018;38(Suppl 1):6–15.
- Bernardi M, Caraceni P, Navickis RJ, Wilkes MM. Albumin infusion in patients undergoing large-volume paracentesis: a meta-analysis of randomized trials. Hepatology. 2012;55(4):1172–1181.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist hepatological input when managing patients with suspected SBP.