Most students memorise that SAAG ≥1.1 g/dL means portal hypertension and SAAG <1.1 g/dL means non-portal hypertension. But SAAG becomes much easier when you understand what it is actually measuring.
SAAG does not simply describe ascitic fluid in isolation. It compares serum albumin with ascitic fluid albumin. This gradient indirectly reflects the hydrostatic pressure forcing fluid out of the portal circulation into the peritoneal cavity.
This article is the diagnostic bridge in the hepatology cluster. Read Ascites Explained first to understand why fluid accumulates, then use this article to understand how to classify and investigate it.
SAAG is a pressure clue. A high SAAG usually means that elevated portal pressure is driving fluid into the peritoneal cavity. A low SAAG usually means that something else — peritoneal disease, malignancy, or protein-rich leakage — is responsible.
Learning Objectives
- Define SAAG and state the formula correctly
- Calculate SAAG from given albumin values
- Explain the physiology behind high SAAG
- Explain the physiology behind low SAAG
- List the common causes of high SAAG and low SAAG ascites
- Interpret SAAG in combination with ascitic fluid protein
- Apply a systematic approach to ascitic fluid analysis
What Is SAAG?
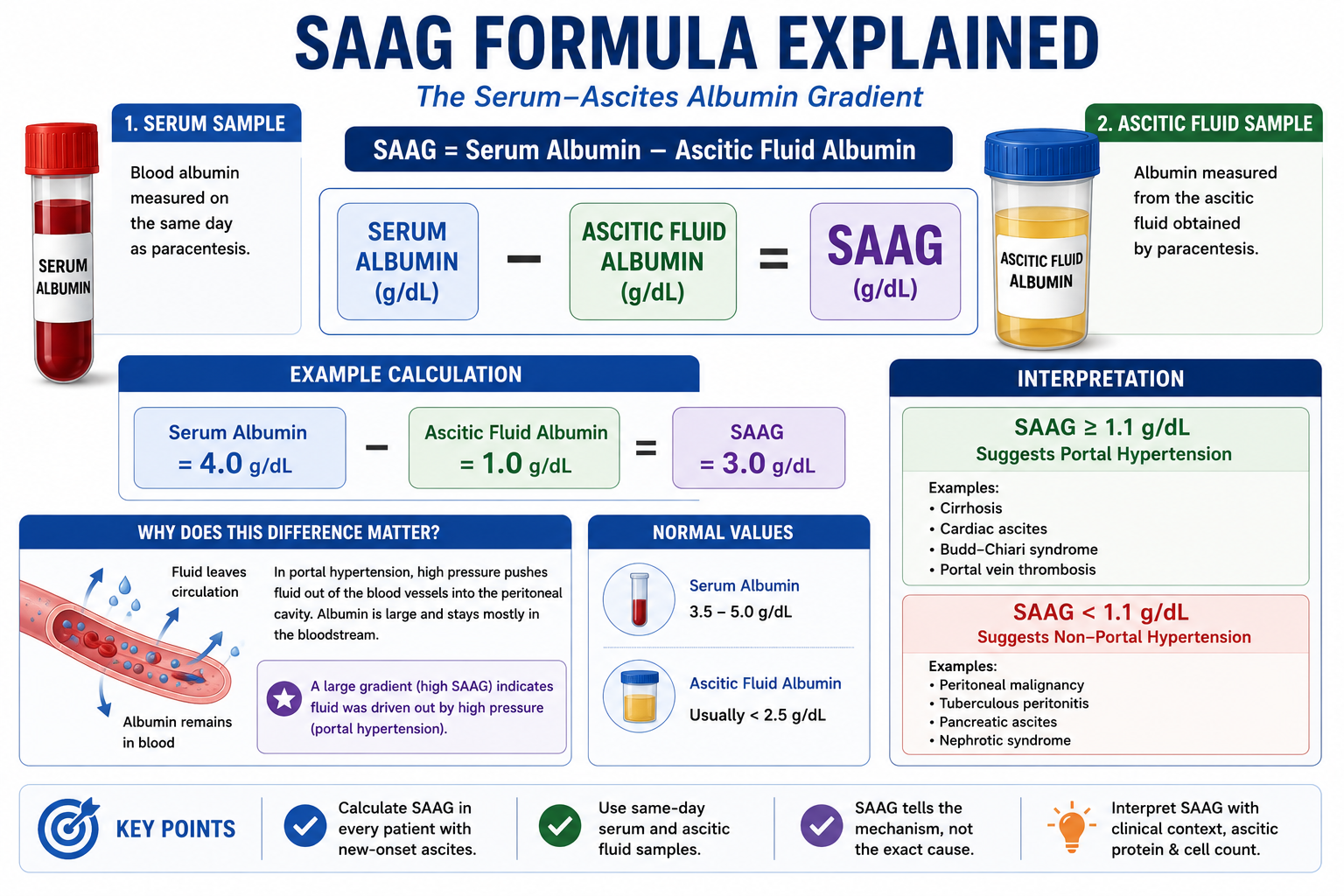
SAAG stands for Serum-Ascites Albumin Gradient. It is calculated by subtracting ascitic fluid albumin from serum albumin, using samples taken on the same day.
SAAG = Serum Albumin − Ascitic Fluid Albumin
Both the serum sample and the ascitic fluid sample must be taken on the same day to ensure accuracy. The result is expressed in g/dL.
Interpretation
| SAAG | Interpretation |
|---|---|
| ≥ 1.1 g/dL | Portal hypertension likely |
| < 1.1 g/dL | Portal hypertension unlikely — consider non-portal hypertensive cause |
Quick Calculation Example
Serum albumin = 4.0 g/dL
Ascitic fluid albumin = 1.0 g/dL
SAAG = 4.0 − 1.0 = 3.0 g/dL → High SAAG → Portal hypertension likely
Why Was SAAG Developed?
Older teaching classified ascitic fluid as a transudate (protein <25 g/L) or an exudate (protein ≥25 g/L). While simple, this approach was unreliable — many conditions produced results that overlapped, and low serum albumin (common in cirrhosis) artificially lowered ascitic fluid protein, misclassifying portal hypertensive ascites as an exudate.
SAAG became the preferred tool because it reflects the presence or absence of portal hypertension more directly. By comparing serum and ascitic albumin as a gradient — rather than relying on ascitic fluid protein alone — SAAG corrects for variation in serum albumin levels.
Because SAAG uses a gradient rather than an absolute ascitic fluid protein value, it remains useful even when serum albumin is low. This is especially important in cirrhosis, where hypoalbuminaemia is common.
SAAG is superior to simple transudate/exudate classification for identifying portal hypertensive ascites. This is a well-established exam point. The transudate/exudate classification is still taught but SAAG is the preferred clinical tool.
What Does SAAG Actually Measure?
SAAG measures the difference between albumin concentration in the blood and albumin concentration in ascitic fluid. Understanding why this difference changes with portal pressure is the key to understanding SAAG intuitively.
SAAG tells you the mechanism of ascites — whether portal hypertension is likely or unlikely. It does not give the final diagnosis by itself. The final cause must be determined using clinical context, ascitic fluid protein, cell count, culture, imaging, and additional tests when needed.
In Portal Hypertension — High SAAG
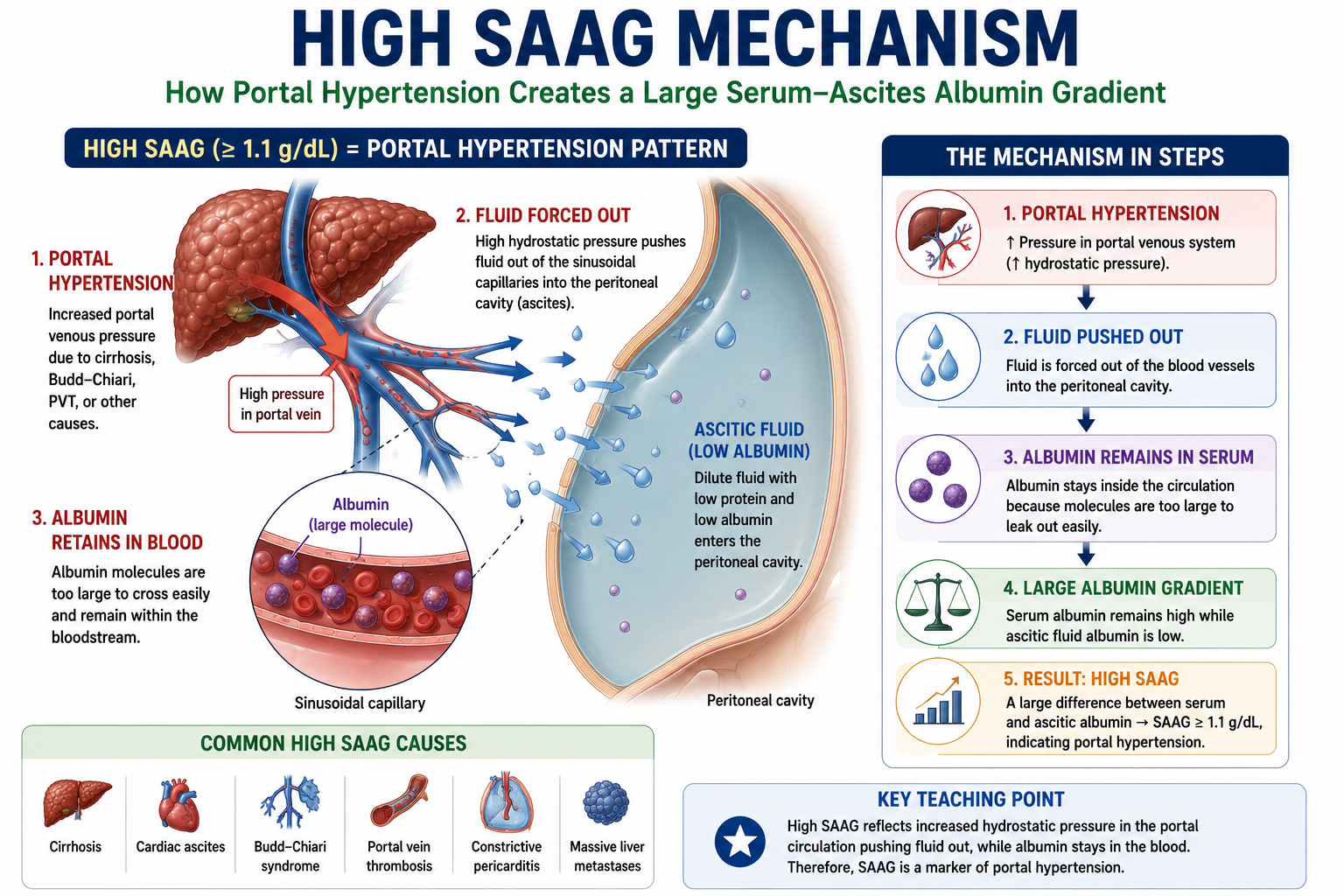
In portal hypertension, raised hydrostatic pressure in the portal and mesenteric capillaries forces fluid out of the vascular space into the peritoneal cavity. This fluid is largely water with electrolytes — albumin, being a large protein, tends to remain relatively concentrated within the bloodstream.
Therefore, serum albumin stays much higher than ascitic fluid albumin, creating a large gradient — a high SAAG.
In Peritoneal Disease — Low SAAG
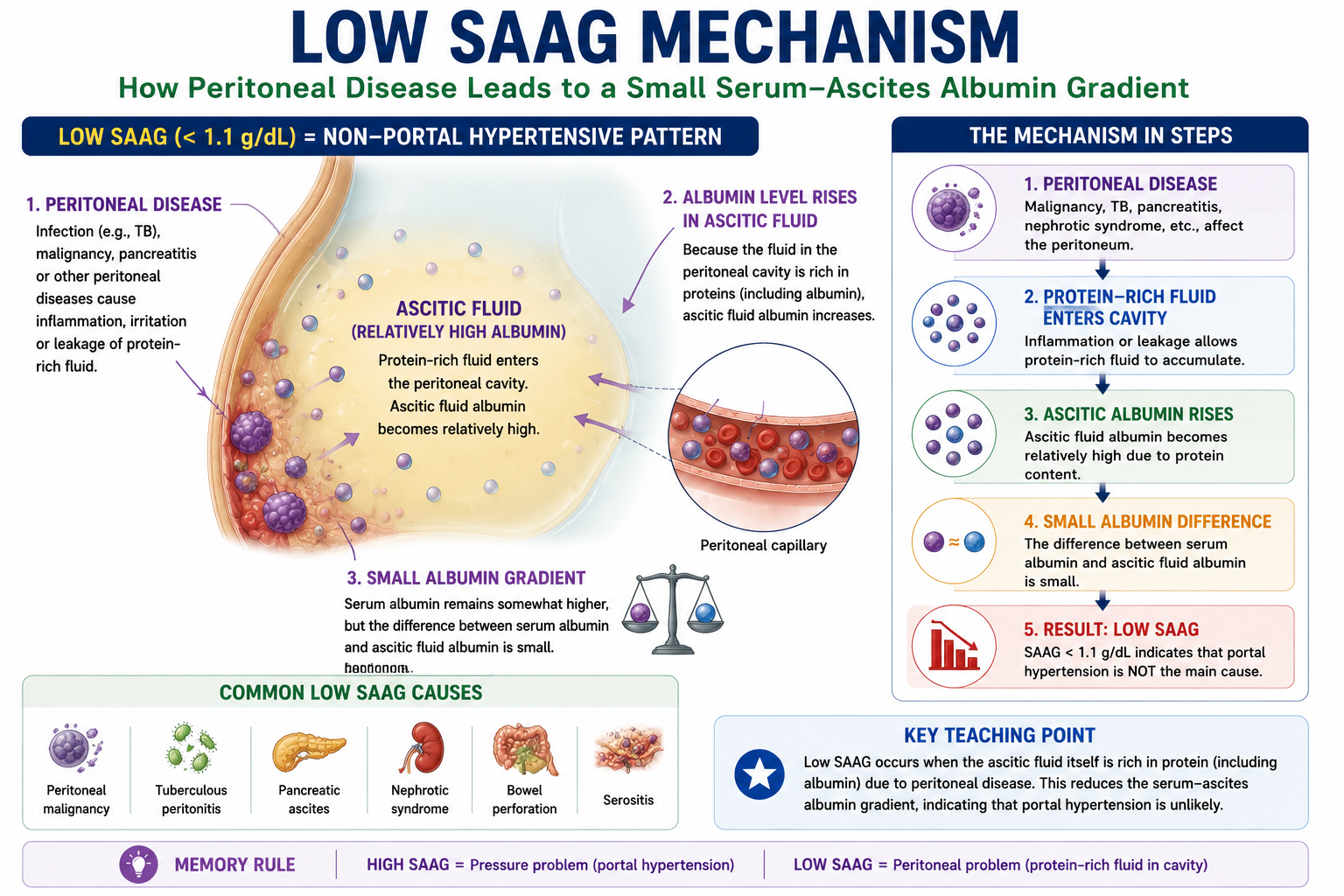
When ascites arises from peritoneal inflammation, malignancy, or lymphatic obstruction, the mechanism is different. Diseased peritoneum or disrupted lymphatics allow protein-rich fluid to accumulate in the ascitic space. Ascitic fluid albumin rises. Because ascitic fluid albumin is now relatively high, the difference between serum albumin and ascitic albumin becomes small — a low SAAG.
High SAAG: Portal Hypertension Pattern
A SAAG of 1.1 g/dL or more suggests that ascites is caused by portal hypertension. This does not mean cirrhosis only — it means that portal or hepatic venous pressure is elevated from any cause.
Causes of High SAAG Ascites
- Cirrhosis — most common cause overall
- Alcohol-related liver disease with portal hypertension
- Cardiac ascites — right heart failure, tricuspid regurgitation
- Constrictive pericarditis — elevated venous backpressure to portal system
- Budd–Chiari syndrome — hepatic vein thrombosis causing post-hepatic portal hypertension
- Portal vein thrombosis — pre-hepatic portal hypertension
- Massive liver metastases — extensive hepatic replacement causing portal hypertension
High SAAG means portal hypertension — not necessarily cirrhosis. Cardiac ascites, Budd–Chiari syndrome and portal vein thrombosis all produce high SAAG despite the liver itself being structurally normal in some cases. Always correlate with clinical findings.
Low SAAG: Non-Portal Hypertensive Pattern
A SAAG below 1.1 g/dL suggests that portal hypertension is not the main mechanism. The problem is usually peritoneal inflammation, malignancy, infection, or leakage of protein-rich fluid into the peritoneal cavity — causing ascitic albumin to be relatively high.
Causes of Low SAAG Ascites
- Peritoneal malignancy — carcinomatosis from ovarian, gastric, colon, pancreatic cancers
- Tuberculous peritonitis — important in endemic regions; high protein, raised ADA
- Pancreatic ascites — duct disruption; very high ascitic amylase is characteristic
- Nephrotic syndrome — hypoalbuminaemia-driven; low SAAG but protein may also be low
- Bowel perforation / serositis — chemical peritonitis producing protein-rich fluid
Low SAAG does not mean malignancy only. Always consider tuberculous peritonitis — especially in patients from endemic regions — and pancreatic ascites. Check ADA (adenosine deaminase) for TB and amylase for pancreatic ascites when SAAG is low.
High SAAG vs Low SAAG: Summary Table
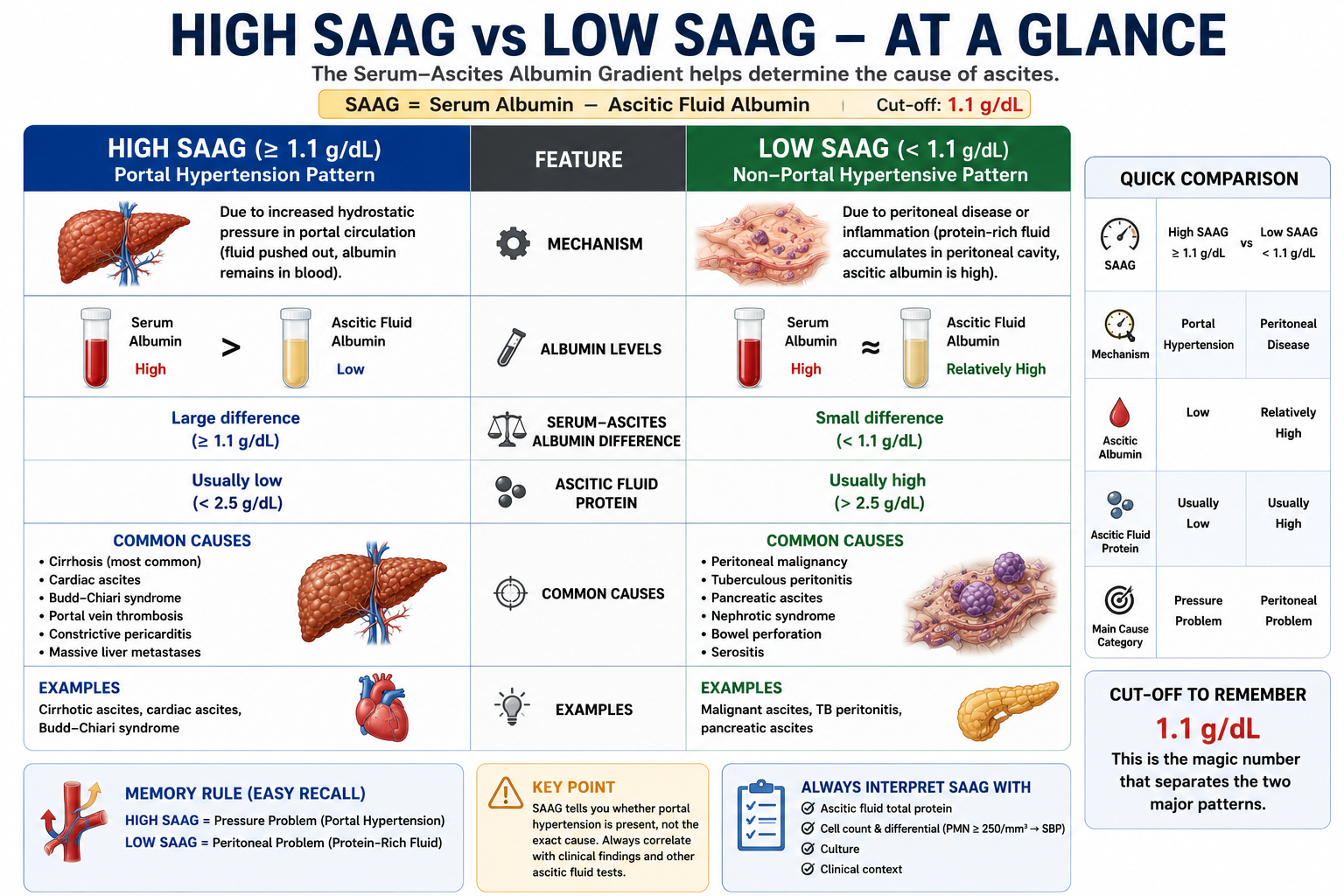
| Feature | High SAAG ≥1.1 g/dL | Low SAAG <1.1 g/dL |
|---|---|---|
| Mechanism | Portal hypertension — hydrostatic pressure drives albumin-poor fluid out | Peritoneal disease — protein-rich fluid accumulates |
| Ascitic albumin | Low | Relatively high |
| Common causes | Cirrhosis, cardiac ascites, Budd–Chiari, portal vein thrombosis | Malignancy, TB, pancreatic ascites, nephrotic syndrome |
| Memory rule | Pressure problem | Peritoneal / protein problem |
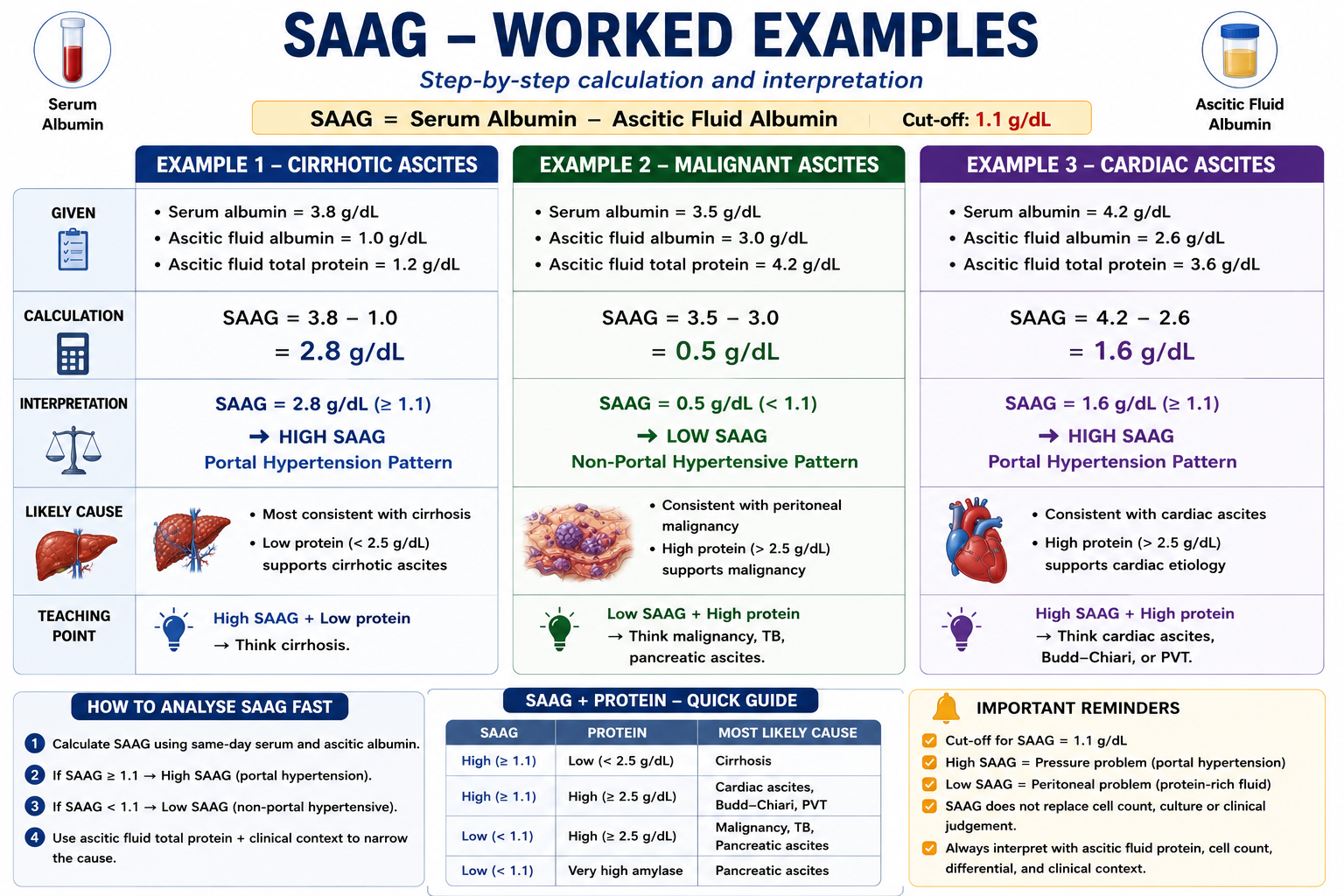
Worked Examples
Practice interpreting SAAG with these three representative clinical scenarios.
Serum albumin = 3.8 g/dL
Ascitic fluid albumin = 1.0 g/dL
SAAG = 3.8 − 1.0 = 2.8 g/dL
High SAAG. Portal hypertension likely. Clinical findings of cirrhosis confirm the diagnosis.
Serum albumin = 3.5 g/dL
Ascitic fluid albumin = 3.0 g/dL
SAAG = 3.5 − 3.0 = 0.5 g/dL
Low SAAG. Portal hypertension unlikely. Consider malignancy, tuberculosis or pancreatic ascites. Send cytology, ADA and amylase.
Serum albumin = 4.2 g/dL
Ascitic fluid albumin = 2.6 g/dL
SAAG = 4.2 − 2.6 = 1.6 g/dL
High SAAG. Portal hypertension pattern. However, ascitic fluid protein is also high — this combination suggests cardiac ascites or Budd–Chiari rather than cirrhosis.
- Cirrhotic ascites: High SAAG + low ascitic fluid protein
- Cardiac ascites: High SAAG + high ascitic fluid protein
Both are high-SAAG. The protein level distinguishes them.
SAAG Combined with Ascitic Fluid Protein
SAAG tells you whether portal hypertension is present. Ascitic fluid protein helps narrow which cause within each group. Using them together gives a much more precise interpretation.
| SAAG | Ascitic Fluid Protein | Likely Diagnosis |
|---|---|---|
| High (≥1.1) | Low (<25 g/L) | Cirrhosis |
| High (≥1.1) | High (≥25 g/L) | Cardiac ascites / Budd–Chiari syndrome |
| Low (<1.1) | High (≥25 g/L) | Malignancy / Tuberculous peritonitis |
| Low (<1.1) | Very high amylase | Pancreatic ascites |
- High SAAG + high protein → think cardiac ascites or Budd–Chiari
- High SAAG + low protein → think cirrhosis
- Low SAAG + high protein → think malignancy or TB
- Low SAAG + very high amylase → think pancreatic ascites
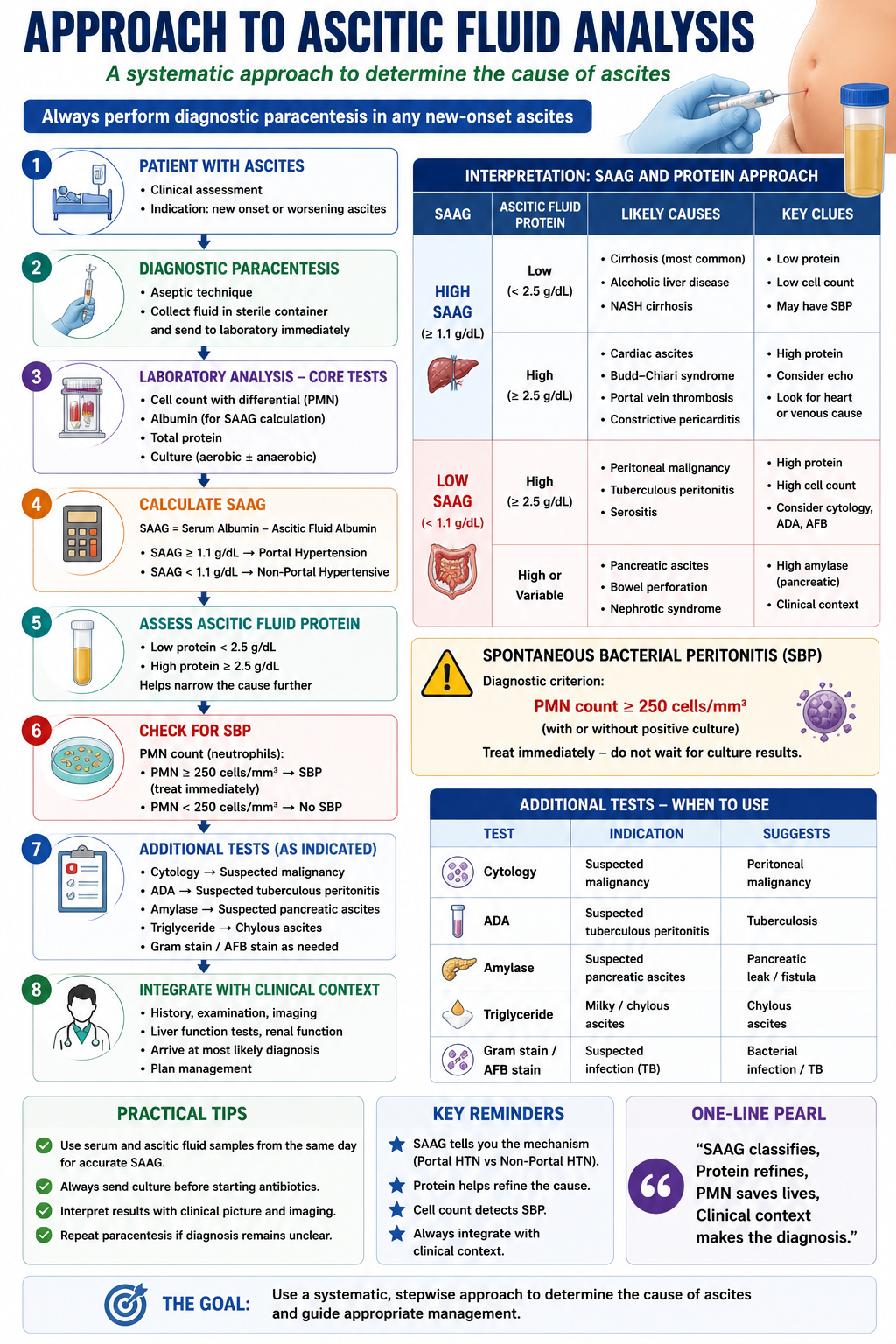
Approach to Ascitic Fluid Analysis
SAAG should never be interpreted in isolation. A complete ascitic fluid analysis follows a structured algorithm, with SAAG as one essential component.
Ascitic fluid neutrophil count ≥250 cells/mm³ diagnoses spontaneous bacterial peritonitis (SBP), regardless of SAAG. SBP can occur in any patient with ascites and may present with minimal symptoms. Never skip cell count — it is the most urgent result to act on.
Common Pitfalls
High SAAG means portal hypertension. Cirrhosis is the most common cause, but cardiac ascites, Budd–Chiari syndrome, portal vein thrombosis and constrictive pericarditis can all produce a high SAAG. Always correlate with clinical findings and ascitic protein.
Tuberculous peritonitis and pancreatic ascites are equally important low-SAAG causes. In patients from TB-endemic regions, always send ADA (adenosine deaminase). Send amylase when pancreatic ascites is suspected.
SAAG is only valid if serum albumin and ascitic fluid albumin are measured from samples collected on the same day. Using values from different time points introduces error and may lead to misclassification.
SAAG identifies the mechanism — portal hypertension or not. It does not replace cell count, culture, cytology, or the full clinical picture. An isolated SAAG result without clinical context and full fluid analysis is incomplete and potentially misleading.
Exam Pearls
SAAG formula = Serum albumin − Ascitic albumin
Cutoff = 1.1 g/dL
High SAAG (≥1.1) = portal hypertension
Low SAAG (<1.1) = non-portal hypertensive ascites
Most common high-SAAG cause = cirrhosis
High SAAG + high protein = cardiac ascites / Budd–Chiari
High SAAG + low protein = cirrhosis
Low SAAG + high protein = malignancy or TB
Low SAAG + very high amylase = pancreatic ascites
Ascitic neutrophils ≥250/mm³ = SBP
- SAAG ≥1.1 = portal hypertension — not cirrhosis specifically.
- Malignancy is usually low SAAG, but massive liver metastases or portal venous obstruction can produce high SAAG by causing portal hypertension.
- SAAG <1.1 = non-portal — malignancy, TB, pancreatic are the three most important.
- Cardiac ascites is high SAAG with high protein — this distinguishes it from cirrhosis.
- Both samples same day — always specify this when asked about SAAG method.
- SAAG replaced transudate/exudate — explain why: more accurate for portal hypertension.
- Cell count first — SBP (neutrophils ≥250/mm³) takes clinical priority over SAAG in acute deterioration.
One-Minute SAAG Revision
Use this summary as a rapid pre-examination revision aid.
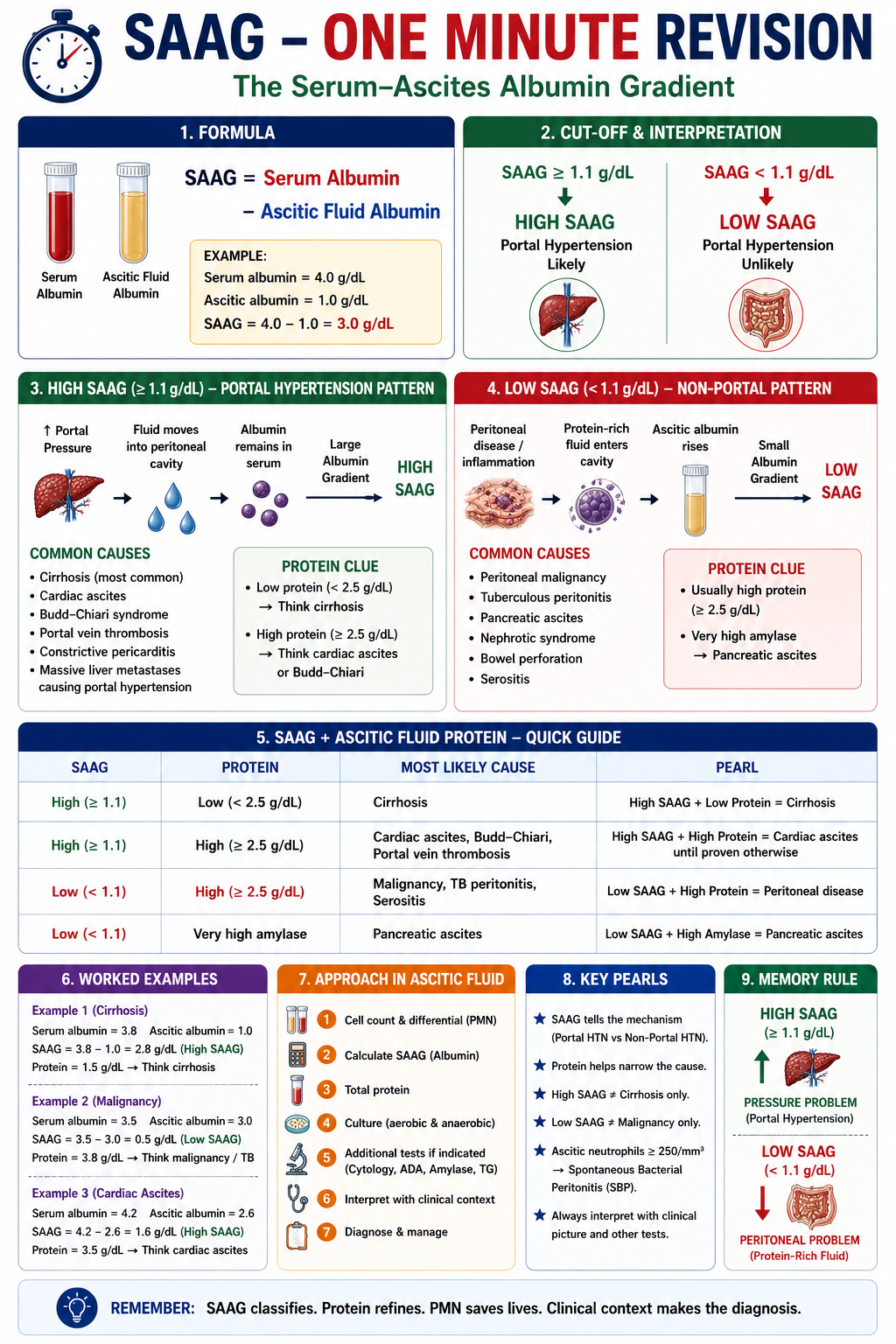
Key Takeaways
- SAAG = Serum Albumin − Ascitic Fluid Albumin (same-day samples)
- SAAG ≥1.1 g/dL indicates portal hypertension
- SAAG <1.1 g/dL indicates a non-portal hypertensive cause
- SAAG identifies the mechanism of ascites, not the final diagnosis
- Malignancy is usually low SAAG, but may be high SAAG if it causes portal hypertension
- High SAAG reflects elevated hydrostatic pressure forcing albumin-poor fluid into the peritoneal cavity
- Low SAAG reflects protein-rich fluid from peritoneal disease, malignancy or lymphatic obstruction
- High SAAG + low protein = cirrhosis; High SAAG + high protein = cardiac ascites or Budd–Chiari
- Low SAAG + high protein = malignancy or TB; Low SAAG + very high amylase = pancreatic ascites
- SAAG is superior to the older transudate/exudate classification
- SAAG must always be combined with cell count, protein, and culture for complete interpretation
- SBP is diagnosed by ascitic fluid neutrophil count ≥250 cells/mm³ — this takes clinical priority
Frequently Asked Questions
References
- Runyon BA, Montano AA, Akriviadis EA, et al. The serum-ascites albumin gradient is superior to the exudate-transudate concept in the differential diagnosis of ascites. Ann Intern Med. 1992;117(3):215–220.
- Runyon BA; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013;57(4):1651–1653.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460.
- Pare P, Talbot J, Hoefs JC. Serum-ascites albumin concentration gradient: a physiologic approach to the differential diagnosis of ascites. Gastroenterology. 1983;85(2):240–244.
- Moore KP, Aithal GP. Guidelines on the management of ascites in cirrhosis. Gut. 2006;55(Suppl 6):vi1–12.
- Akriviadis EA, Runyon BA. Utility of an algorithm in differentiating spontaneous from secondary bacterial peritonitis. Gastroenterology. 1990;98(1):127–133.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist hepatological input when investigating and managing patients with ascites.