Most students memorize: acute liver failure = INR > 1.5 + encephalopathy.
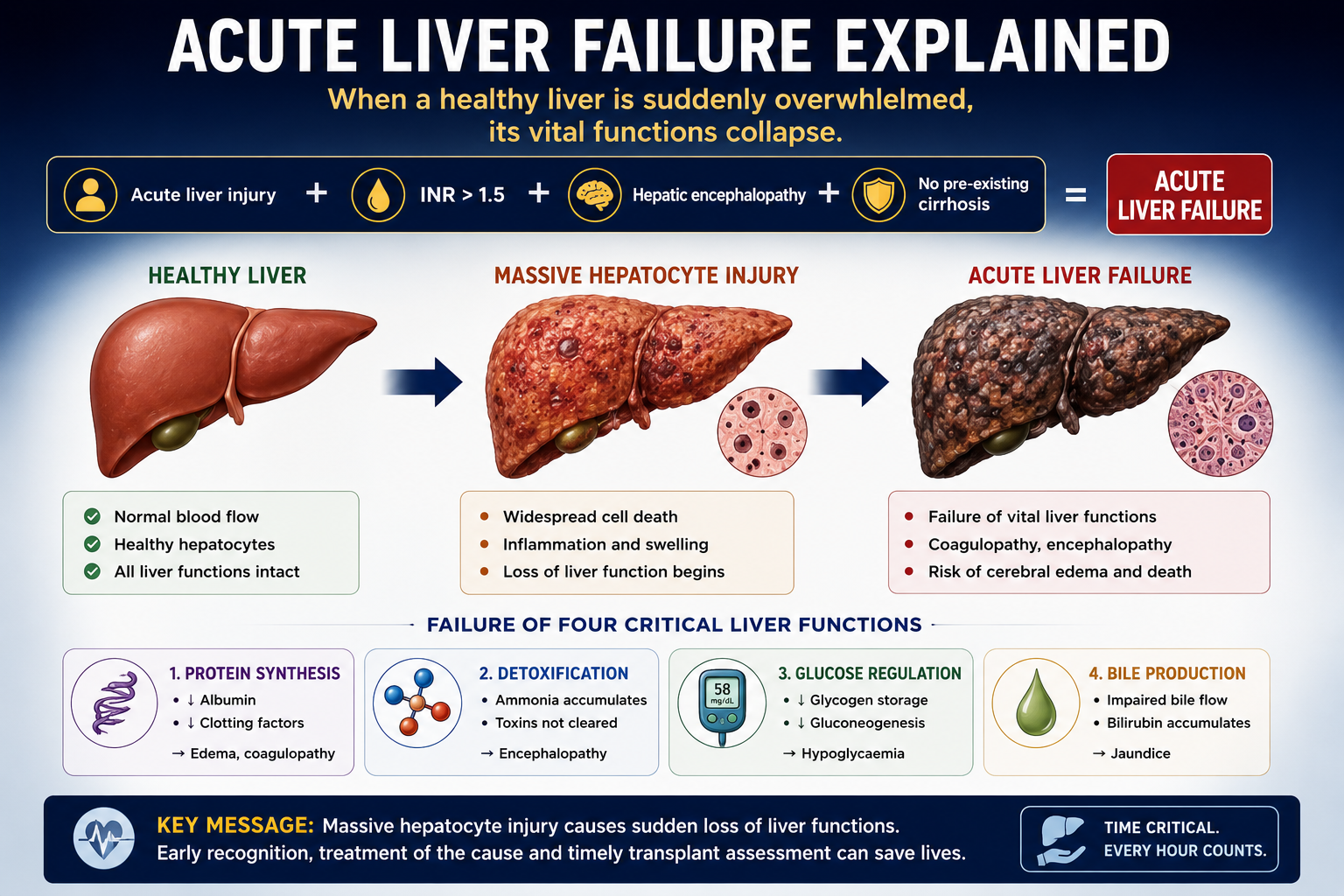
That definition is important, but it only becomes useful when you understand the mechanism. Acute liver failure is a sudden collapse of normal liver function after severe hepatocyte injury.
Once you know which liver function has failed, every clinical feature becomes logical.
Learning Objectives
- Define acute liver failure
- Explain major liver functions
- Explain coagulopathy, encephalopathy, cerebral edema and hypoglycaemia
- Recognize common causes
- Outline diagnosis, severity assessment and management
- Understand why early transplant assessment matters
What Is Acute Liver Failure?
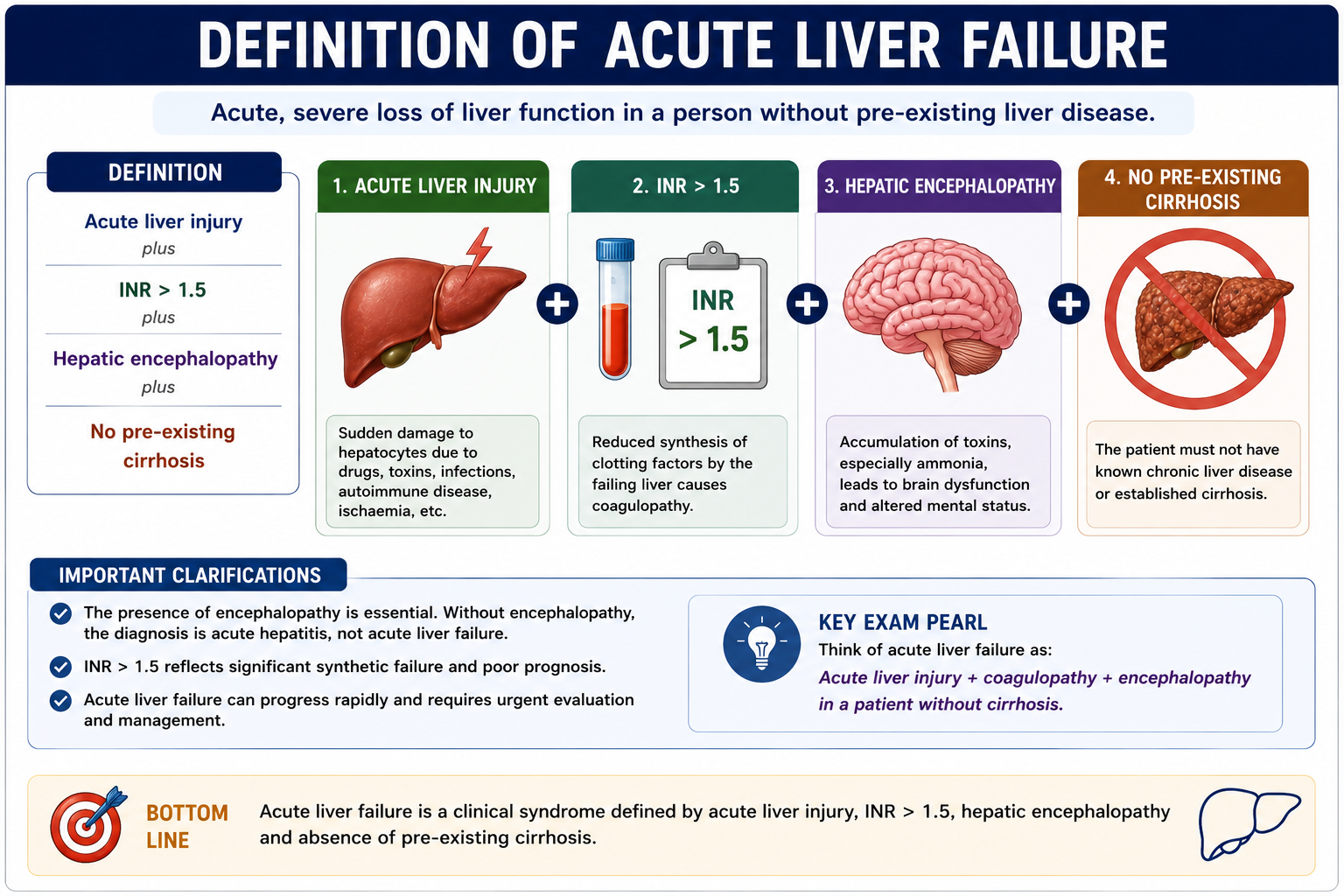
Acute liver failure is acute liver injury with INR > 1.5 and hepatic encephalopathy in a patient without pre-existing cirrhosis.
The presence of encephalopathy distinguishes acute liver failure from uncomplicated acute hepatitis. A patient may have very high transaminases but, without encephalopathy, they do not yet meet the usual clinical definition of acute liver failure.
Acute liver failure requires encephalopathy. INR elevation alone is acute severe hepatitis or acute liver injury, not full acute liver failure.
Hyperacute vs Acute vs Subacute Liver Failure
Acute liver failure can be classified by the time interval between jaundice and encephalopathy. This matters because the clinical course and prognosis are different.
Hyperacute liver failure progresses very rapidly, while subacute liver failure evolves more slowly and may have poorer spontaneous recovery.
| Type | Time from Jaundice to Encephalopathy | Typical Pattern |
|---|---|---|
| Hyperacute ALF | < 7 days | Rapid progression, high cerebral edema risk, but often better chance of spontaneous recovery if the cause is reversible |
| Acute ALF | 8-28 days | Intermediate pattern |
| Subacute ALF | 29-84 days, about 4-12 weeks | Slower progression, less cerebral edema than hyperacute ALF, but often poorer spontaneous recovery |
Hyperacute ALF often has more cerebral edema but may have better spontaneous recovery. Subacute ALF may look less dramatic early, but prognosis can be worse.

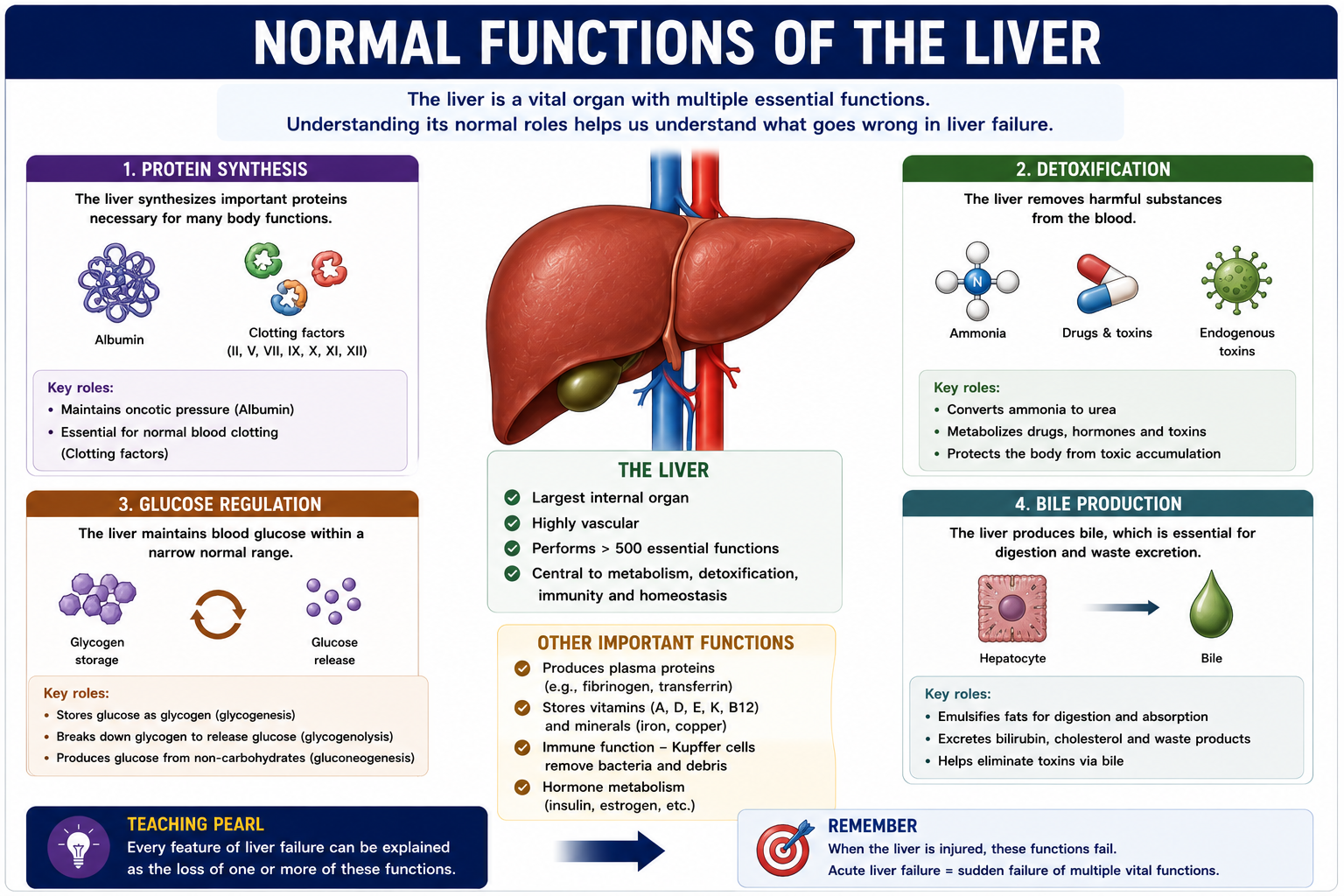
Normal Functions of the Liver
The easiest way to understand acute liver failure is to ask: which normal liver function has failed?
1. Protein Synthesis
The liver produces albumin and most clotting factors. When synthesis fails, INR rises and oncotic pressure may fall.
2. Detoxification
The liver detoxifies ammonia, drugs and toxins. When detoxification fails, neurotoxins reach the brain and encephalopathy develops.
3. Glucose Regulation
The liver stores glycogen and performs gluconeogenesis. When these fail, dangerous hypoglycaemia can occur.
4. Bile Production and Bilirubin Excretion
The liver produces bile and excretes bilirubin. When this fails, jaundice develops.
Acute liver failure is easiest to understand by asking: which liver function has failed?
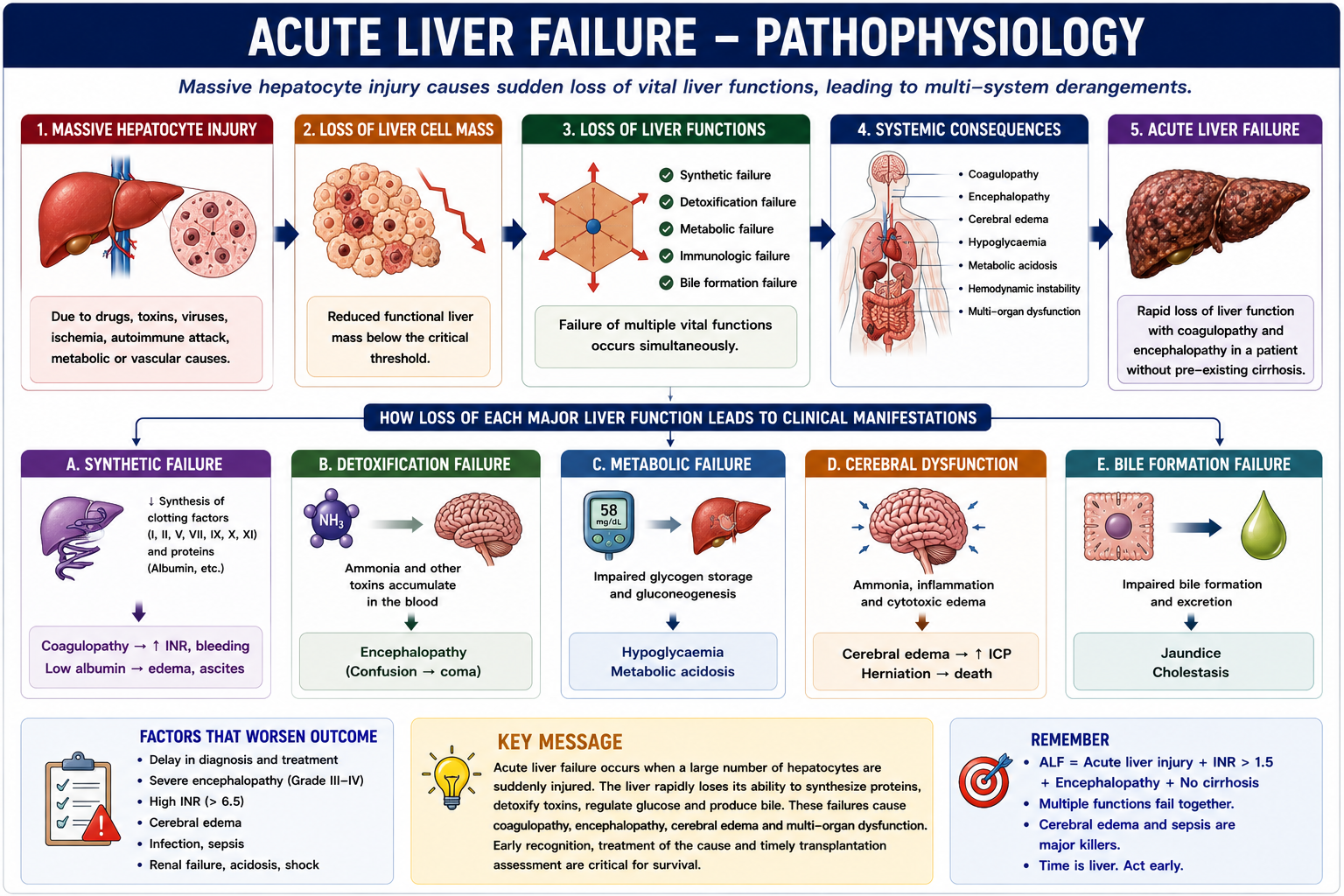
Pathophysiology of Acute Liver Failure
Acute liver failure occurs when a major insult destroys or disables enough hepatocytes that the liver can no longer perform essential physiological tasks.
This is why acute liver failure is not just a high ALT or AST. Transaminases signal hepatocyte injury; acute liver failure means the injury is severe enough to cause functional collapse.
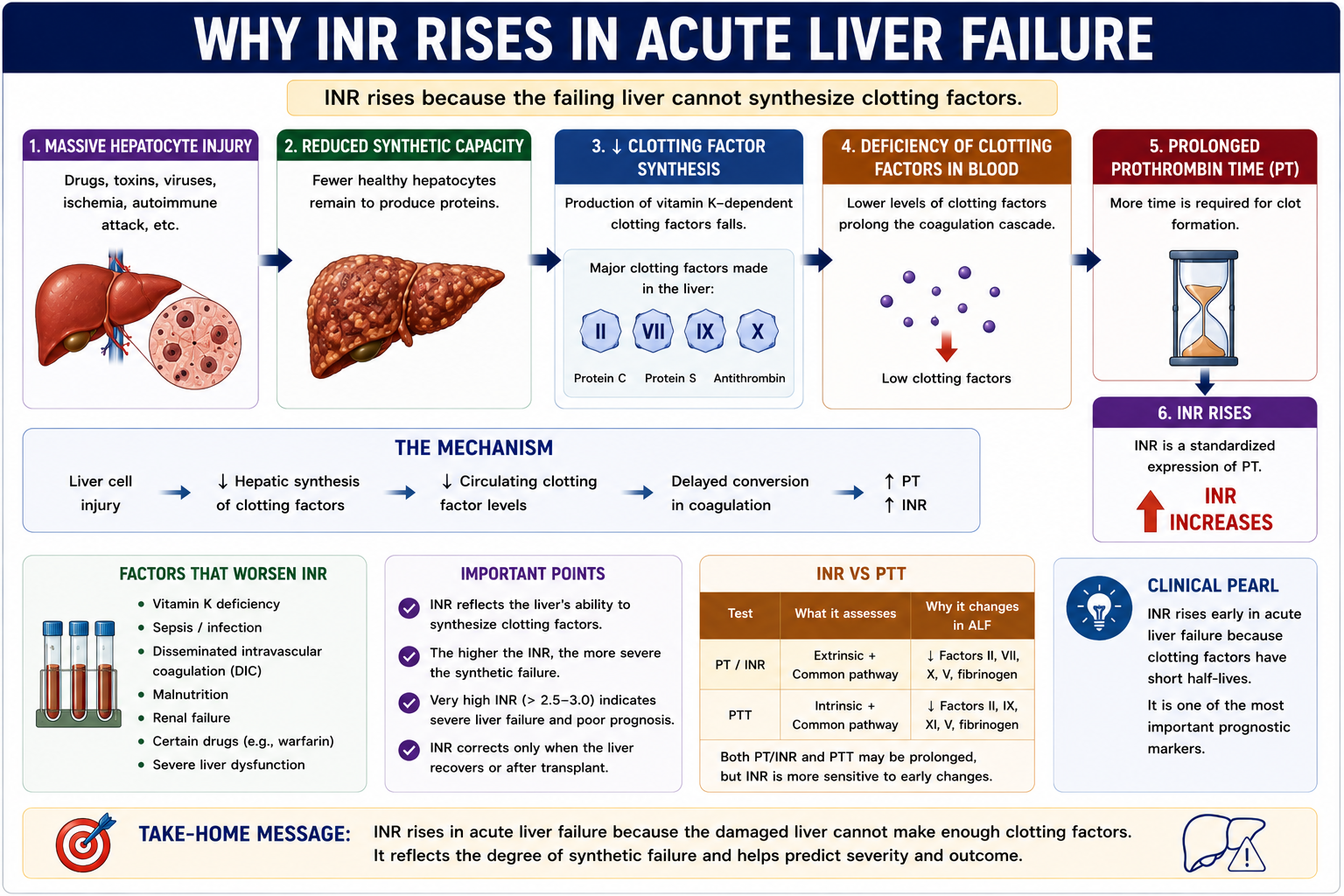
Why Does INR Rise?
The liver produces most clotting factors. When hepatocytes are destroyed, clotting factor production falls quickly because many clotting factors have short half-lives.
INR is therefore both a diagnostic feature and a key severity marker. A rising INR means worsening synthetic failure.
INR is one of the most important prognostic markers in acute liver failure.
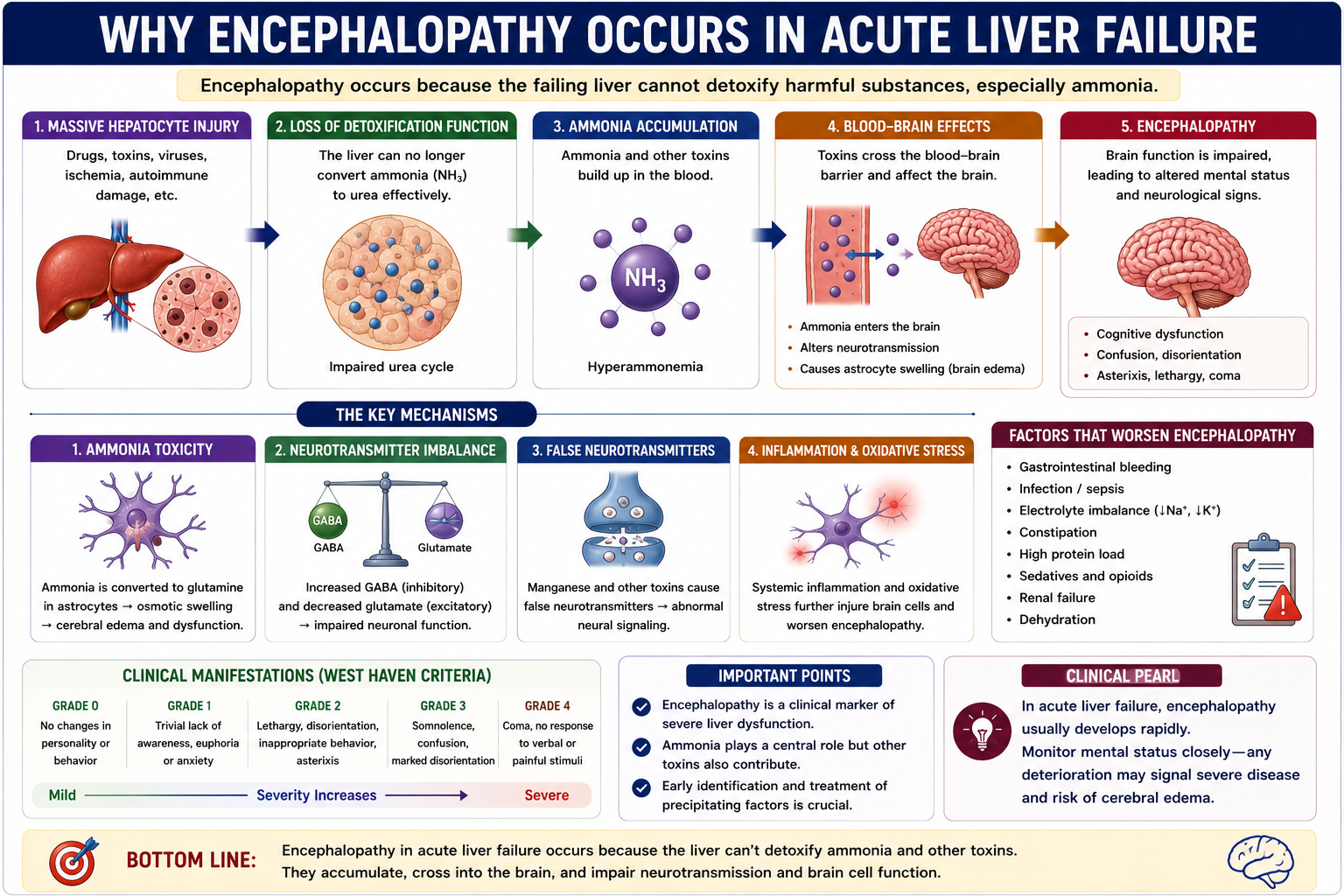
Why Does Encephalopathy Occur?
Encephalopathy occurs because detoxification fails. Ammonia and other gut-derived toxins are no longer cleared effectively and can impair brain function.
This is closely related to the concepts in Hepatic Encephalopathy Explained, but in acute liver failure it may evolve faster and carry a higher risk of cerebral edema.
Acute liver failure causes encephalopathy because toxins reach the brain.
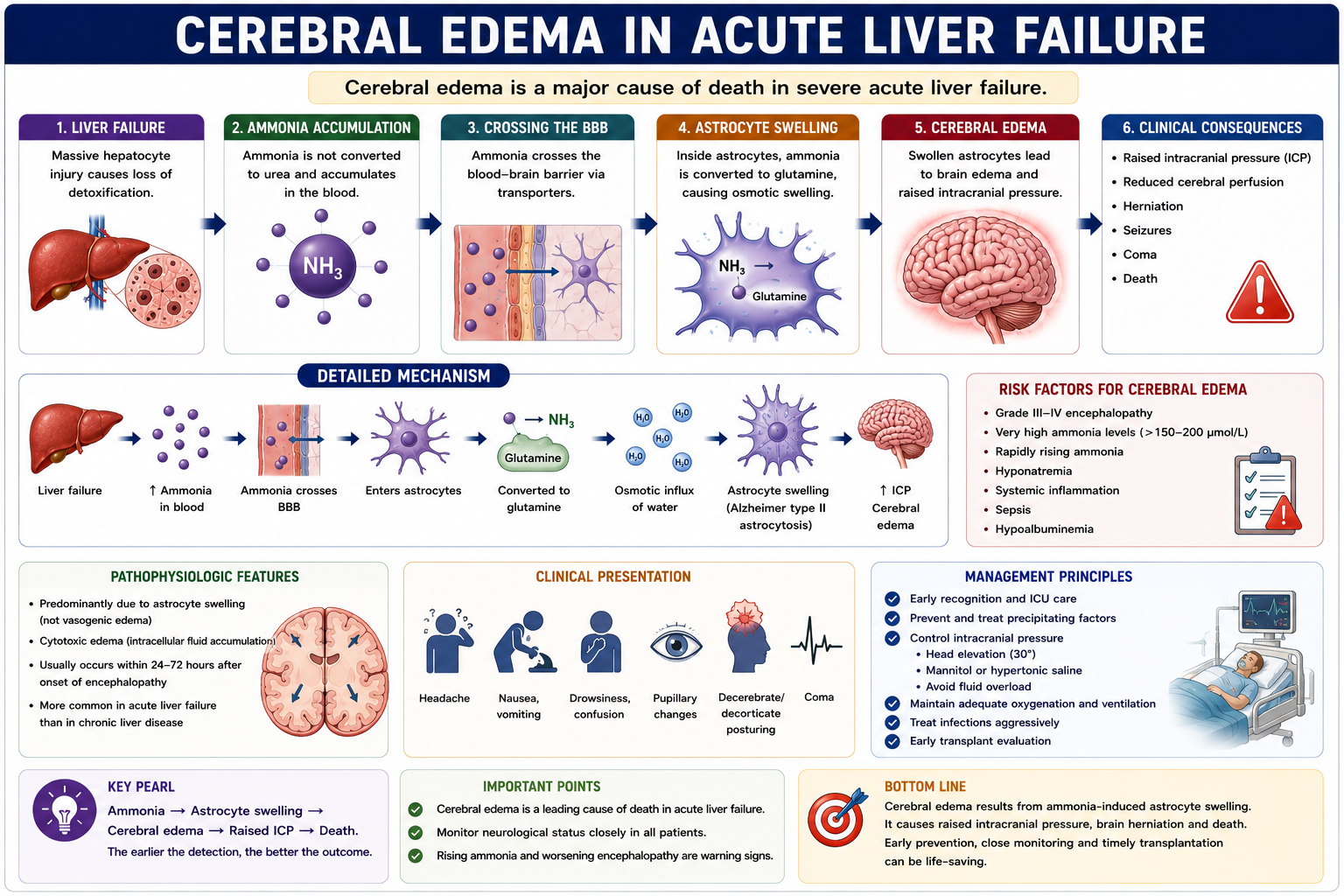
Why Does Cerebral Edema Occur?
Cerebral edema is one of the most feared complications of severe acute liver failure. Ammonia is converted within astrocytes to glutamine, drawing water into astrocytes and contributing to brain swelling.
Raised intracranial pressure can reduce cerebral perfusion and may progress to brain herniation. This is particularly important in hyperacute liver failure.
Cerebral edema is a major cause of death in severe acute liver failure.
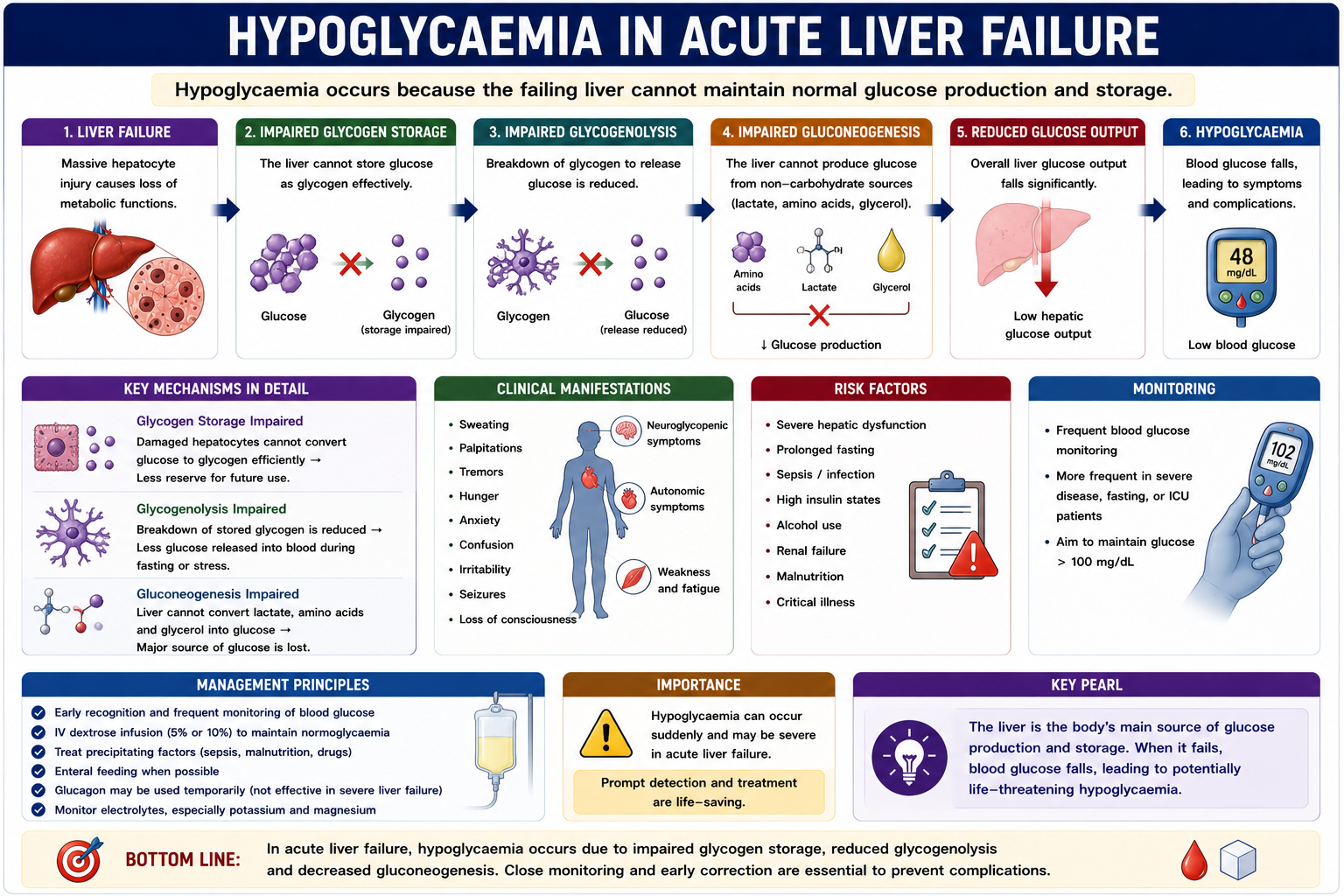
Why Does Hypoglycaemia Occur?
The liver is central to glucose homeostasis. It stores glycogen and produces glucose through gluconeogenesis during fasting or physiological stress.
When the liver fails, blood glucose may fall dangerously. Regular glucose monitoring is therefore a basic part of acute liver failure supportive care.
Why Does Jaundice Occur?
Jaundice occurs because the injured liver cannot process and excrete bilirubin normally.
Normally, hepatocytes take up bilirubin, conjugate it and excrete it into bile. In acute liver failure, hepatocyte injury and impaired bile formation cause bilirubin to accumulate in blood.
The phrase acute liver failure jaundice usually refers to bilirubin accumulation caused by severe hepatocyte dysfunction and impaired bile excretion.
In acute liver failure, jaundice reflects failed bilirubin handling, while INR reflects failed protein synthesis and encephalopathy reflects failed detoxification.

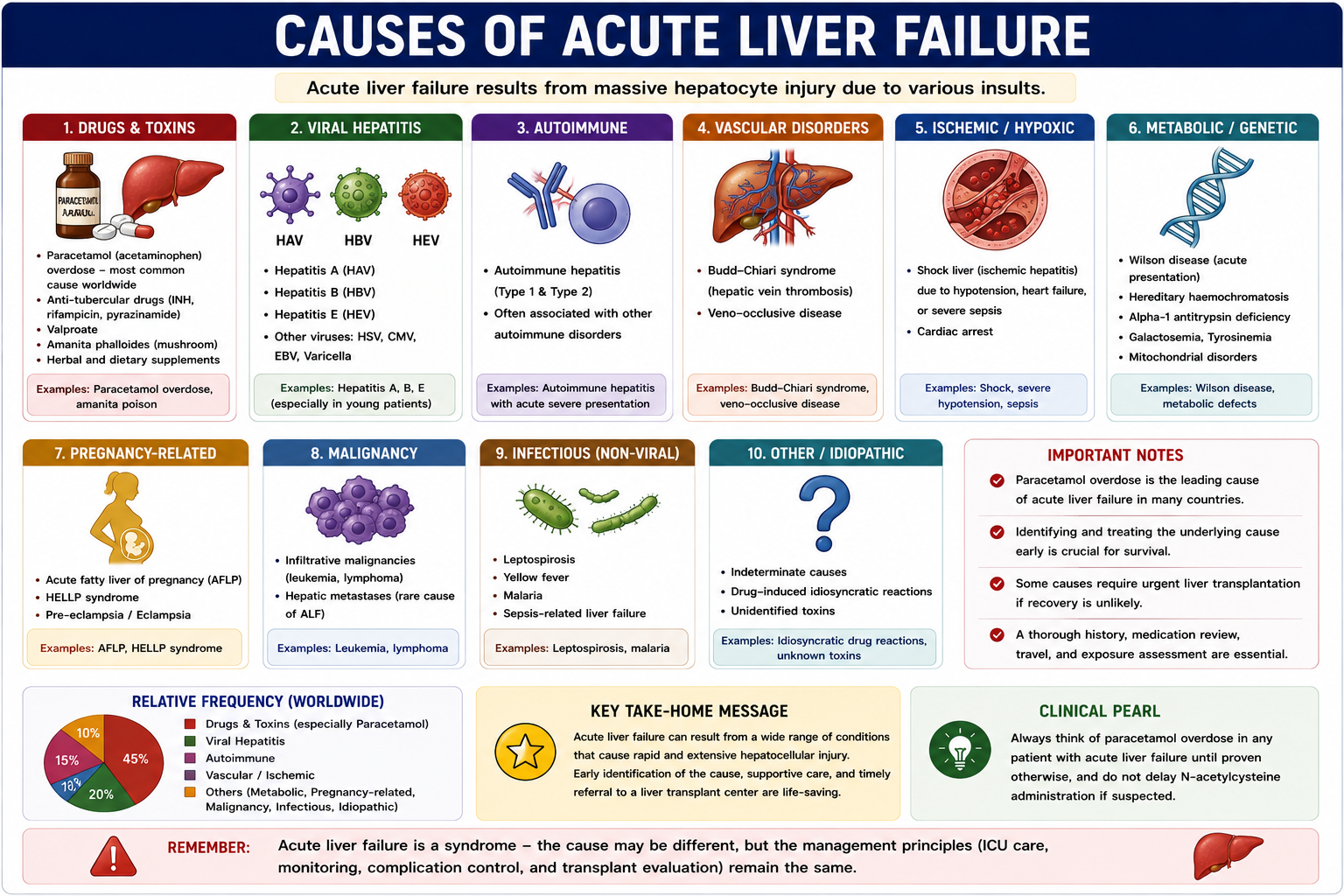
Causes of Acute Liver Failure
Causes vary by region, but paracetamol overdose is one of the most important causes worldwide. Always look for treatable causes early.
| Category | Examples |
|---|---|
| Drugs and toxins | Paracetamol overdose, idiosyncratic drug injury, herbal toxins, mushroom poisoning |
| Viral | Hepatitis A, B and E; herpes simplex virus in selected settings |
| Autoimmune | Autoimmune hepatitis |
| Vascular | Budd-Chiari syndrome, ischemic hepatitis or shock liver |
| Metabolic | Wilson disease, mitochondrial disorders |
| Pregnancy-related | Acute fatty liver of pregnancy, HELLP syndrome |
Paracetamol overdose is a major cause and is treatable with N-acetylcysteine when recognized early.
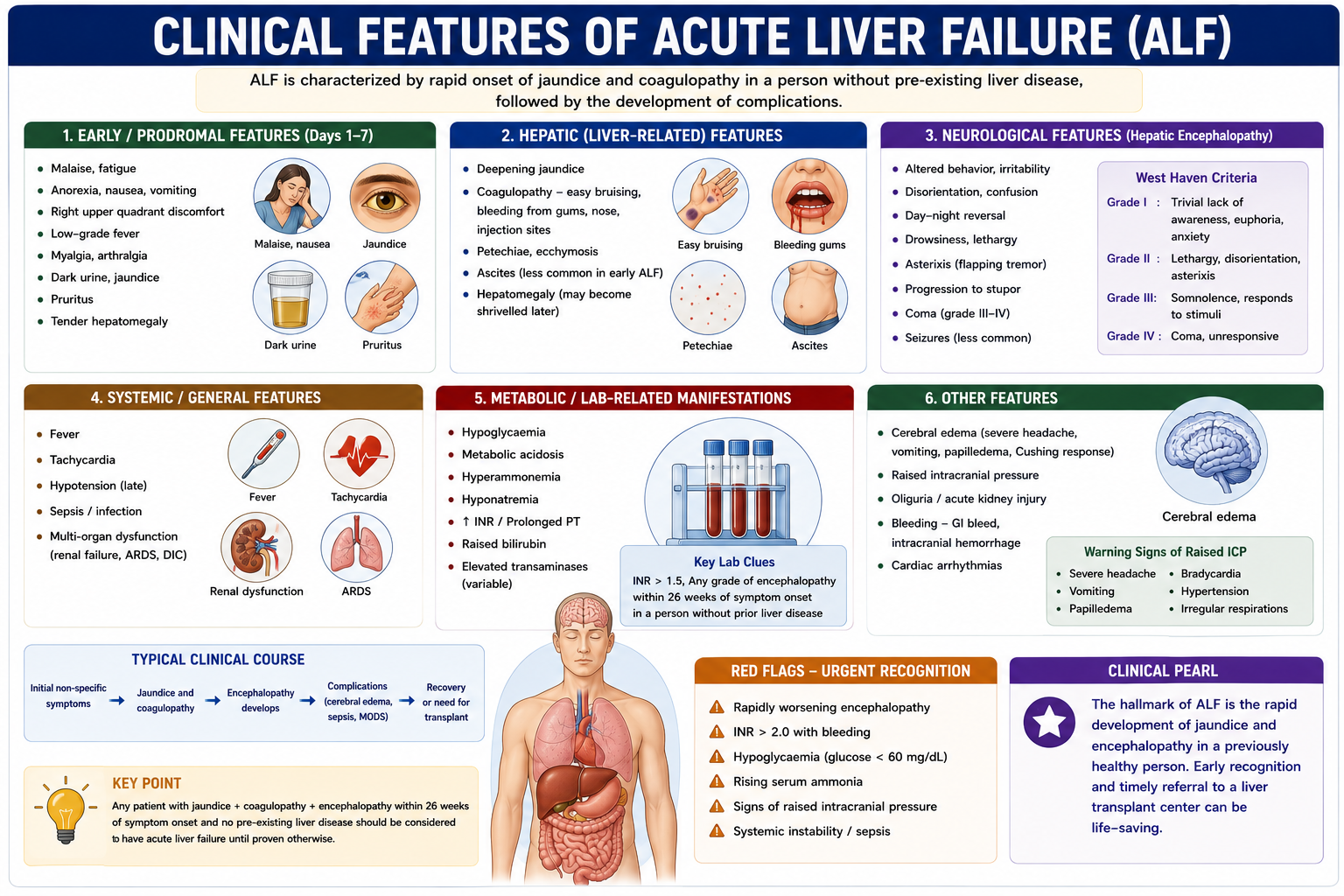
Clinical Features
Clinical features reflect loss of liver function and complications of systemic critical illness.
| Feature | Mechanism |
|---|---|
| Jaundice | Bilirubin accumulation |
| INR elevation | Clotting factor deficiency |
| Confusion or coma | Ammonia and toxins affecting the brain |
| Bleeding tendency | Coagulopathy and platelet dysfunction |
| Hypoglycaemia | Metabolic failure |
| Cerebral edema | Astrocyte swelling and raised intracranial pressure |
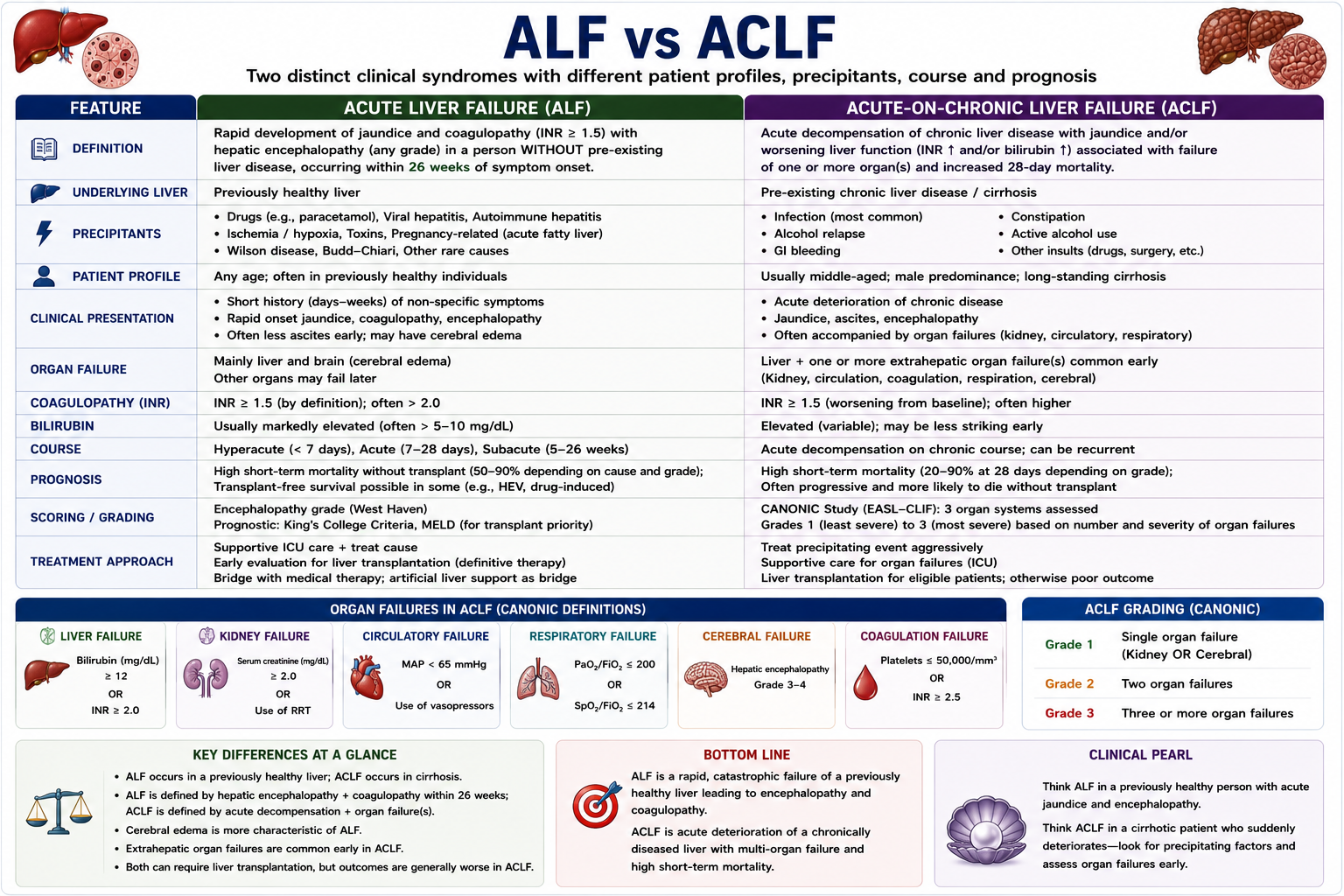
Acute Liver Failure vs Acute-on-Chronic Liver Failure
Acute liver failure occurs in a previously non-cirrhotic liver. Acute-on-chronic liver failure occurs when a patient with chronic liver disease acutely deteriorates.
| Acute Liver Failure | Acute-on-Chronic Liver Failure |
|---|---|
| No pre-existing cirrhosis | Cirrhosis or chronic liver disease present |
| New severe liver injury | Acute deterioration of existing disease |
| Sudden loss of liver function | Often precipitated by infection, alcohol, bleeding or drugs |
| Potential recovery or emergency transplant | Often poorer prognosis due to limited baseline reserve |
ALF occurs in a previously non-cirrhotic liver.
Diagnosis
Diagnosis requires both recognition of the syndrome and urgent identification of the cause.
- Liver function tests and bilirubin
- PT/INR and full blood count
- Glucose, electrolytes, renal function, ABG and lactate
- Ammonia when encephalopathy or cerebral edema risk is a concern
- Paracetamol level and toxicology screen
- Viral serology and autoimmune markers
- Ceruloplasmin and haemolysis screen when Wilson disease is suspected
- Pregnancy test when relevant
- Ultrasound with Doppler to assess liver, portal vein and hepatic venous flow

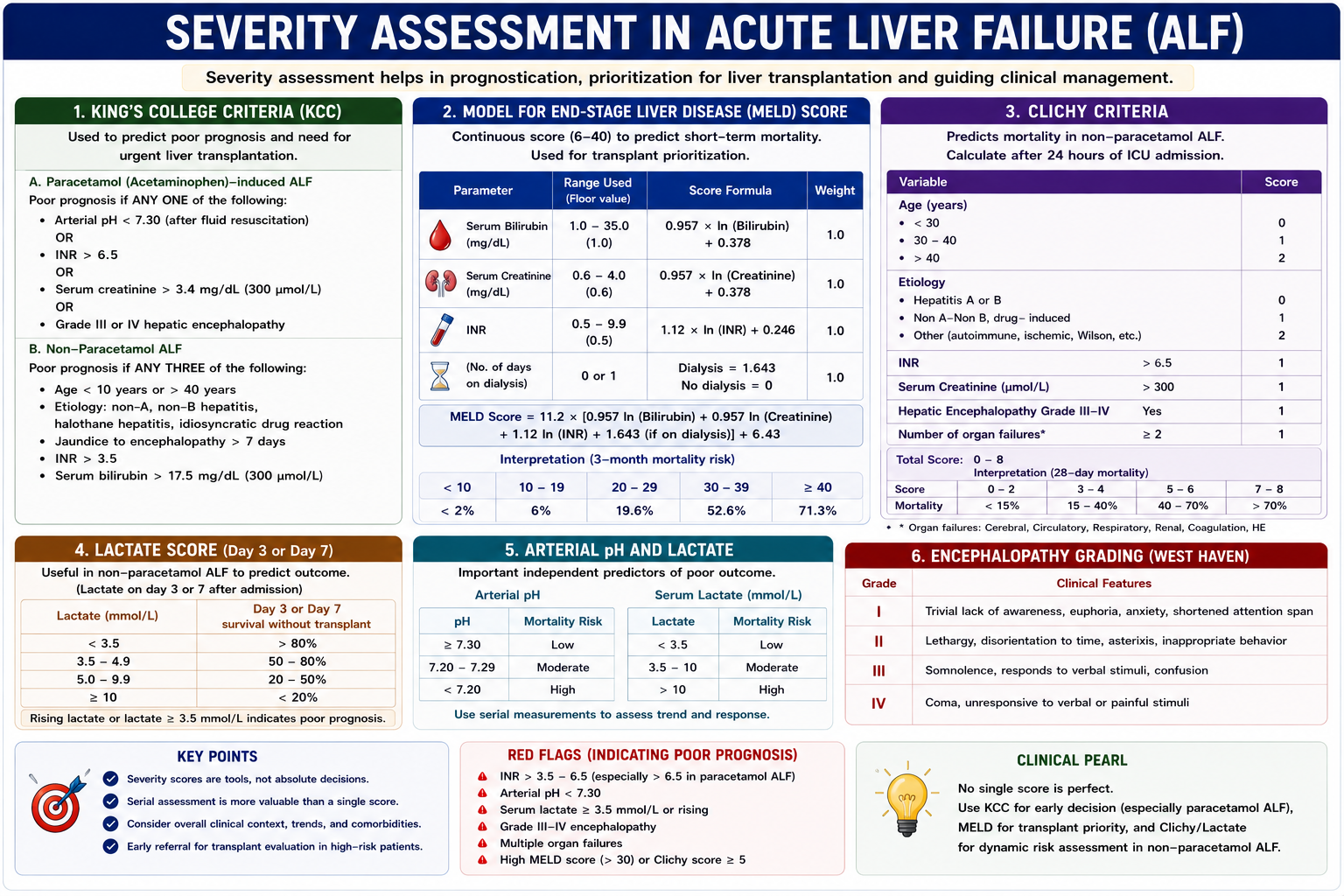
Acute Liver Failure Severity Assessment
Severity assessment identifies patients who need intensive care, transplant-center transfer and possible emergency liver transplantation.
- INR - marker of synthetic failure
- Encephalopathy grade - marker of neurological severity
- Ammonia - helps assess risk of cerebral edema
- Lactate and pH - markers of systemic and mitochondrial stress
- Renal function - kidney injury worsens prognosis
- Cerebral edema - life-threatening neurological complication
Severity assessment identifies patients who need transplantation.
Management Overview
Acute liver failure is a medical emergency. Management is supportive, cause-specific and transplant-focused from the beginning.
Treat the Cause
Give N-acetylcysteine for suspected or confirmed paracetamol toxicity. Consider antivirals for selected viral causes and corticosteroids for selected autoimmune hepatitis cases under specialist guidance.
Supportive Care
Monitor glucose closely, correct electrolytes, avoid unnecessary sedation, treat seizures, monitor renal function and maintain infection surveillance.
Cerebral Edema Management
Use head elevation, avoid overhydration, maintain appropriate sodium targets, and use hypertonic saline or other specialist measures when indicated. Intracranial pressure monitoring is individualized in specialist centers.
Early Specialist Referral
Patients with encephalopathy or worsening coagulopathy should be discussed early with a liver transplant center because deterioration can be rapid.

When Is Liver Transplant Needed?
Liver transplantation is needed when the chance of spontaneous recovery is low and death is likely without replacement of the failing liver.
King's College Criteria are commonly used to help identify patients with poor prognosis in paracetamol and non-paracetamol acute liver failure. They should guide assessment, not replace specialist judgment.
King's College Criteria acute liver failure assessment is mainly about prognosis and transplant need, not diagnosis.
Transplant evaluation should occur early, before irreversible neurological or multi-organ complications develop.
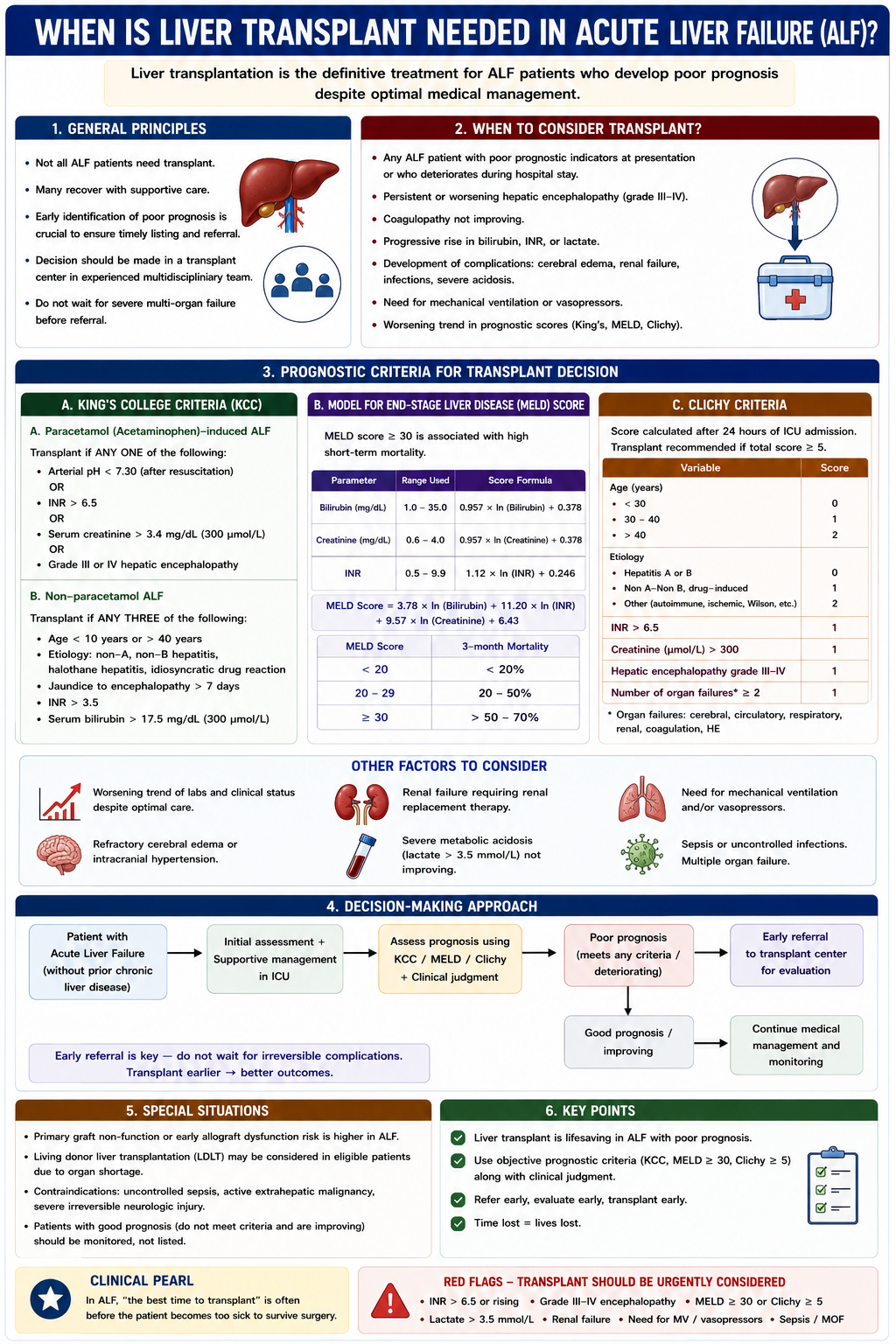
King's College Criteria: What Is the Purpose?
King's College Criteria are not used to diagnose acute liver failure. They are used to identify patients with poor prognosis who may need emergency liver transplantation.
King's College Criteria help decide prognosis and transplant need. They do not replace clinical judgment or specialist transplant-center assessment.

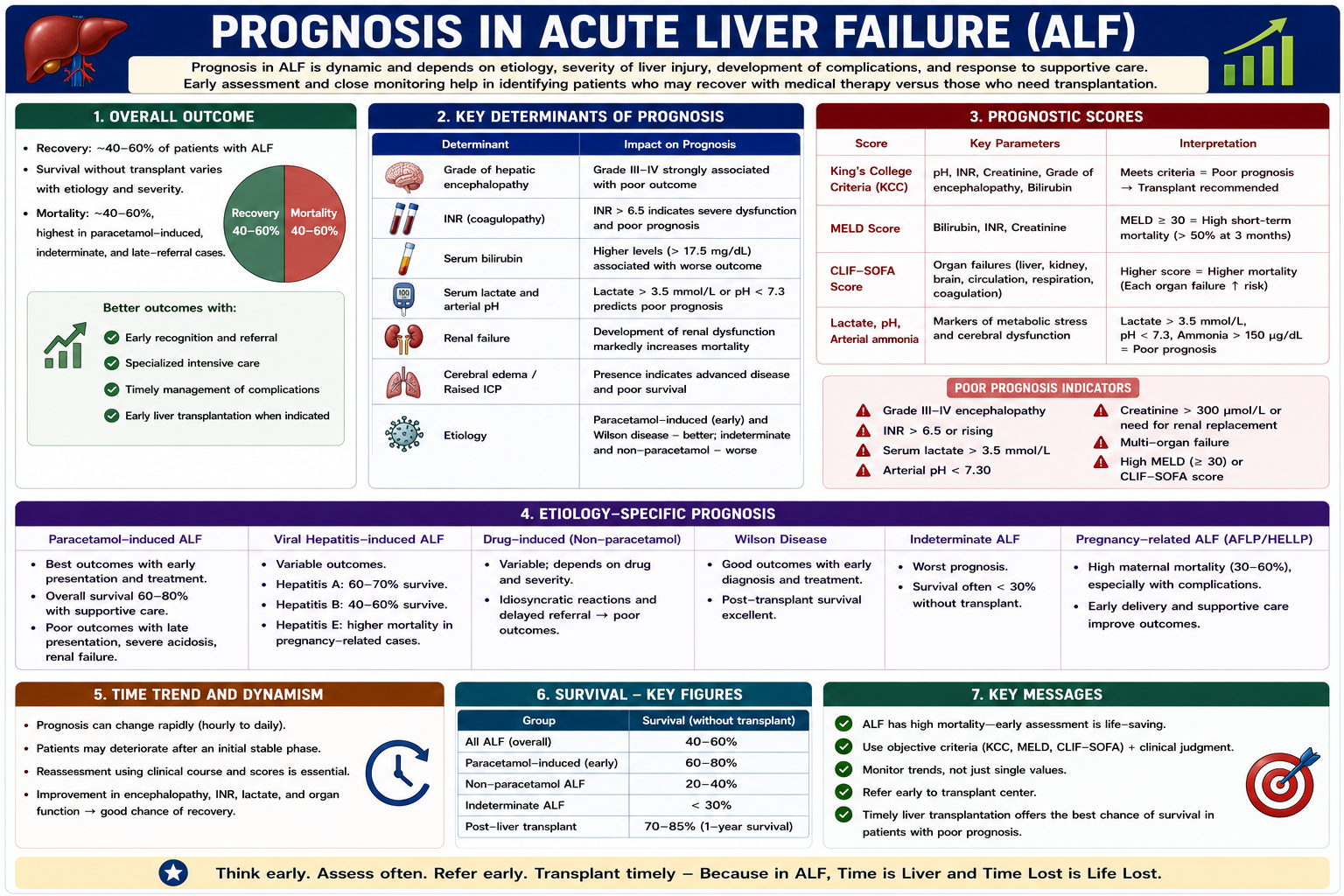
Prognosis
Outcome depends on the cause, speed of progression, severity of encephalopathy, INR, lactate, renal function and whether cerebral edema develops.
Understanding acute liver failure prognosis by cause is important because paracetamol-related ALF, viral ALF, Wilson disease and indeterminate ALF behave differently.
Cause-Specific Prognosis
| Cause | General Prognostic Pattern |
|---|---|
| Paracetamol overdose | Often good if recognized early and treated promptly with N-acetylcysteine; poor if delayed with severe acidosis, renal failure or cerebral edema |
| Hepatitis A | Often good with supportive care, though severe cases can require transplantation |
| Hepatitis B | Variable; severe cases may require antiviral therapy and transplant assessment |
| Wilson disease | Often poor without urgent transplantation when fulminant liver failure develops |
| Indeterminate ALF | Often poorer prognosis because cause-specific treatment may not be available |
| Budd-Chiari syndrome | Depends on rapid recognition and ability to restore or decompress hepatic venous outflow |
| Pregnancy-related ALF | Can improve after delivery and intensive supportive care, but severe cases remain high risk |
Prognosis depends not only on how severe the liver failure is, but also on whether the cause is rapidly reversible.
| Better Prognosis | Worse Prognosis |
|---|---|
| Early diagnosis | Delayed diagnosis |
| Lower INR | Very high INR |
| No cerebral edema | Cerebral edema or raised ICP |
| Reversible cause | Irreversible cause or delayed antidote |
Complications
- Cerebral edema and raised intracranial pressure
- Seizures
- Bleeding
- Hypoglycaemia
- Infection and sepsis
- Renal failure
- Multi-organ failure and death
High-Yield Exam Pearls
- Acute liver failure requires encephalopathy.
- INR > 1.5 is essential to the usual definition.
- Massive hepatocyte injury causes loss of liver functions.
- Coagulopathy results from reduced clotting factor synthesis.
- Encephalopathy results from failed detoxification.
- Cerebral edema is a major cause of death.
- Paracetamol overdose is a major cause and N-acetylcysteine is time-critical.
- King's College Criteria help guide transplant assessment.
- Early referral to a transplant center is critical.
Frequently Asked Questions
One-Minute Acute Liver Failure Revision
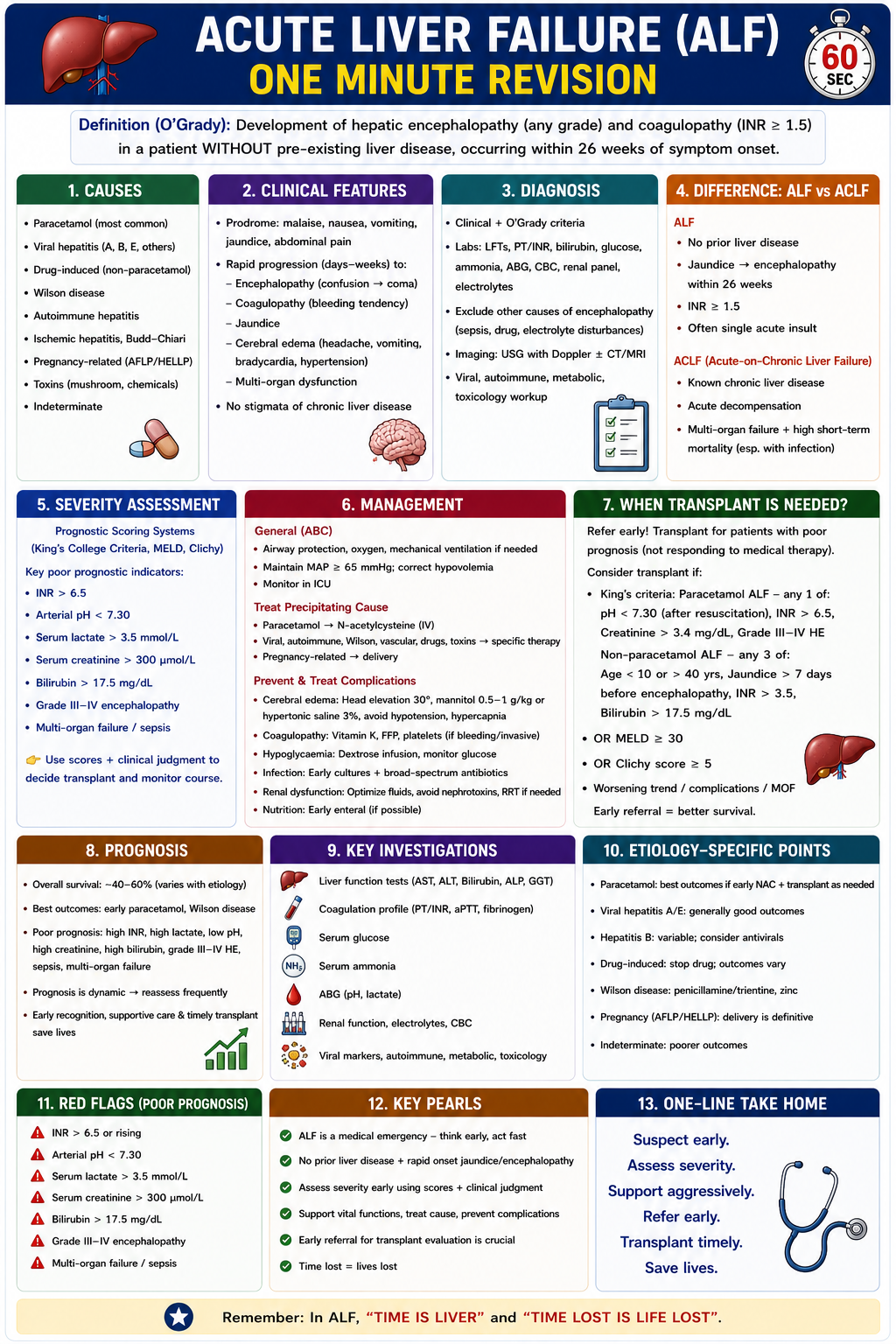
Key Takeaways
- Acute liver failure is acute liver injury with INR > 1.5 and encephalopathy without pre-existing cirrhosis.
- It is best understood as sudden loss of synthesis, detoxification and metabolism.
- INR rises because clotting factor synthesis fails.
- Encephalopathy and cerebral edema occur because detoxification fails and ammonia accumulates.
- Paracetamol overdose is a major treatable cause.
- Management requires ICU care, cause-specific treatment, complication monitoring and early transplant assessment.
Acute liver failure is sudden functional collapse of a previously non-cirrhotic liver. Remember the core triad: acute liver injury + INR > 1.5 + encephalopathy. Every major complication reflects loss of a liver function: failed synthesis causes INR rise, failed detoxification causes encephalopathy and cerebral edema, failed metabolism causes hypoglycaemia, and failed bilirubin handling causes jaundice. Early cause-specific treatment, ICU care and transplant-center discussion can save lives.
References
- Wendon J, Cordoba J, Dhawan A, et al. EASL Clinical Practical Guidelines on the management of acute (fulminant) liver failure. J Hepatol. 2017;66(5):1047-1081.
- Polson J, Lee WM; American Association for the Study of Liver Disease. AASLD position paper: the management of acute liver failure. Hepatology. 2005;41(5):1179-1197.
- Lee WM, Stravitz RT, Larson AM. Introduction to the revised American Association for the Study of Liver Diseases position paper on acute liver failure 2011. Hepatology. 2012;55(3):965-967.
- O'Grady JG, Alexander GJ, Hayllar KM, Williams R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology. 1989;97(2):439-445.
- Bernal W, Wendon J. Acute liver failure. N Engl J Med. 2013;369(26):2525-2534.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Acute liver failure is a medical emergency requiring urgent specialist hepatology and transplant-center input.
- Definition
- ALF Time Course
- Normal Liver Functions
- Pathophysiology
- Why INR Rises
- Encephalopathy
- Cerebral Edema
- Hypoglycaemia
- Why Jaundice Occurs
- Causes
- Clinical Features
- ALF vs ACLF
- Diagnosis
- Severity Assessment
- Management
- Transplant
- Prognosis
- Complications
- Exam Pearls
- FAQ
- One-Minute Revision
- Key Takeaways
- References