Most students know that TIPS treats variceal bleeding.
Few understand why it works.
TIPS works because it solves the underlying pressure problem — not by directly treating varices or removing ascitic fluid, but by creating a shortcut that allows portal blood to bypass the high-resistance cirrhotic liver. When portal pressure falls, its complications follow.
This article is a pathophysiology-first explanation of TIPS. Understanding the mechanism is everything.
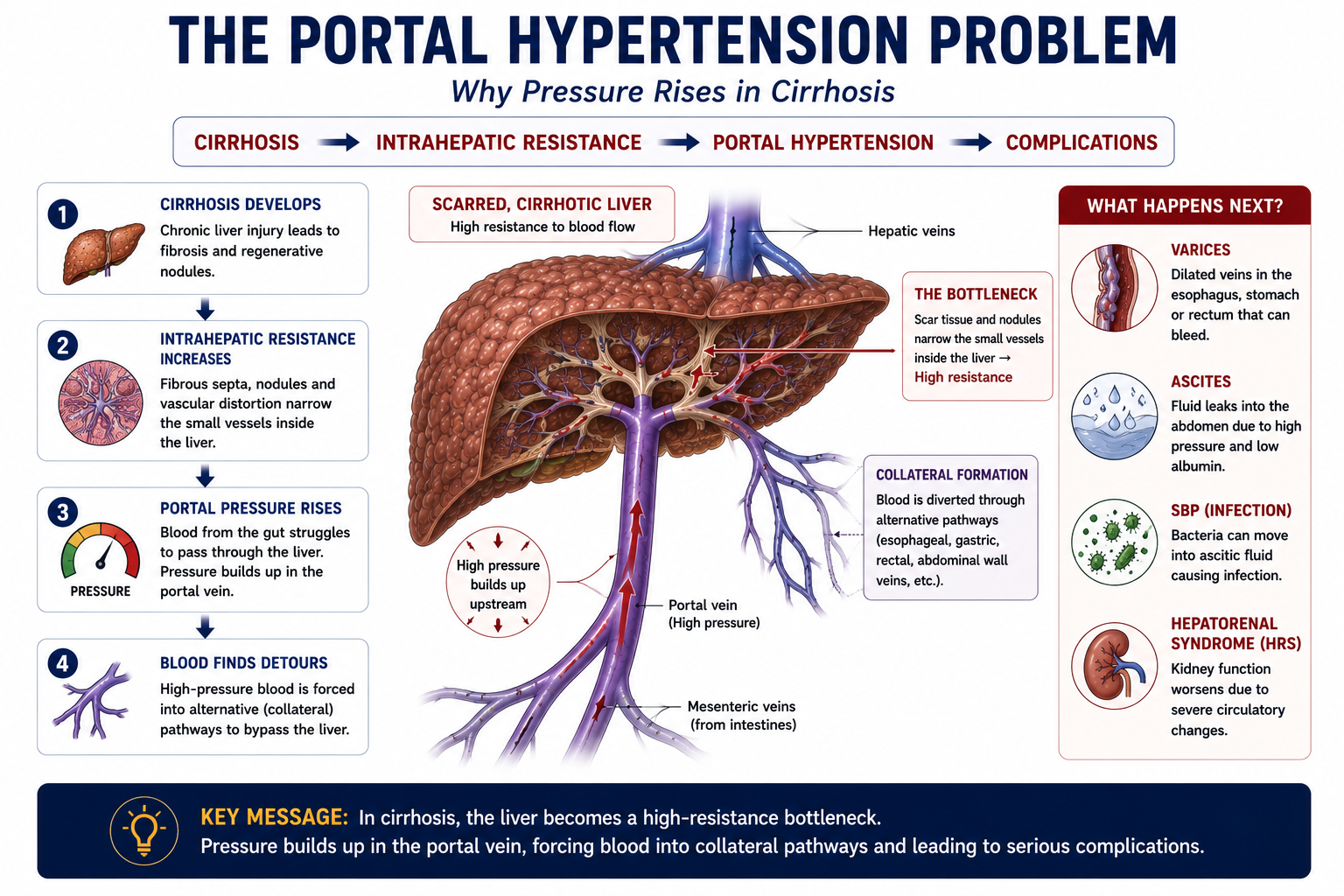
Branch 1: Portal hypertension → ascites → SBP → hepatorenal syndrome
Branch 2: Portal hypertension → portosystemic collaterals → varices → variceal bleeding
TIPS: Treats portal hypertension directly — improving both branches simultaneously
Learning Objectives
- Define TIPS and explain what the acronym stands for
- Explain how TIPS works and why portal pressure falls after the procedure
- Understand why cirrhosis creates the need for TIPS
- Identify the major indications for TIPS
- Explain why TIPS improves both ascites and variceal bleeding
- Understand why hepatic encephalopathy can worsen after TIPS
- Recognise key complications and contraindications
- Distinguish TIPS from paracentesis and liver transplantation
What Is TIPS?
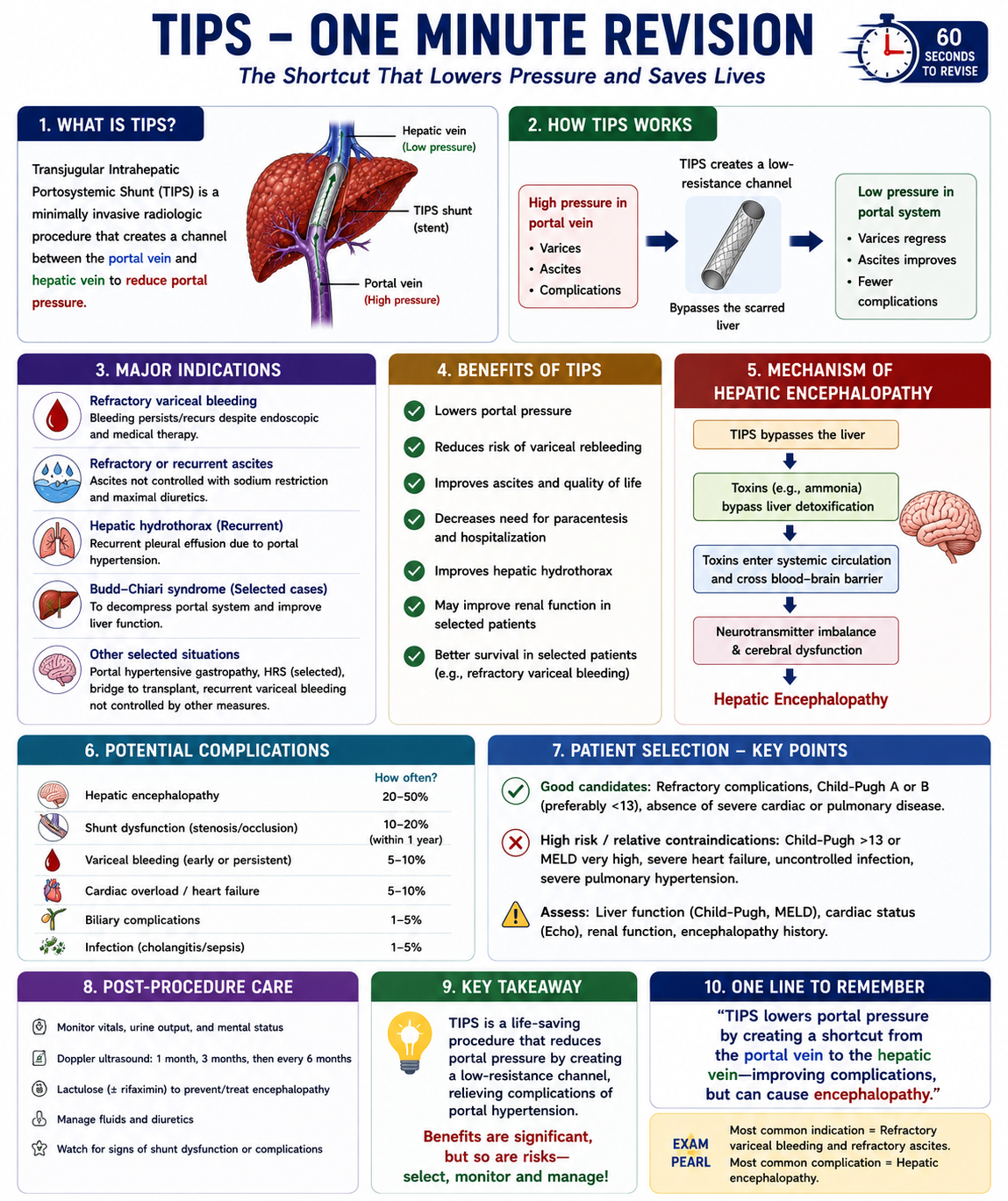
TIPS stands for Transjugular Intrahepatic Portosystemic Shunt.
Breaking down the name explains the procedure:
| Word | Meaning |
|---|---|
| Transjugular | Access is via the internal jugular vein — the entry point for the catheter |
| Intrahepatic | The channel passes through liver tissue |
| Portosystemic | Connects the portal venous system to the systemic venous circulation |
| Shunt | An artificial bypass channel maintained open by a stent |
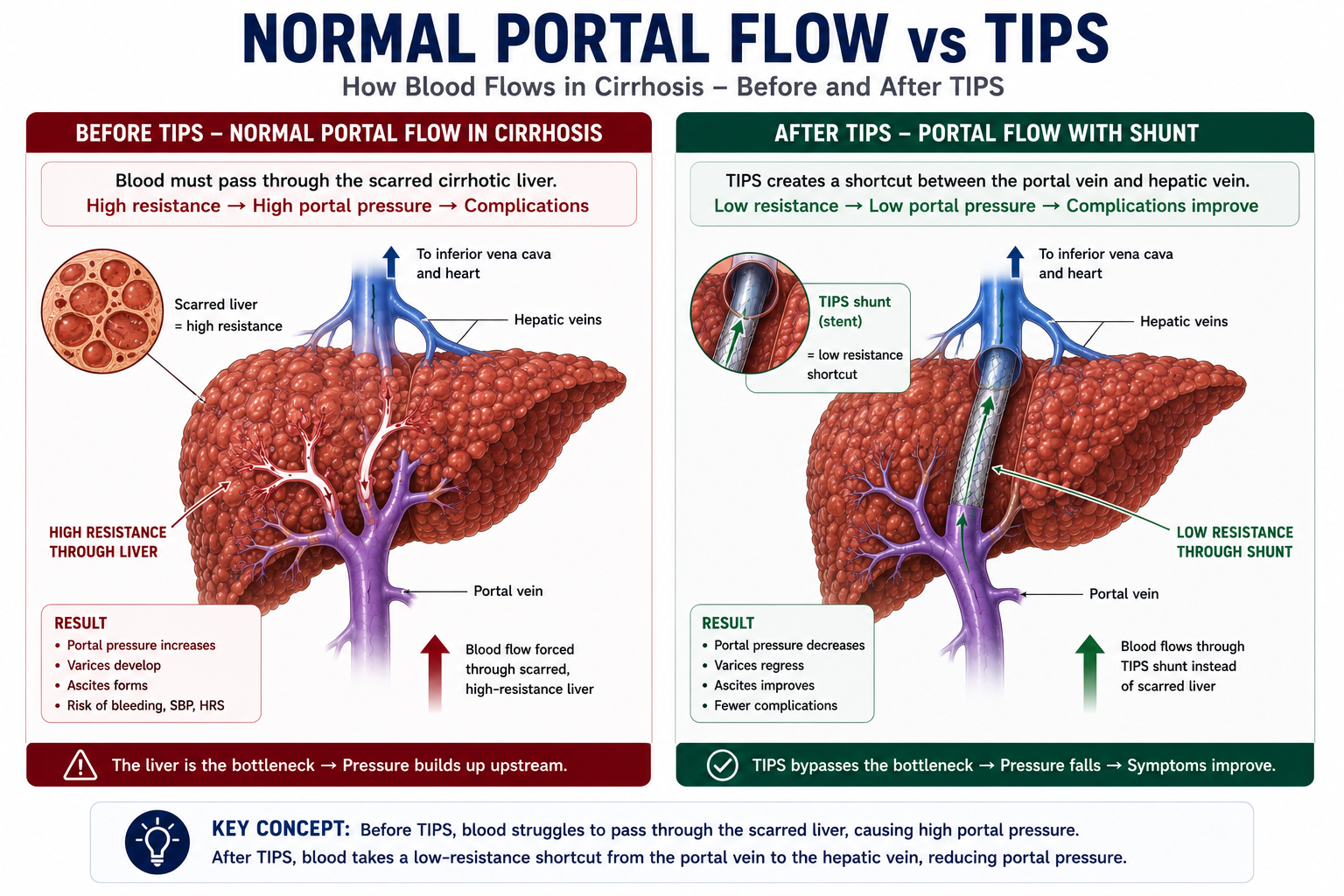
In practical terms: a stent is placed inside the liver connecting the portal vein (high-pressure) to the hepatic vein (low-pressure). Portal blood can now flow directly into the systemic circulation without passing through diseased liver tissue.
TIPS does not cure cirrhosis. It treats the consequences of portal hypertension by reducing portal pressure. The underlying liver disease, fibrosis, and hepatocyte dysfunction remain unchanged.
Why Is TIPS Needed?
To understand TIPS, start with why portal pressure rises in cirrhosis.
In a healthy liver, portal blood flows easily through the hepatic sinusoids. In cirrhosis, progressive scarring and architectural distortion create resistance. Blood struggles to pass through. Pressure builds upstream in the portal system.
The cirrhotic liver becomes the bottleneck. Blood cannot pass through efficiently, and pressure builds upstream. The complications of portal hypertension — ascites, variceal bleeding, SBP and hepatorenal syndrome — are all downstream consequences of this raised upstream pressure.
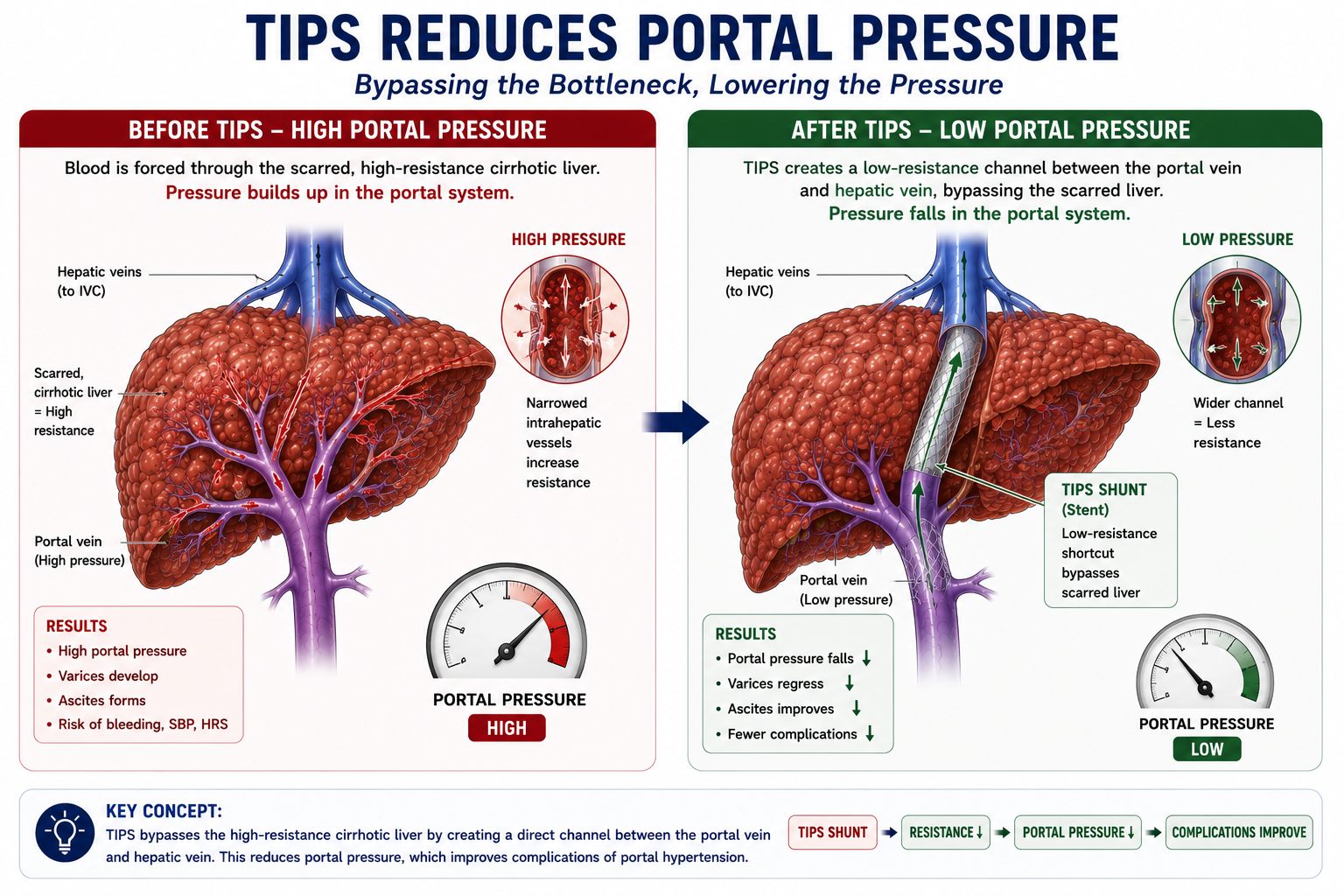
TIPS solves the pressure problem. Instead of forcing blood through a scarred, high-resistance liver, TIPS creates a shortcut around the resistance. Portal blood diverts through the stent directly into the hepatic vein, and portal pressure falls.
How Does TIPS Work?
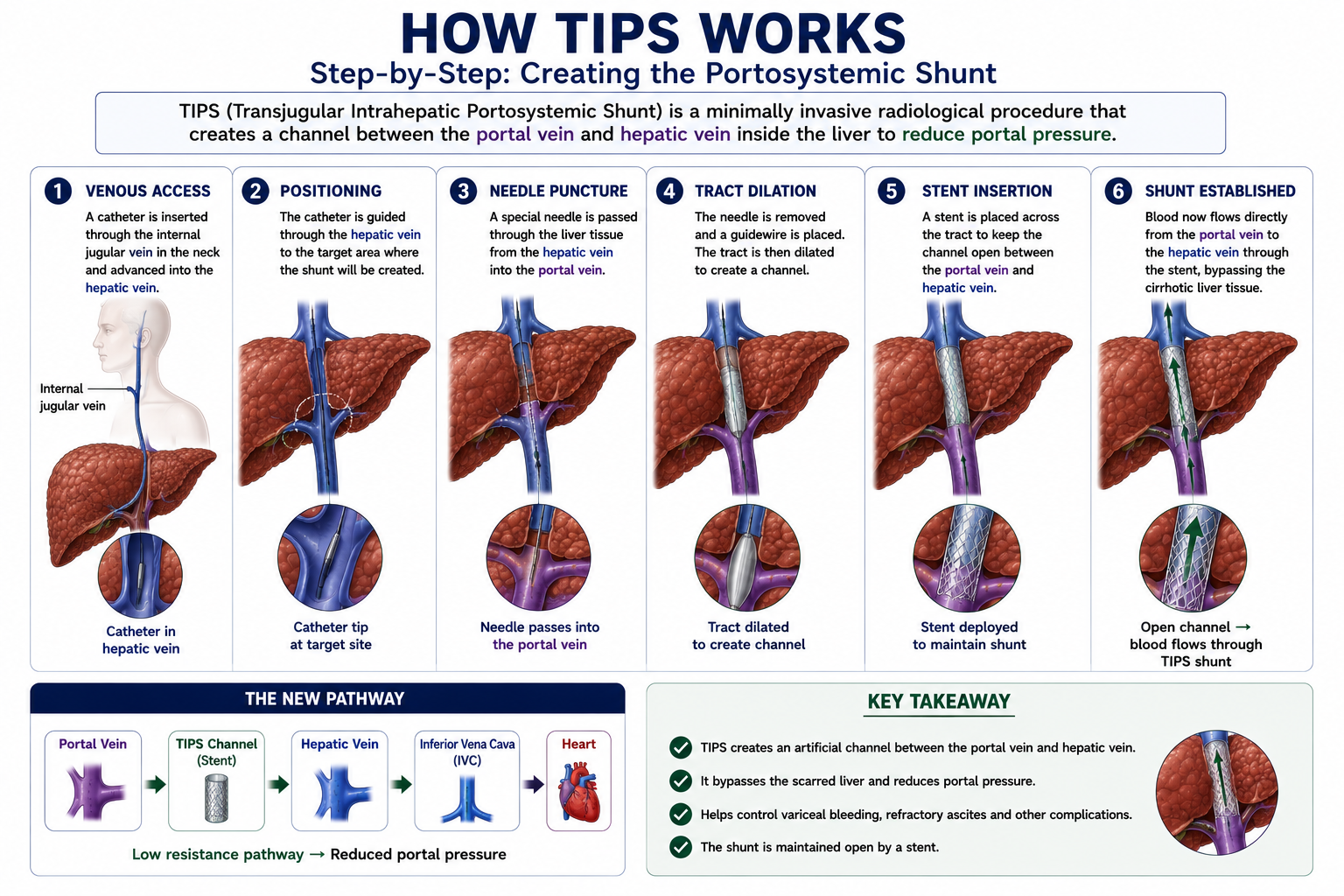
TIPS is performed by an interventional radiologist, typically under conscious sedation and imaging guidance. Understanding the steps explains why the procedure is called transjugular and intrahepatic.
- 1Access via the internal jugular vein. A catheter is introduced into the right internal jugular vein in the neck.
- 2Catheter reaches the hepatic vein. The catheter is advanced through the superior vena cava, right atrium, and inferior vena cava into a hepatic vein inside the liver.
- 3Needle passes into the portal vein. From the hepatic vein, a needle is advanced through liver tissue to puncture a branch of the portal vein.
- 4Tract created and dilated. A guidewire is passed through the needle, and the tract through the liver is dilated to create a channel.
- 5Stent inserted. A metal stent — typically a covered (polytetrafluoroethylene-lined) expandable stent — is deployed to keep the channel open.
- 6Portal blood flows directly to the hepatic vein. Blood now flows from the portal vein through the stent into the hepatic vein and then into the inferior vena cava, bypassing the diseased liver parenchyma.
The jugular approach allows the radiologist to navigate downstream from the hepatic vein into the portal vein — working with the venous anatomy rather than against it. It avoids the need to puncture through the abdominal wall and minimises the risk of bleeding from a cirrhotic liver with abnormal clotting.
How Does TIPS Reduce Portal Pressure?
This is the most important concept in the article. Understanding the physiology explains both why TIPS works and why it causes its main complication.
↓ must pass through
Scarred cirrhotic liver
↓ high resistance
Pressure builds upstream
↓
Portal hypertension
↓ diverts through
Low-resistance stent
↓ resistance falls
Pressure falls upstream
↓
Portal pressure reduced
The key principle is resistance. In cirrhosis, the liver offers high resistance to portal blood flow. TIPS creates a parallel, low-resistance pathway. Blood follows the path of least resistance — flowing preferentially through the stent and bypassing the high-resistance liver. Upstream portal pressure falls as a direct consequence.
TIPS is like opening a bypass road around a traffic jam. The blocked road (cirrhotic liver) remains congested, but traffic (portal blood) can now flow freely via the bypass (stent). The pressure in the congested section falls because traffic is being diverted away.
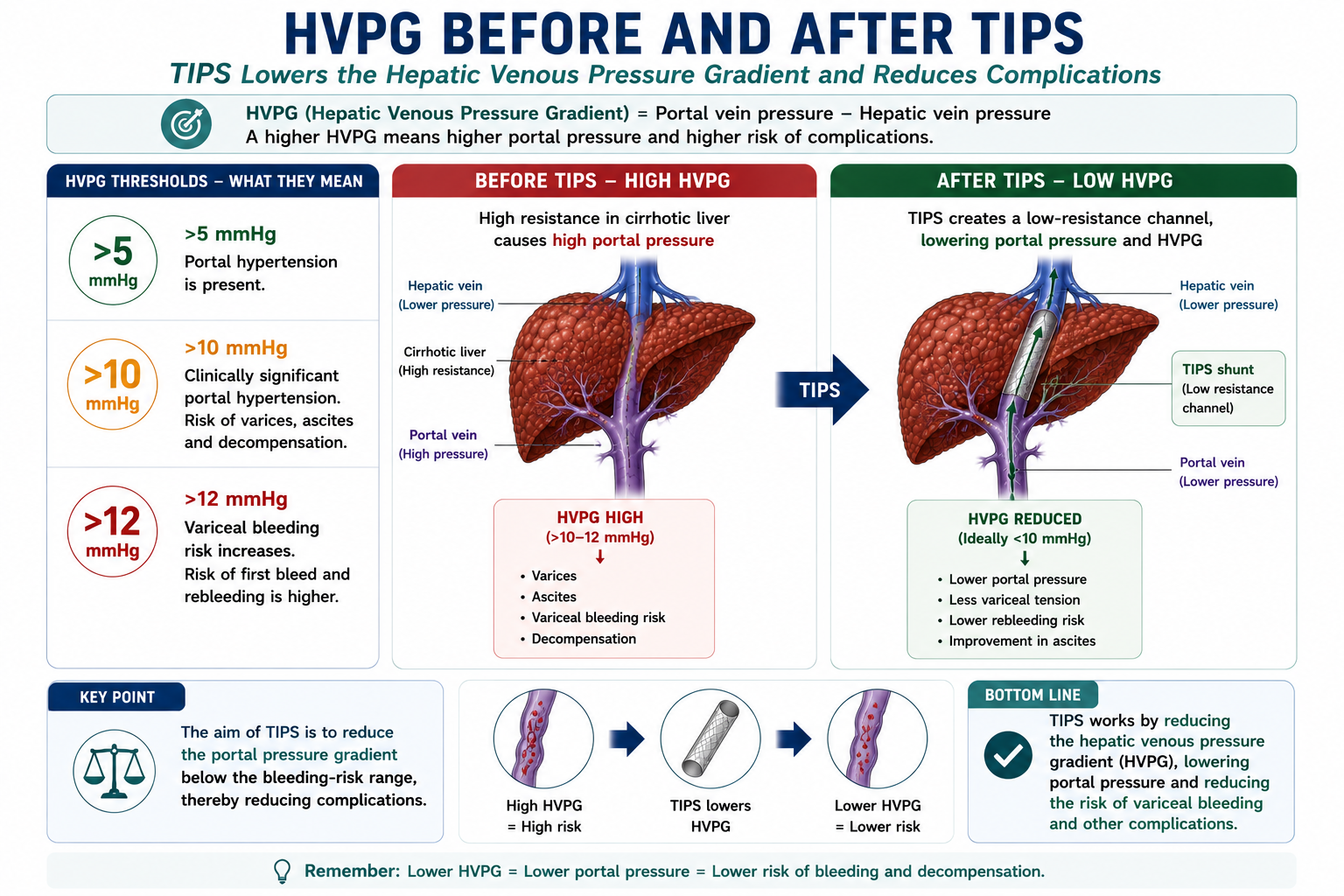
HVPG Before and After TIPS
The hepatic venous pressure gradient, or HVPG, is a specialist measurement used to estimate the pressure difference between the portal venous system and the hepatic venous system.
For students, the exact measurement technique is less important than the thresholds.
| HVPG Level | Clinical Meaning |
|---|---|
| >5 mmHg | Portal hypertension is present. |
| >10 mmHg | Clinically significant portal hypertension. Varices, ascites and decompensation become more likely. |
| >12 mmHg | Variceal bleeding becomes possible. Bleeding risk rises above this threshold. |
TIPS aims to reduce portal pressure substantially by creating a low-resistance shunt between the portal vein and hepatic vein.
A key goal of TIPS is to reduce portal pressure below the bleeding-risk range. In variceal bleeding, lowering the portal pressure gradient reduces variceal wall tension and rebleeding risk.
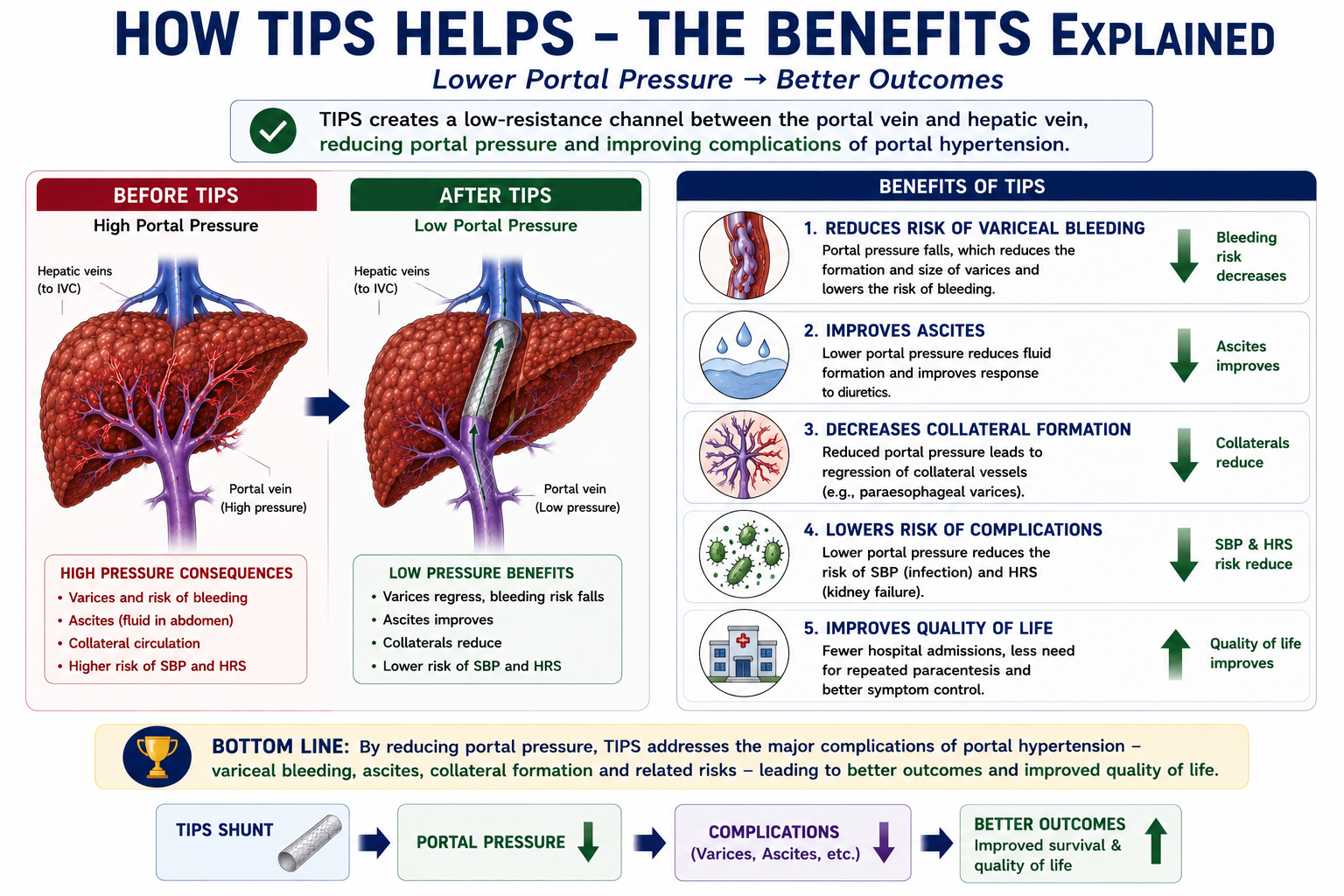
Benefits of TIPS
Because TIPS directly lowers portal pressure, it addresses the driving force behind multiple complications simultaneously.
For varices: lowering portal pressure reduces the wall tension in variceal vessels, decreasing both the risk of active bleeding and the risk of rebleeding.
For ascites: lower portal pressure reduces hydrostatic fluid transudation into the peritoneal cavity and improves effective circulating volume, blunting the RAAS activation that drives sodium and water retention.
TIPS improves both the variceal branch and the ascites branch of portal hypertension simultaneously — because both originate from the same underlying raised portal pressure. This is why TIPS is used for refractory variceal bleeding and refractory ascites.
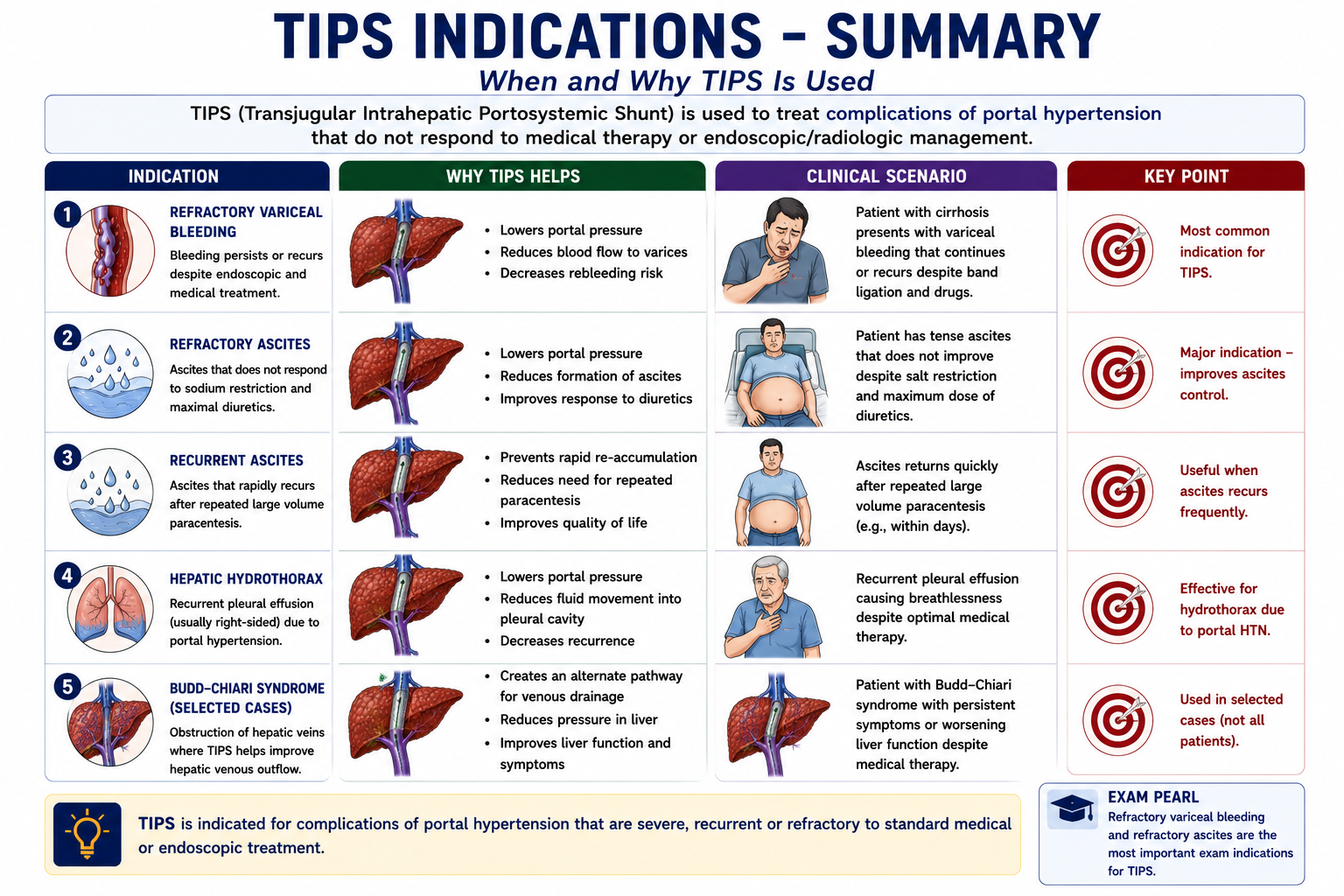
Major Indications for TIPS
TIPS is used when portal hypertension complications cannot be managed adequately with standard medical and endoscopic therapy.
| Indication | Why TIPS Helps |
|---|---|
| Refractory variceal bleeding | Lowers portal pressure, reducing variceal wall tension and bleeding risk when endoscopy and vasoactive drugs fail |
| High-risk early variceal rebleeding | Early TIPS (within 72 hours) reduces rebleeding mortality in high-risk patients (Child-Pugh C or HVPG ≥20 mmHg) |
| Refractory ascites | Reduces portal pressure and fluid transudation, decreasing ascites formation and need for repeated large-volume paracentesis |
| Recurrent symptomatic ascites | Improves portal haemodynamics long-term, reducing frequency of drainage procedures |
| Hepatic hydrothorax | Reduces ascitic fluid production, which is the source of pleural fluid in hepatic hydrothorax |
| Selected Budd-Chiari syndrome | Improves venous outflow in cases where hepatic vein obstruction causes portal hypertension |
The most commonly examined TIPS indication is refractory variceal bleeding — bleeding that cannot be controlled or that recurs early despite vasoactive drugs and endoscopic band ligation. Know that TIPS is a rescue and secondary option, not first-line therapy for a first variceal bleed.
When Should TIPS Be Avoided?
TIPS can be life-saving, but it is not suitable for every patient with portal hypertension. Because TIPS diverts portal blood away from the liver and increases venous return to the heart, patient selection is crucial.
| Contraindication / High-Risk Situation | Why It Matters |
|---|---|
| Severe or recurrent hepatic encephalopathy | TIPS may worsen encephalopathy because more portal blood bypasses liver detoxification. |
| Severe right-sided heart failure | TIPS increases venous return to the heart and can precipitate cardiac decompensation. |
| Severe pulmonary hypertension | Increased venous return can worsen pulmonary pressures and right-heart strain. |
| Very advanced liver failure | Reduced portal perfusion after TIPS can precipitate further hepatic deterioration. |
| Uncontrolled systemic infection | Infection increases procedural risk and may seed the shunt. |
| Severe uncorrectable coagulopathy | Procedure-related bleeding risk is increased. |
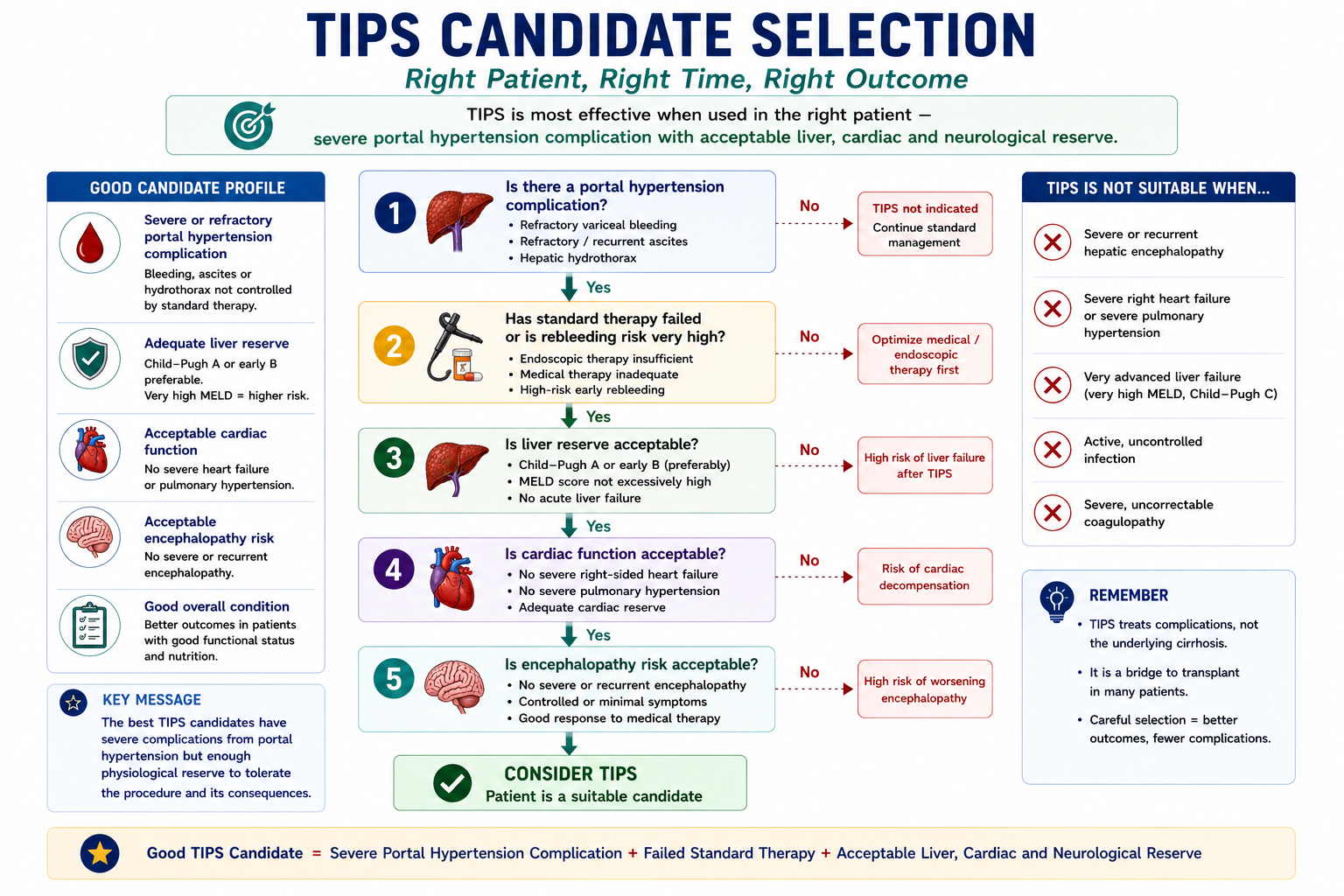
TIPS is most useful when portal hypertension complications are severe or refractory, but liver reserve, cardiac function and encephalopathy risk are still acceptable.
Who Is a Good Candidate for TIPS?
A good TIPS candidate is not simply a patient with portal hypertension. The patient should have a complication that is severe or refractory enough to justify shunt placement, while still having enough physiological reserve to tolerate the procedure.
- 1Is there a portal hypertension complication? Examples include refractory variceal bleeding, refractory ascites or hepatic hydrothorax.
- 2Has standard therapy failed or is rebleeding risk very high? TIPS is usually considered after medical, endoscopic or paracentesis-based strategies are insufficient.
- 3Is liver reserve acceptable? Very poor liver function increases the risk of post-TIPS liver failure.
- 4Is cardiac function acceptable? TIPS increases venous return and may worsen heart failure.
- 5Is encephalopathy risk acceptable? Severe or recurrent encephalopathy makes TIPS high risk.
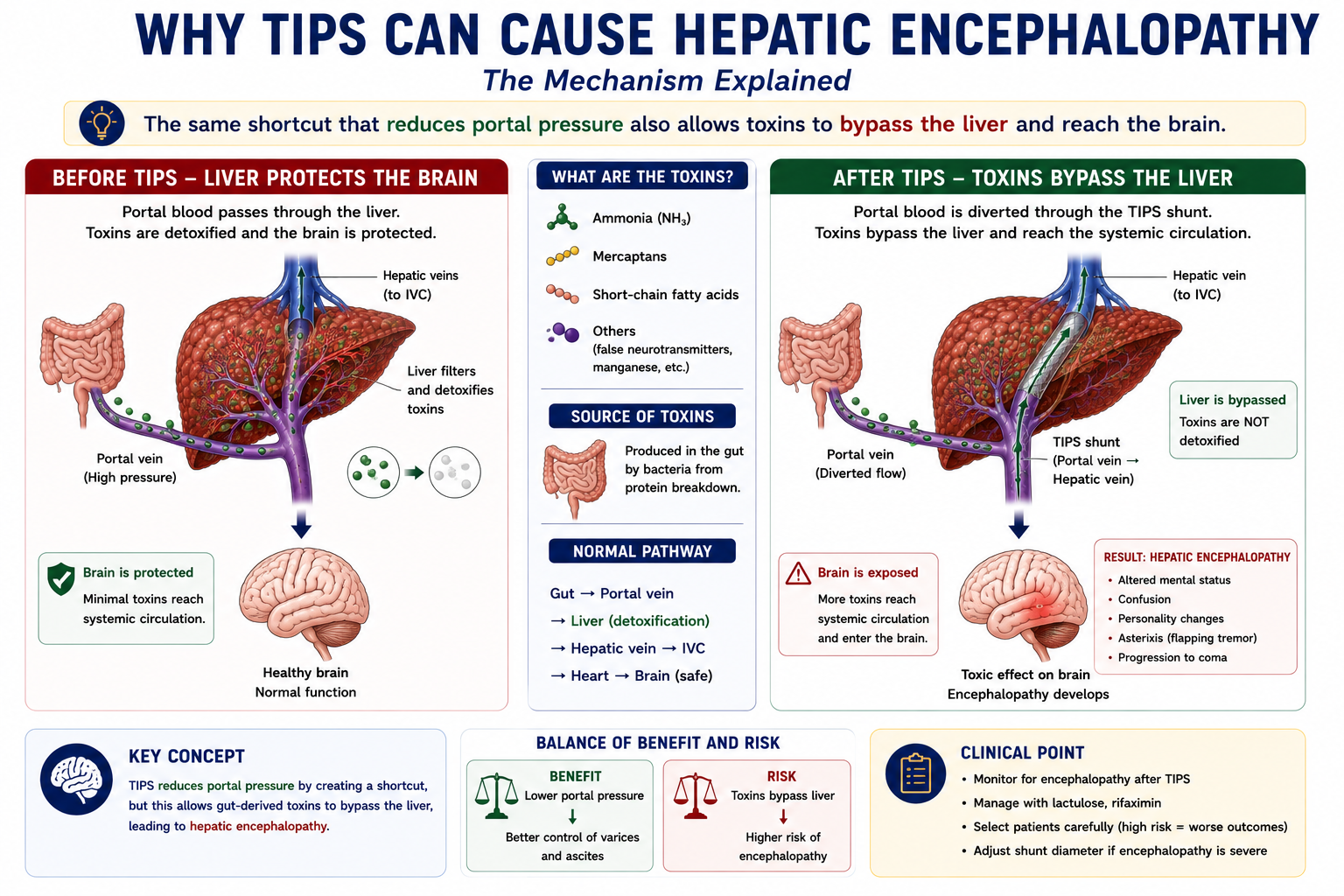
Why Can TIPS Cause Hepatic Encephalopathy?
Hepatic encephalopathy is the most important complication of TIPS. Understanding why it occurs requires understanding what the liver normally does with portal blood.
The liver's first-pass detoxification role is critical: ammonia and other nitrogenous toxins absorbed from the gut enter the portal vein and are normally removed by hepatocytes before reaching the systemic circulation. In cirrhosis, this function is already impaired — but most portal blood still passes through at least some functioning liver tissue.
↓ absorbed into portal vein
Pass through liver
↓ partially detoxified
Reduced toxin load
↓ reaches brain
Some protection maintained
↓ absorbed into portal vein
Bypass liver via stent
↓ no detoxification
Higher toxin load
↓ reaches brain
Encephalopathy risk ↑
The same mechanism that makes TIPS effective also causes its main complication. By bypassing the liver, TIPS reduces portal pressure — but at the cost of reduced hepatic detoxification. More ammonia and other neurotoxins reach the systemic circulation and the brain.
Who Is at Highest Risk?
Not all patients develop hepatic encephalopathy after TIPS. Risk is highest in:
- Patients with pre-existing hepatic encephalopathy
- Patients with advanced liver disease (high MELD score, Child-Pugh C)
- Elderly patients
- Patients with sarcopenia — reduced muscle mass impairs peripheral ammonia detoxification
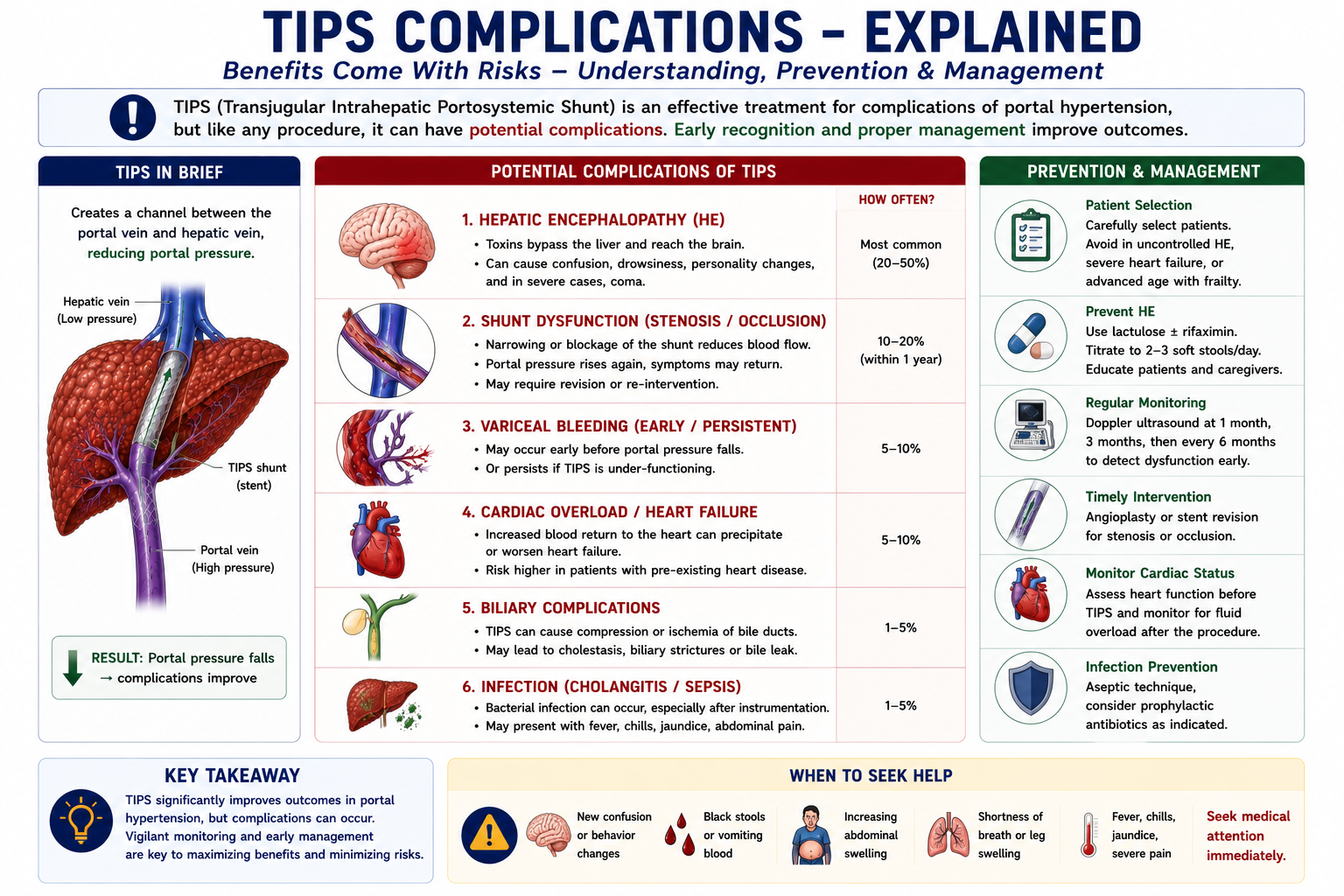
Complications of TIPS
| Complication | Mechanism | Notes |
|---|---|---|
| Hepatic encephalopathy | Toxins bypass hepatic detoxification via the shunt | Most common long-term complication; 30–40% of patients |
| Shunt stenosis | Gradual narrowing of the stent over time | Covered stents (PTFE) have lower stenosis rates than bare metal |
| Shunt occlusion | Complete stent blockage | Portal pressure rises again; complications recur |
| Heart failure worsening | Increased venous return to the right heart via the shunt | TIPS is relatively contraindicated in severe heart failure |
| Liver failure | Reduced hepatic arterial and portal perfusion | Risk highest in patients with very poor liver reserve |
| Haemobilia / haemoperitoneum | Accidental puncture of hepatic artery or capsule | Procedural complication; uncommon with modern technique |
Hepatic encephalopathy is the most common and clinically significant long-term complication of TIPS. It occurs in up to 30–40% of patients to some degree. Patients with pre-existing encephalopathy, poor liver reserve, or elderly patients are at highest risk. This is why careful patient selection is essential before TIPS placement.
Follow-Up After TIPS
TIPS is not a "place and forget" procedure. After insertion, patients require monitoring for shunt patency, recurrence of portal hypertension complications, hepatic encephalopathy and liver function deterioration.
| Follow-Up Area | What to Monitor |
|---|---|
| Shunt patency | Doppler ultrasound is used to assess shunt flow and detect stenosis or occlusion. |
| Recurrent portal hypertension | Return of ascites or variceal bleeding may suggest shunt dysfunction. |
| Hepatic encephalopathy | Monitor for sleep disturbance, confusion, personality change, asterixis or reduced consciousness. |
| Liver function | Check bilirubin, INR, albumin and clinical signs of hepatic deterioration. |
| Cardiac status | Monitor for fluid overload, dyspnoea or worsening heart failure in susceptible patients. |
Doppler ultrasound is useful after TIPS because it can assess blood flow through the shunt. Reduced flow, abnormal velocities or recurrent symptoms may suggest shunt stenosis or occlusion.
TIPS vs Paracentesis for Ascites
Both TIPS and large-volume paracentesis (LVP) are used for refractory ascites, but they work in fundamentally different ways and have different risk profiles.
| Feature | TIPS | Large-Volume Paracentesis |
|---|---|---|
| Mechanism | Treats portal pressure — reduces fluid formation | Directly removes accumulated fluid |
| Treats the cause | Yes — reduces portal hypertension | No — removes fluid but pressure unchanged |
| Duration of effect | Sustained portal pressure reduction | Temporary — ascites re-accumulates |
| Encephalopathy risk | Increased — portal blood bypasses liver | Not increased |
| Procedural risk | Higher — invasive radiological procedure | Lower — bedside needle drainage |
| Patient selection | Requires adequate liver reserve; contraindicated in encephalopathy | Can be used in most patients with ascites |
The key distinction: paracentesis removes fluid; TIPS reduces fluid formation. TIPS is preferred when repeated paracentesis is burdensome and the patient has adequate liver reserve. Paracentesis remains the safer option for patients with high encephalopathy risk or poor liver function.
TIPS vs Liver Transplantation
TIPS and liver transplantation are often discussed together because both manage advanced cirrhosis — but they are fundamentally different interventions with different goals.
| Feature | TIPS | Liver Transplantation |
|---|---|---|
| Treats portal hypertension | Yes — directly reduces portal pressure | Yes — removes the diseased liver entirely |
| Cures cirrhosis | No | Yes |
| Restores liver function | No | Yes |
| Definitive treatment | No — bridge procedure only | Yes — definitive cure |
| Encephalopathy impact | Increases encephalopathy risk | Resolves encephalopathy (new liver detoxifies) |
| Role in clinical practice | Complication control while awaiting transplant or when transplant not possible | Definitive treatment for end-stage liver disease |
TIPS is a bridge. Liver transplantation is definitive treatment. In practice, TIPS is frequently used to control complications — variceal bleeding, refractory ascites — while patients wait on the transplant list. It buys time without prejudicing transplant eligibility. Once transplanted, the TIPS is no longer relevant — the new liver resolves portal hypertension from the source.
TIPS as a Bridge to Transplant
In suitable patients with advanced cirrhosis, TIPS can stabilise complications while transplant assessment or waiting-list placement is ongoing.
This is why TIPS is often described as a bridge: it buys time by controlling complications, but the definitive treatment for end-stage cirrhosis remains liver transplantation.
One-Minute TIPS Revision
High-Yield Exam Pearls
TIPS = portal vein → hepatic vein stent
Mechanism = bypasses high-resistance cirrhotic liver
Effect = portal pressure falls
Benefits = varices improve, ascites improves
Main complication = hepatic encephalopathy
Why encephalopathy = portal blood bypasses liver detoxification
Does NOT cure cirrhosis
Bridge to liver transplantation
- TIPS is a portosystemic shunt — it connects portal and systemic circulations, reducing portal pressure by providing a low-resistance bypass pathway.
- The access route is transjugular — via the internal jugular vein, then through the hepatic vein, then needle into the portal vein.
- Most common indication — refractory variceal bleeding (and refractory ascites).
- Most common long-term complication — hepatic encephalopathy. Know the mechanism: portal blood bypasses hepatic detoxification.
- TIPS vs paracentesis — TIPS reduces fluid formation; paracentesis removes accumulated fluid. TIPS treats the cause; paracentesis treats the effect.
- TIPS vs transplant — TIPS is a bridge; transplant is the cure. TIPS does not restore liver function.
- Shunt stenosis — the most common cause of TIPS failure. Covered stents (PTFE) have better long-term patency than bare metal stents.
- Contraindications to TIPS — severe hepatic encephalopathy, severe right heart failure, very poor liver reserve (high MELD), active infection.
- HVPG thresholds — >5 mmHg = portal hypertension, >10 mmHg = clinically significant portal hypertension, >12 mmHg = variceal bleeding risk.
- Good candidate principle — refractory portal hypertension complication plus acceptable liver, cardiac and encephalopathy risk profile.
- Post-TIPS monitoring — Doppler ultrasound checks shunt patency; recurrent ascites or bleeding suggests shunt dysfunction.
- Why not everyone gets TIPS — the pressure benefit comes at the cost of encephalopathy, cardiac strain and possible liver failure.
Key Takeaways
- TIPS stands for Transjugular Intrahepatic Portosystemic Shunt — an artificial stent channel between the portal vein and hepatic vein
- The purpose of TIPS is to reduce portal pressure by bypassing the high-resistance cirrhotic liver
- Portal blood diverts through the stent into the hepatic vein, reducing upstream portal pressure
- HVPG above 10 mmHg indicates clinically significant portal hypertension; above about 12 mmHg increases variceal bleeding risk
- TIPS reduces HVPG by creating a low-resistance channel between the portal vein and hepatic vein
- TIPS should be avoided or used cautiously in severe encephalopathy, severe heart failure, severe pulmonary hypertension, active infection and very advanced liver failure
- After TIPS, patients need Doppler ultrasound and clinical monitoring for shunt dysfunction, encephalopathy and liver function deterioration
- Good TIPS candidates have severe portal hypertension complications but acceptable liver, cardiac and neurological reserve
- Benefits include reduced variceal bleeding risk and improvement of ascites — both driven by lower portal pressure
- Major indications: refractory variceal bleeding, high-risk early rebleeding, refractory ascites, hepatic hydrothorax
- Most important complication: hepatic encephalopathy — portal blood bypasses liver detoxification, raising systemic ammonia
- The mechanism that makes TIPS effective is the same mechanism that causes its main complication
- TIPS vs paracentesis: TIPS reduces fluid formation; paracentesis removes fluid — TIPS treats the cause, not the effect
- TIPS does not cure cirrhosis — it is a bridge procedure, most often used while awaiting liver transplantation
- Shunt stenosis is the most common cause of TIPS failure; covered stents reduce long-term stenosis rates
Frequently Asked Questions
References
- Rössle M. TIPS: 25 years later. J Hepatol. 2013;59(5):1081–1093.
- Boyer TD, Haskal ZJ; American Association for the Study of Liver Diseases. The Role of Transjugular Intrahepatic Portosystemic Shunt in the Management of Portal Hypertension. Hepatology. 2010;51(1):1–16.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460.
- de Franchis R; Baveno VII Faculty. Baveno VII — Renewing consensus in portal hypertension. J Hepatol. 2022;76(4):959–974.
- García-Pagán JC, Caca K, Bureau C, et al. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med. 2010;362(25):2370–2379.
- Tripathi D, Stanley AJ, Hayes PC, et al. UK guidelines on the management of variceal haemorrhage in cirrhotic patients. Gut. 2015;64(11):1680–1704.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist hepatological and interventional radiology input when managing patients with portal hypertension complications.
- What Is TIPS?
- Why Is TIPS Needed?
- How Does TIPS Work?
- How TIPS Reduces Portal Pressure
- HVPG Before and After TIPS
- Benefits of TIPS
- Indications for TIPS
- When TIPS Should Be Avoided
- Candidate Selection
- Why TIPS Causes Encephalopathy
- Complications of TIPS
- Follow-Up After TIPS
- TIPS vs Paracentesis
- TIPS vs Liver Transplant
- One-Minute Revision
- Exam Pearls
- Key Takeaways
- FAQ
- References