Most students know that ammonia causes hepatic encephalopathy.
Few understand why ammonia rises, why TIPS worsens it, why GI bleeding triggers it, and why lactulose works.
Hepatic encephalopathy is the neurological complication that ties together portal hypertension, variceal bleeding, SBP and TIPS into a single coherent story. Understanding hepatic encephalopathy requires understanding the liver's detoxification role — and what happens when that role fails.
Portal hypertension → ascites → SBP → HRS
Portal hypertension → varices → variceal bleeding
Portal hypertension → TIPS → hepatic encephalopathy
Cirrhosis itself → impaired detoxification → hepatic encephalopathy
Learning Objectives
- Define hepatic encephalopathy and explain why it is a brain problem caused by liver disease
- Explain the role of ammonia and how the healthy liver removes it
- Understand how portosystemic shunting contributes to HE
- Describe the West Haven classification (Grades 0–4)
- Identify common precipitating factors and explain why each triggers HE
- Explain the specific mechanisms by which GI bleeding and SBP trigger HE
- Explain why TIPS increases the risk of hepatic encephalopathy
- Understand how lactulose and rifaximin reduce ammonia and treat HE
- Distinguish minimal HE from overt HE
What Is Hepatic Encephalopathy?
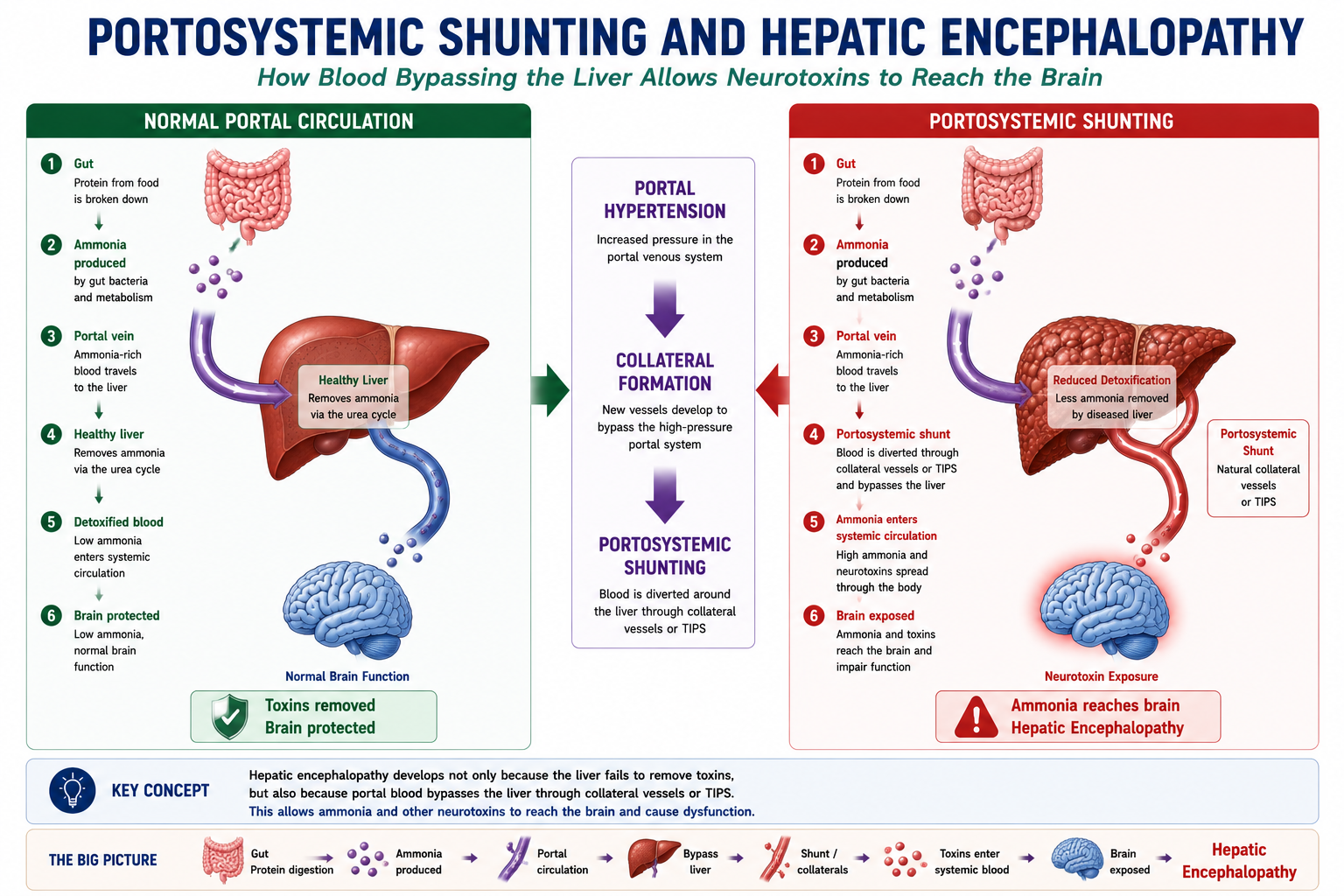
Hepatic encephalopathy (HE) is a potentially reversible neuropsychiatric syndrome caused by liver dysfunction and/or portosystemic shunting.
It occurs when the liver fails to remove neurotoxic substances — most importantly ammonia — from the circulation. These toxins accumulate and impair brain function, producing a spectrum of neurological and psychiatric disturbances.
HE is a brain problem caused by liver disease. The damaged organ is the liver; the organ that malfunctions is the brain. The bridge between the two is failure of hepatic detoxification — particularly of ammonia.
HE can occur in two settings:
- Acute liver failure — sudden severe loss of liver function (e.g. paracetamol overdose, acute viral hepatitis)
- Cirrhosis and chronic liver disease — either episodic (triggered by a precipitant) or persistent (ongoing impairment in advanced disease)
This article focuses primarily on HE in cirrhosis, which is the most commonly encountered setting in clinical practice and examinations.
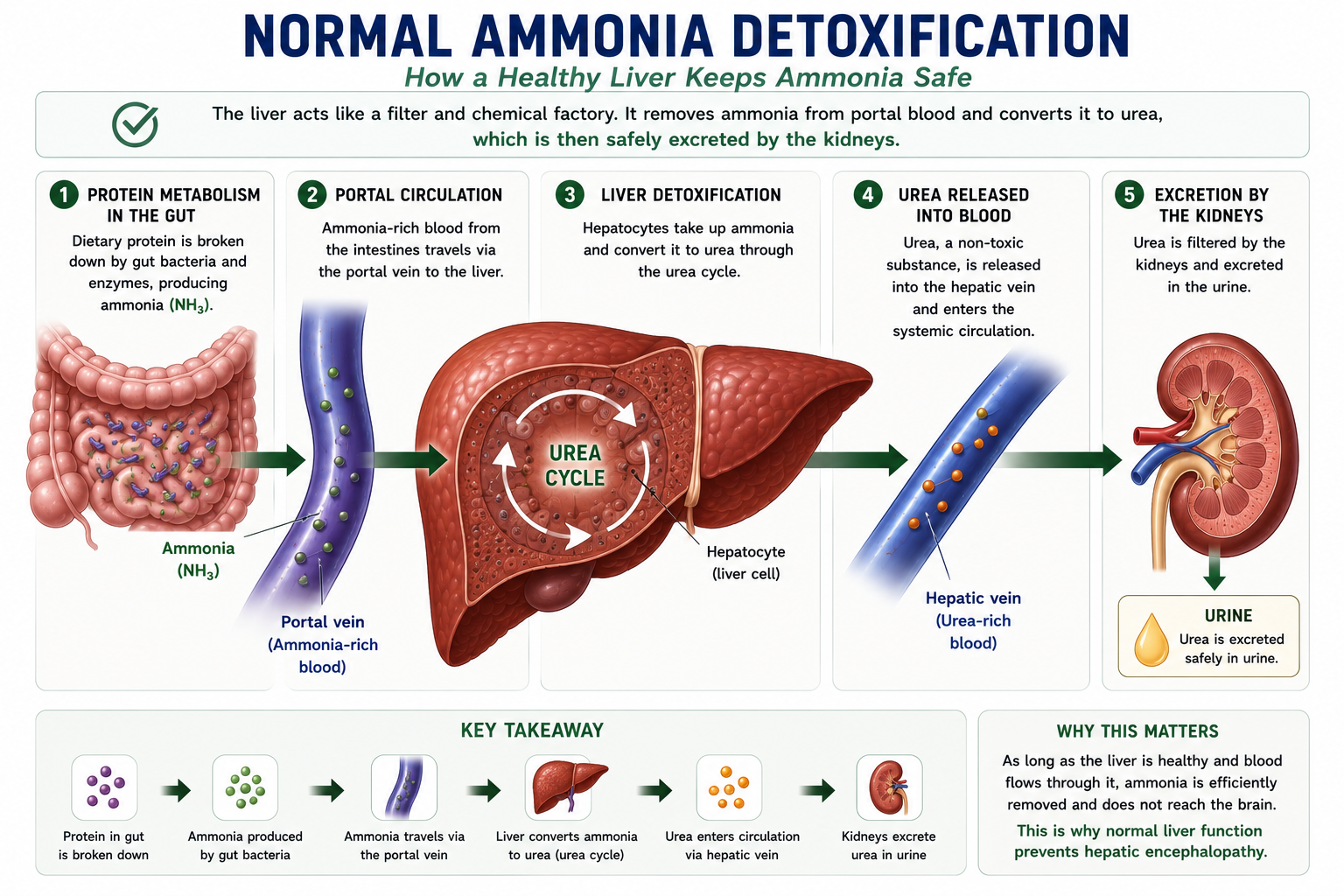
Normal Ammonia Detoxification
To understand why ammonia accumulates in liver disease, you must first understand where ammonia comes from and how the healthy body removes it.
Where Does Ammonia Come From?
Ammonia is produced continuously in the gut by two main mechanisms:
- Bacterial metabolism — colonic bacteria break down undigested proteins and urea, releasing ammonia as a byproduct
- Amino acid deamination — dietary protein digestion releases ammonia during amino acid breakdown in the gut and elsewhere
How Is It Normally Removed?
Ammonia absorbed from the gut enters the portal vein and travels directly to the liver. In the healthy liver, hepatocytes convert ammonia to urea via the urea cycle. Urea is then excreted in the urine. This first-pass hepatic detoxification is highly efficient — almost all ammonia is removed before it can reach the systemic circulation and the brain.
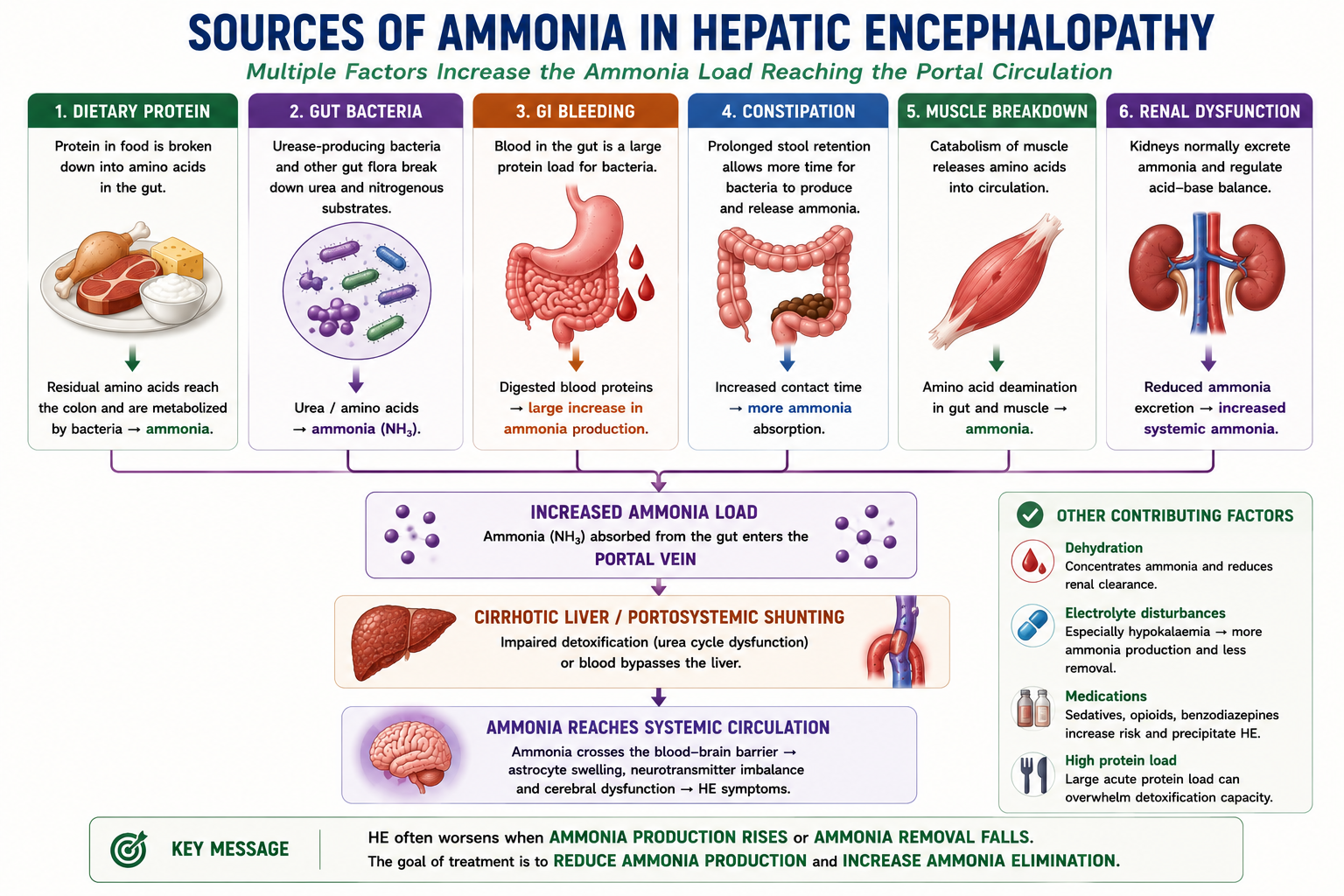
Where Does Ammonia Come From?
Ammonia is not produced only from dietary protein. Several sources contribute to the ammonia load reaching the portal circulation.
| Source | How It Increases Ammonia |
|---|---|
| Dietary protein | Protein digestion produces amino acids; bacterial metabolism generates ammonia. |
| Gut bacteria | Urease-producing bacteria break down urea and nitrogenous substrates into ammonia. |
| GI bleeding | Blood in the gut acts as a large protein load and sharply increases ammonia production. |
| Constipation | Prolonged stool retention gives bacteria more time to produce and release ammonia. |
| Muscle breakdown | Catabolism increases nitrogen load and ammonia generation. |
| Renal dysfunction | Reduced ammonia excretion contributes to systemic accumulation. |
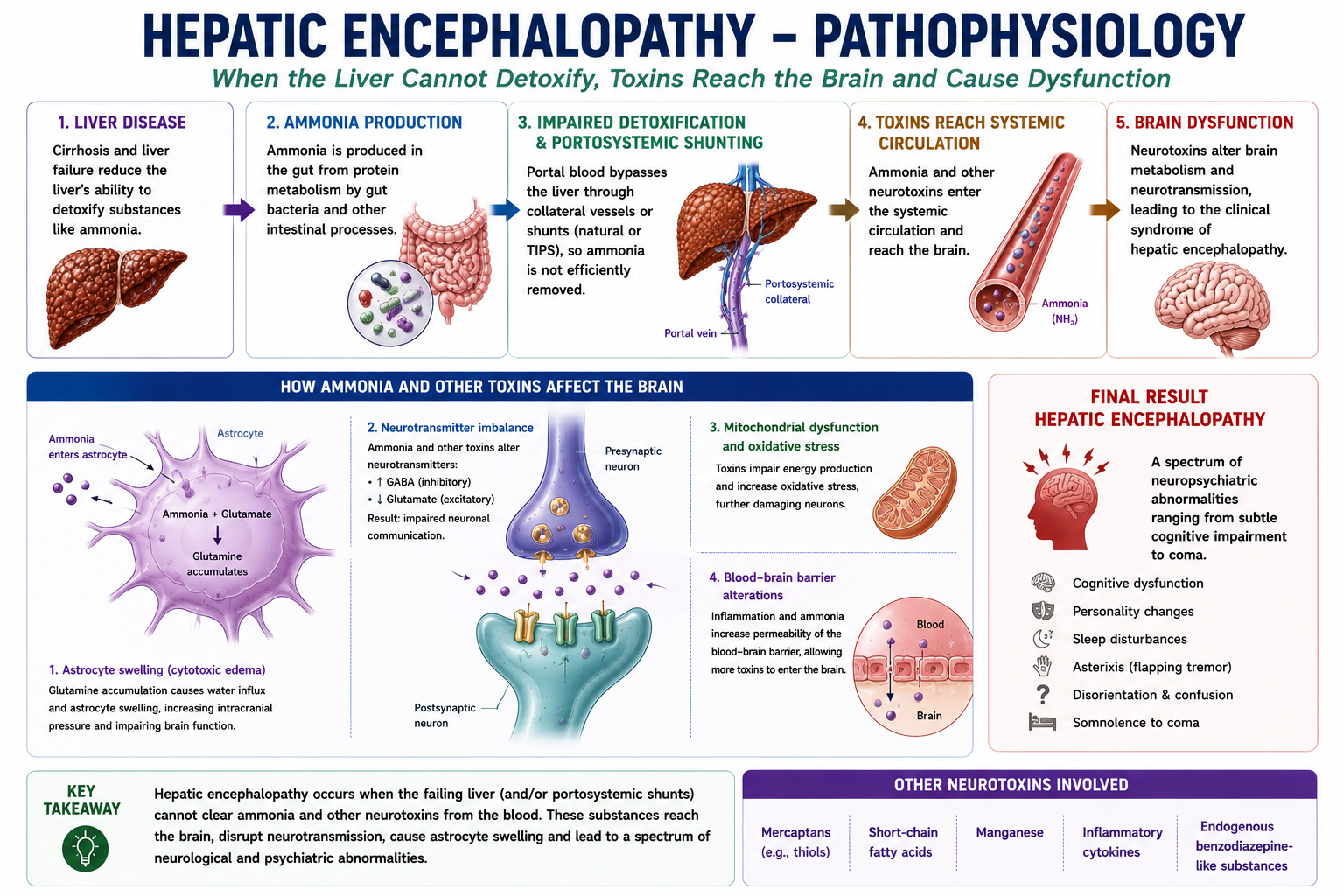
Pathophysiology of Hepatic Encephalopathy
In cirrhosis, two processes combine to allow ammonia and other toxins to reach the brain in dangerous concentrations.
| Problem | Mechanism | Effect |
|---|---|---|
| Impaired hepatic detoxification | Cirrhotic hepatocytes have reduced urea cycle capacity | Less ammonia converted to urea — blood ammonia rises |
| Portosystemic shunting | Collateral vessels and TIPS bypass the liver | Portal blood (containing ammonia) reaches systemic circulation without detoxification |
Once in the systemic circulation, ammonia crosses the blood-brain barrier. Within the brain, astrocytes — the cells responsible for much of the brain's own ammonia detoxification via glutamine synthesis — swell in response to the ammonia load. This astrocyte swelling is thought to be a central mechanism causing cerebral oedema and brain dysfunction in HE.
Ammonia is the most important neurotoxin in HE, but not the only one. Inflammatory cytokines, mercaptans, short-chain fatty acids and GABA-receptor modulating substances also contribute. This explains why ammonia levels do not always correlate perfectly with clinical HE severity — multiple toxins are involved.
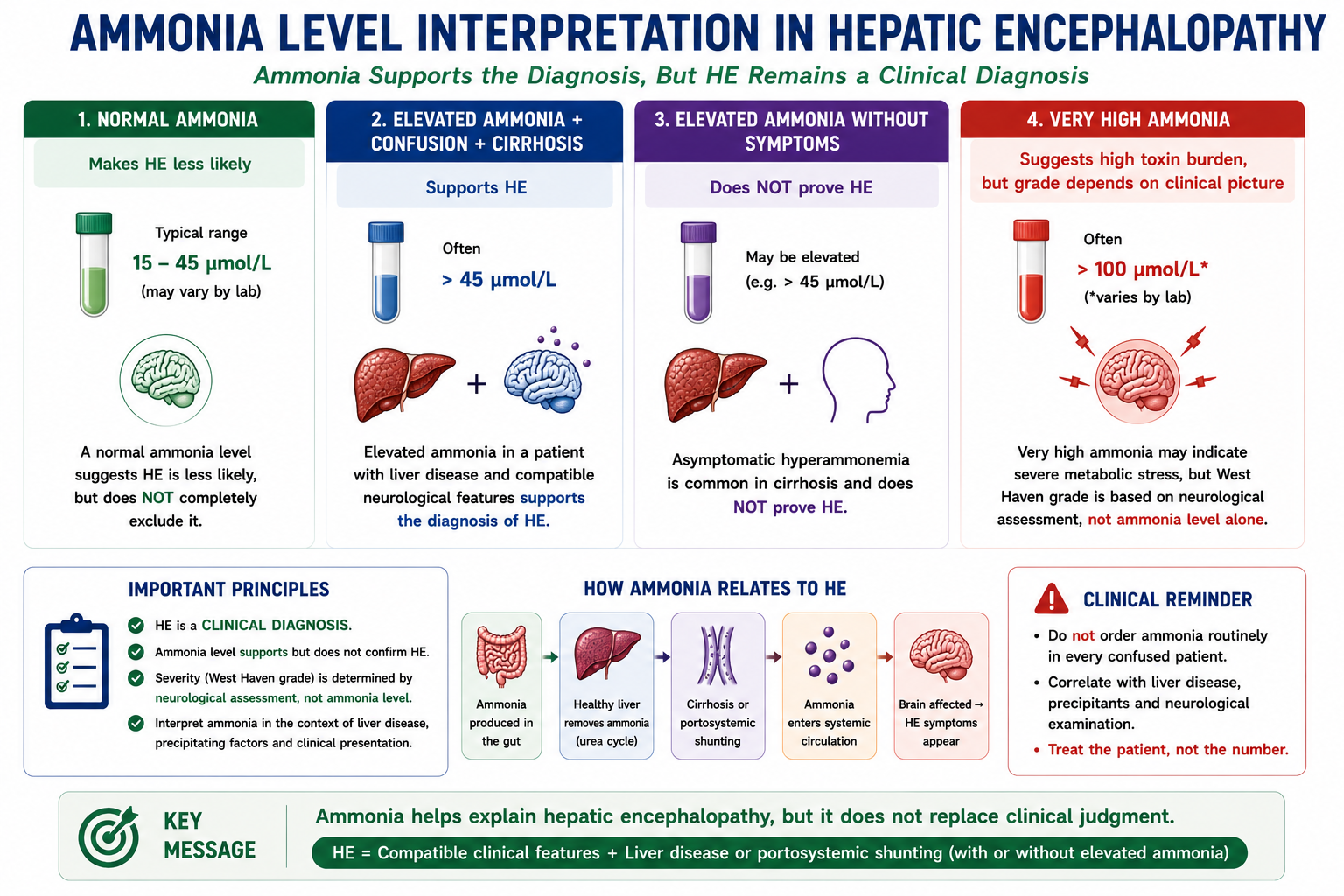
Ammonia Levels in Hepatic Encephalopathy
Ammonia is central to the pathophysiology of hepatic encephalopathy, but ammonia level alone does not diagnose HE.
HE is a clinical diagnosis. Ammonia measurement can support the diagnosis, but it must be interpreted in the clinical context.
| Ammonia Result | Interpretation |
|---|---|
| Normal ammonia | Makes hepatic encephalopathy less likely, but does not fully exclude it. |
| Elevated ammonia with confusion | Supports HE if the patient has liver disease or portosystemic shunting. |
| Elevated ammonia without symptoms | Does not prove HE. Some patients with cirrhosis have elevated ammonia without obvious encephalopathy. |
| Very high ammonia | May suggest severe toxin burden, but clinical grade still depends on neurological assessment. |
Do not diagnose hepatic encephalopathy from ammonia alone. The diagnosis requires compatible clinical features in a patient with liver disease or portosystemic shunting.
Role of Portosystemic Shunting
Portosystemic shunting is the second critical mechanism in HE and explains several important clinical scenarios — including why TIPS dramatically increases encephalopathy risk.
In portal hypertension, elevated portal pressure opens alternative venous channels (portosystemic collaterals) that allow portal blood to reach the systemic circulation without passing through the liver. The most important sites are the distal esophagus, stomach, rectum and umbilicus — but any portosystemic collateral contributes to this bypass.
Route 1 — Impaired detoxification: Portal blood enters the liver but hepatocytes cannot adequately convert ammonia to urea.
Route 2 — Shunting: Portal blood bypasses the liver entirely via collaterals or TIPS, delivering undetoxified ammonia directly to the systemic circulation.
This is why HE worsens in several clinical scenarios: when TIPS is placed (creating a deliberate large portosystemic shunt), when portal hypertension worsens (opening more collaterals), or when liver function deteriorates further (reducing residual detoxification capacity).
Clinical Features
Hepatic encephalopathy produces a spectrum of neuropsychiatric disturbances that reflect the degree of toxic impairment of brain function. Symptoms tend to fluctuate and are often worse in the evening or at night.
Progression of Features
As ammonia and neurotoxin burden increases, clinical features progress:
- Subtle impairment — reduced concentration, slowed thought, minor personality change
- Sleep disturbance — reversal of sleep-wake cycle (drowsy by day, wakeful at night)
- Confusion and disorientation — to time, then place, then person
- Lethargy and drowsiness — progressive reduction in conscious level
- Coma — no response to stimuli in severe cases
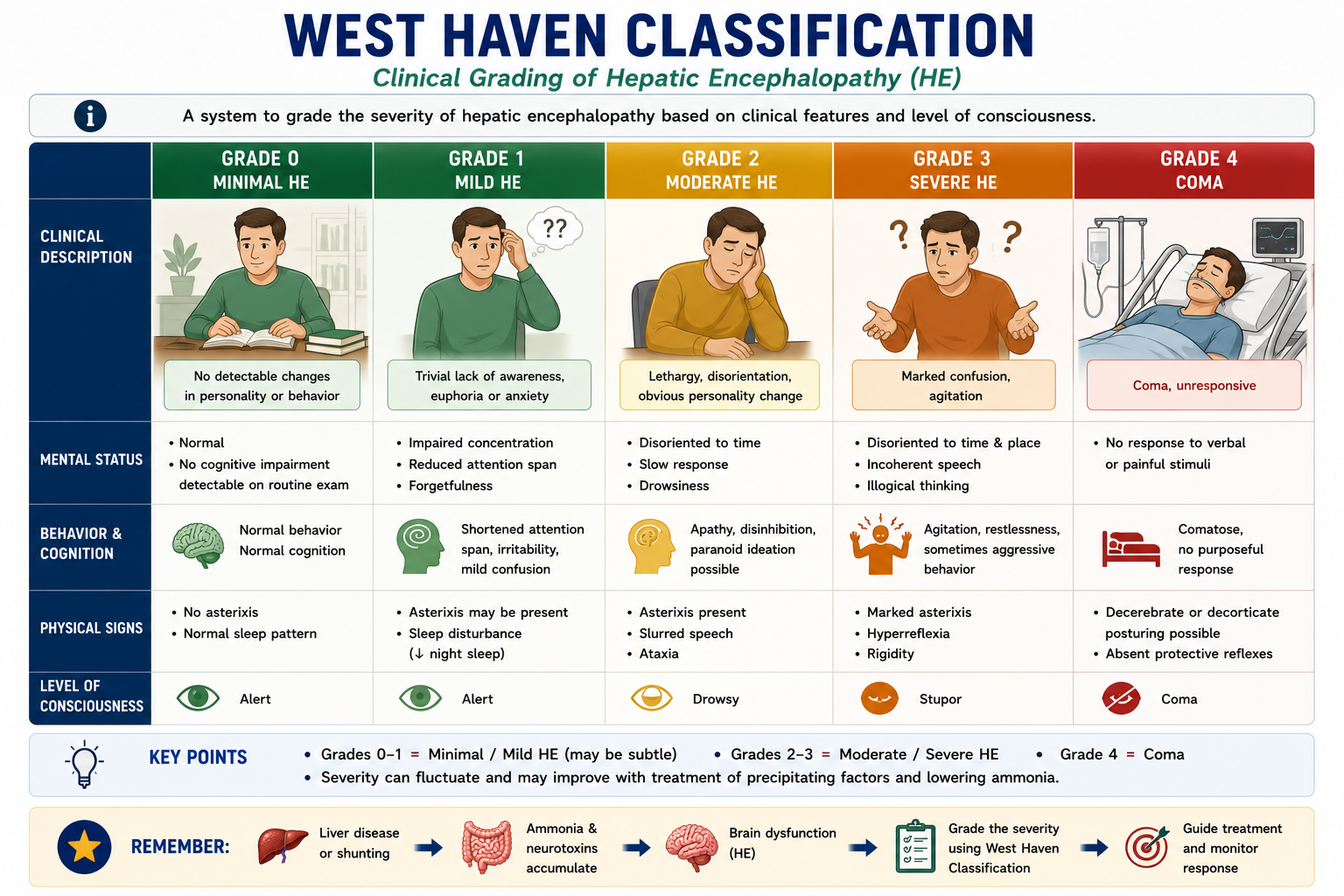
Asterixis is the characteristic physical sign of hepatic encephalopathy. It is demonstrated by asking the patient to extend their arms and dorsiflex their wrists ("stop traffic" position). Brief, intermittent lapses of sustained posture cause the wrists to momentarily flap downward before returning to position. This "flapping tremor" reflects failure of sustained motor control caused by ammonia and neurotoxin impairment of the thalamic reticular system. Asterixis is typically present in Grade 2 HE. It is not specific to HE — it also occurs in uraemia, hypercapnia and other metabolic encephalopathies.
West Haven Classification
The West Haven criteria grade hepatic encephalopathy from 0 to 4 based on neuropsychiatric features. This grading system is the most widely used in clinical practice and examinations.
Grades 1–2 are sometimes called overt HE (clinically apparent); Grade 0 is minimal or covert HE (detectable only on testing). Grades 3–4 represent severe HE requiring intensive management. Grade 4 = coma — this is a consistently tested fact.
Covert vs Overt Hepatic Encephalopathy
Hepatic encephalopathy is often divided into covert HE and overt HE. This distinction is useful because early HE may not be obvious during routine clinical examination.
| Feature | Covert HE | Overt HE |
|---|---|---|
| West Haven grade | Grade 0 and sometimes Grade 1 | Usually Grades 2–4 |
| Clinical visibility | Subtle or not obvious on routine examination | Clinically obvious confusion, asterixis or altered consciousness |
| Detection | Psychometric or neurophysiological testing may be needed | Clinical diagnosis |
| Functional impact | Driving impairment, reduced attention, reduced work performance | Hospital admission, falls, aspiration risk, coma risk |
| Exam clue | Normal-looking patient with impaired testing | Cirrhosis + confusion + asterixis |
Covert HE affects function even when the patient looks clinically normal. Overt HE is clinically apparent and usually needs active treatment and precipitant search.
What Triggers Hepatic Encephalopathy?
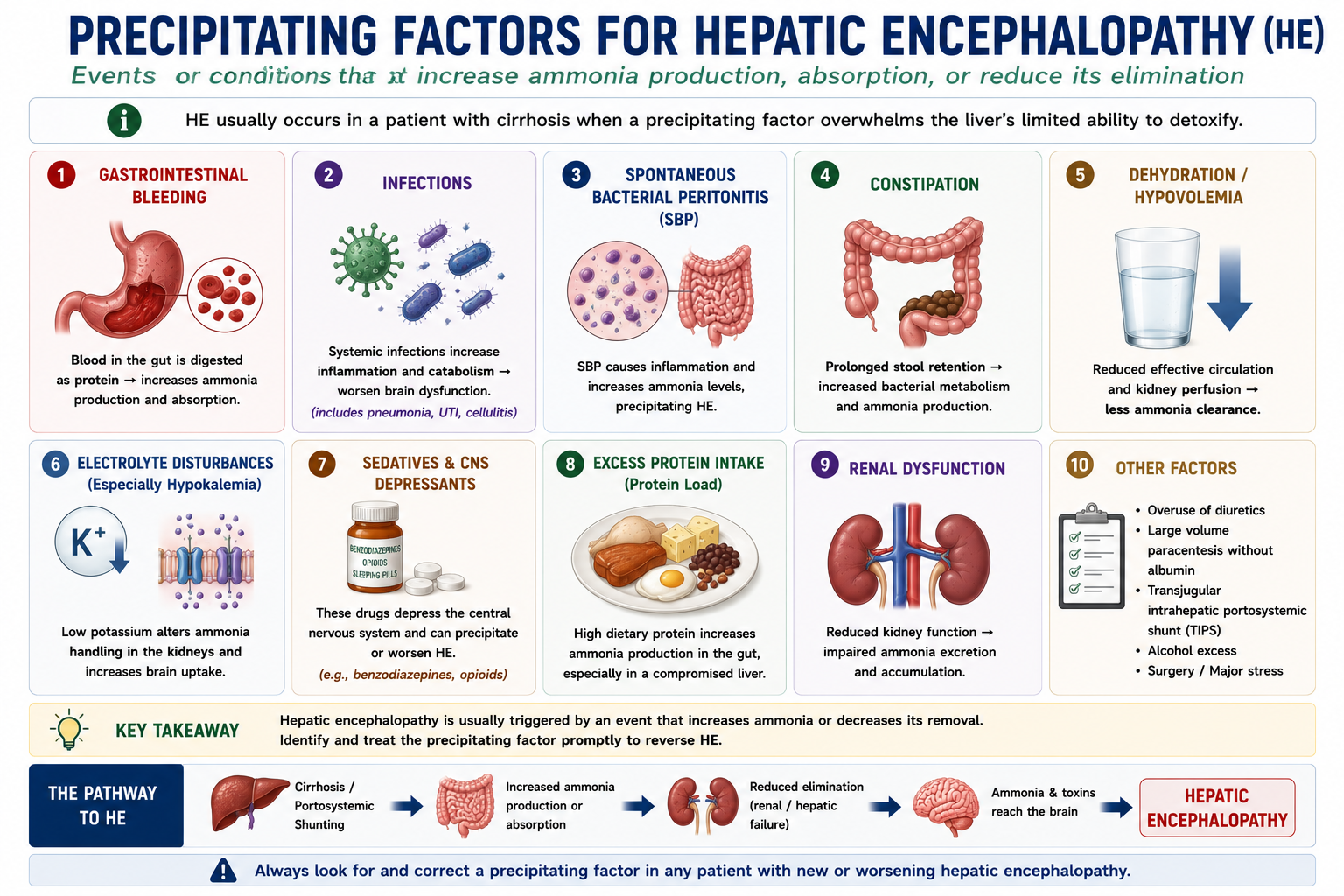
In most patients with cirrhosis, an acute episode of HE has an identifiable precipitating factor. Identifying and correcting the trigger is the cornerstone of acute management.
| Trigger | Mechanism |
|---|---|
| GI bleeding | Blood in the gut is a large protein load — bacterial digestion produces a surge of ammonia |
| Infection (including SBP) | Systemic inflammation impairs brain tolerance to ammonia and other toxins |
| Constipation | Prolonged gut transit increases ammonia absorption from the colon |
| Dehydration | Reduces renal ammonia clearance; worsens circulatory dysfunction |
| Hypokalaemia | Alters renal ammonia handling — increased renal ammoniagenesis |
| Sedatives and opioids | Direct CNS depression compounds neurotoxin-driven impairment |
| Excess protein intake | Increases substrate for ammonia production in the gut |
| TIPS placement | Creates large portosystemic shunt — portal blood bypasses liver detoxification |
| Hepatocellular carcinoma | Progressive loss of functional liver mass reduces detoxification capacity |
The most commonly examined triggers are GI bleeding, infection/SBP, constipation and TIPS. Know the mechanism for each — especially why GI bleeding and SBP precipitate HE, as these have specific mechanistic explanations.
Why Does GI Bleeding Trigger Hepatic Encephalopathy?
Gastrointestinal bleeding is one of the most important precipitants of HE in cirrhosis. Understanding the mechanism explains why certain treatments (antibiotic prophylaxis, lactulose) are given routinely in this setting.
Blood is essentially a very large protein load in the gut. When 500 mL of blood enters the gut from a variceal bleed, the nitrogen content can be equivalent to a large protein meal. Gut bacteria metabolise this protein to ammonia far faster than the cirrhotic liver can clear it.
In variceal bleeding, antibiotic prophylaxis is mandatory — not only to prevent SBP, but also because reducing gut bacterial activity decreases ammonia production from the blood protein load, reducing the risk of precipitating HE.
Why Does SBP Trigger Hepatic Encephalopathy?
Spontaneous bacterial peritonitis is one of the most important precipitants of HE, and it frequently presents with HE as the primary neurological manifestation — sometimes before fever or abdominal pain are apparent.
In a cirrhotic patient presenting with confusion, always consider SBP. HE may be the presenting feature of SBP even when fever and abdominal pain are absent. A diagnostic ascitic tap should be performed urgently in any cirrhotic patient with new or worsening HE.
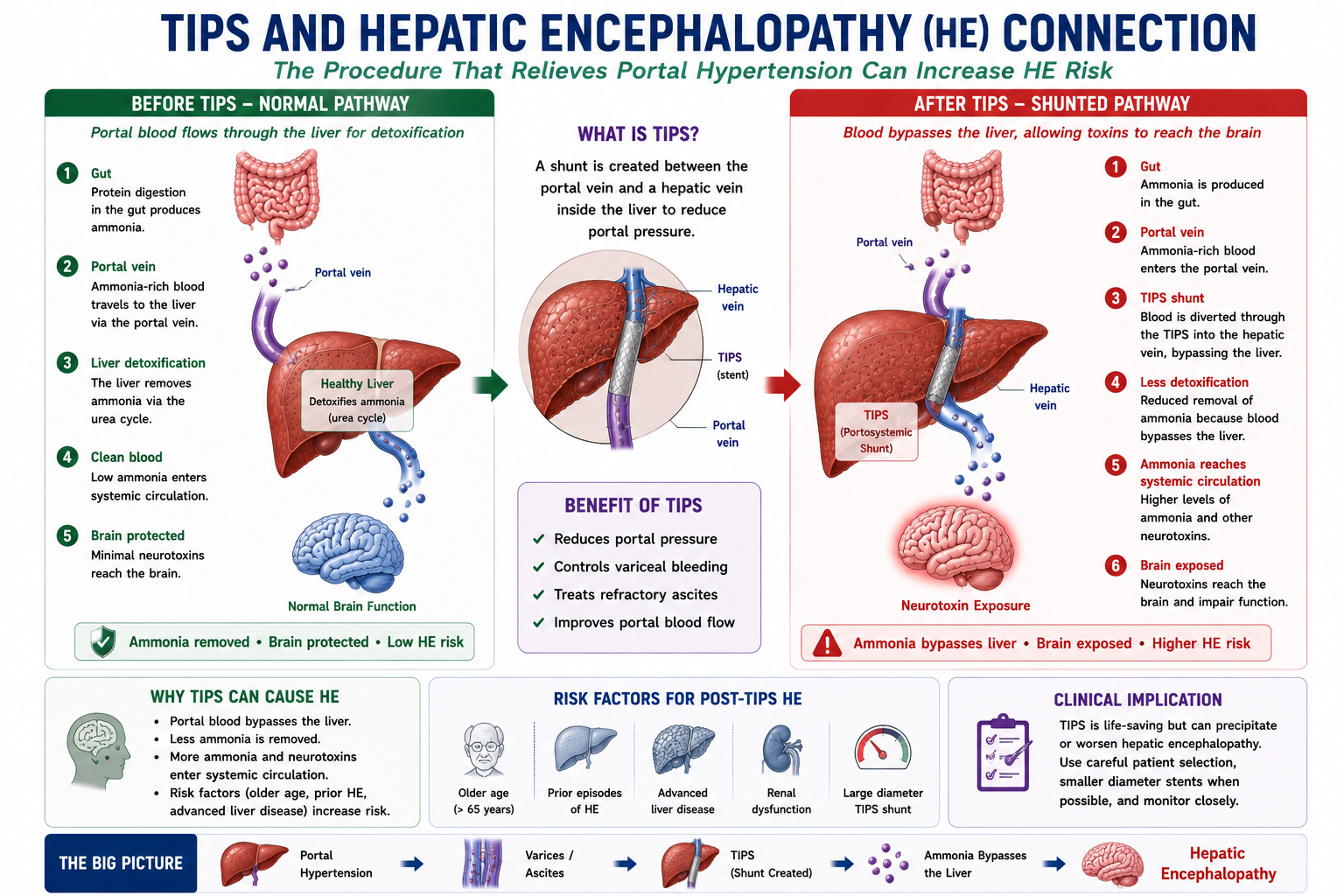
Why Does TIPS Increase Hepatic Encephalopathy Risk?
TIPS creates a deliberate, large portosystemic shunt between the portal vein and hepatic vein. This is its mechanism of benefit — and also its most important complication.
The same mechanism that makes TIPS effective also causes its most important complication. TIPS reduces portal pressure by bypassing the liver — but this reduces hepatic detoxification. It is why pre-existing hepatic encephalopathy is a relative contraindication to TIPS, and why patients are monitored closely for HE after TIPS placement.
How Is Hepatic Encephalopathy Treated?
The management of acute HE follows a four-step framework. All steps are applied simultaneously, not sequentially.
- 1Identify the precipitant. Review for GI bleeding, infection (including SBP), constipation, dehydration, hypokalaemia, sedatives, dietary excess protein. Most episodes have an identifiable trigger.
- 2Correct the precipitant. Treat infection with antibiotics, control GI bleeding, correct electrolytes, stop sedatives, relieve constipation. Correcting the trigger often resolves the HE without further treatment.
- 3Reduce ammonia. Lactulose is the first-line agent for reducing intestinal ammonia. Titrate to 2–3 soft bowel motions per day. Rifaximin is added for recurrent or refractory HE.
- 4Prevent recurrence. Ongoing lactulose and rifaximin for secondary prophylaxis. Address modifiable risk factors — optimise nutrition, avoid sedatives, monitor for new triggers.
HE is often reversible when the precipitant is identified and corrected promptly. The metabolic encephalopathy itself tends to improve as the ammonia burden falls. This reversibility distinguishes HE from structural brain disease.
Lactulose Explained
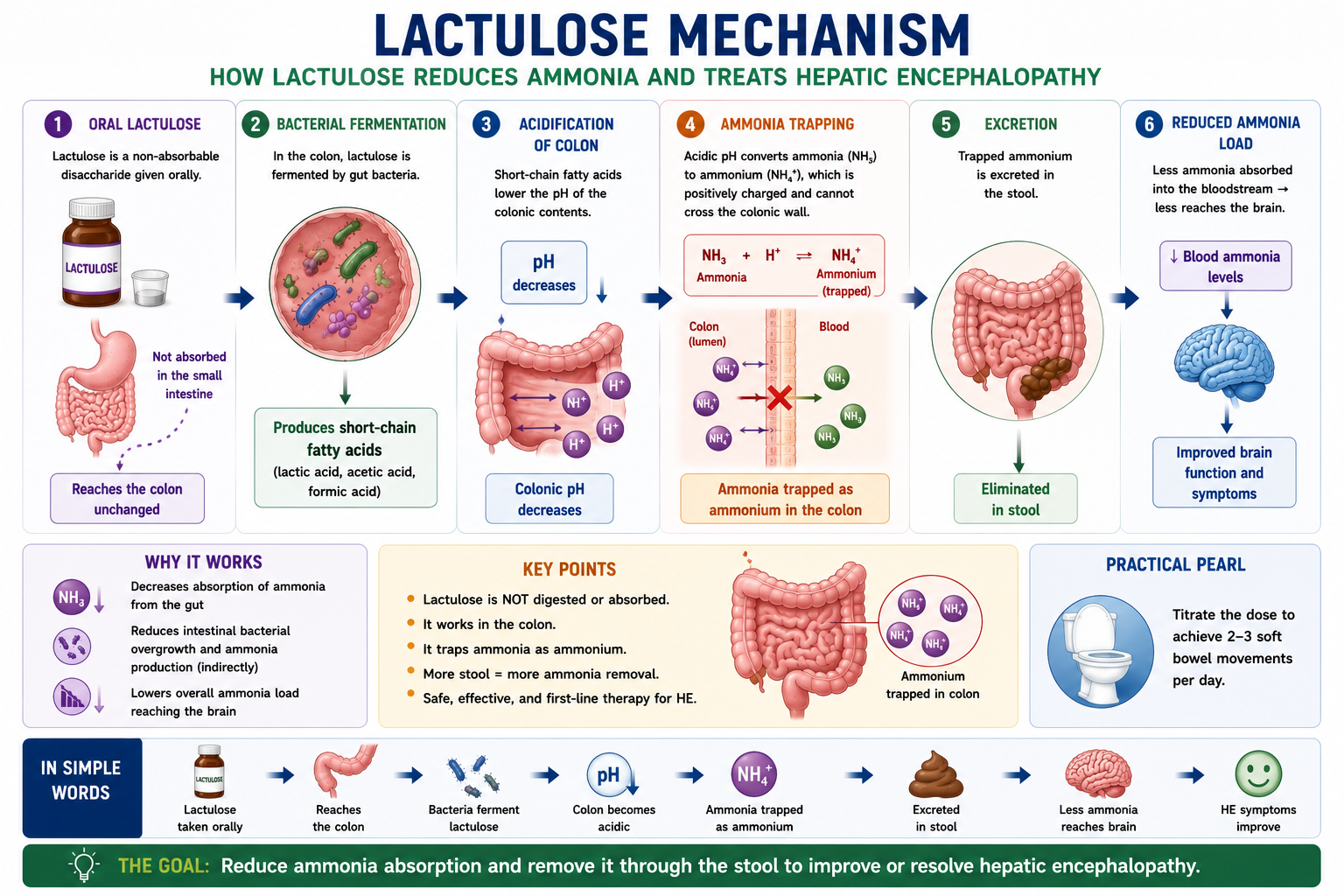
Lactulose is a non-absorbable synthetic disaccharide and the first-line treatment for hepatic encephalopathy. Its mechanism directly targets the gut source of ammonia.
How Lactulose Works
Lactulose is not absorbed in the small intestine. It reaches the colon intact, where gut bacteria metabolise it to produce lactic and acetic acids. These acids lower the colonic pH. The acidic environment converts ammonia (NH₃) — a gas that crosses the colonic wall readily — into ammonium (NH₄⁺), an ionised form that cannot be absorbed. Ammonium remains trapped in the colon and is excreted in stool.
Lactulose also acts as an osmotic laxative, drawing water into the colon and accelerating gut transit. This reduces the time available for ammonia production and absorption.
The treatment goal is 2–3 soft bowel motions per day. Under-dosing leaves too much ammonia in the gut; over-dosing causes diarrhoea, dehydration and electrolyte disturbance — which can worsen HE. Dose titration to bowel frequency is important.
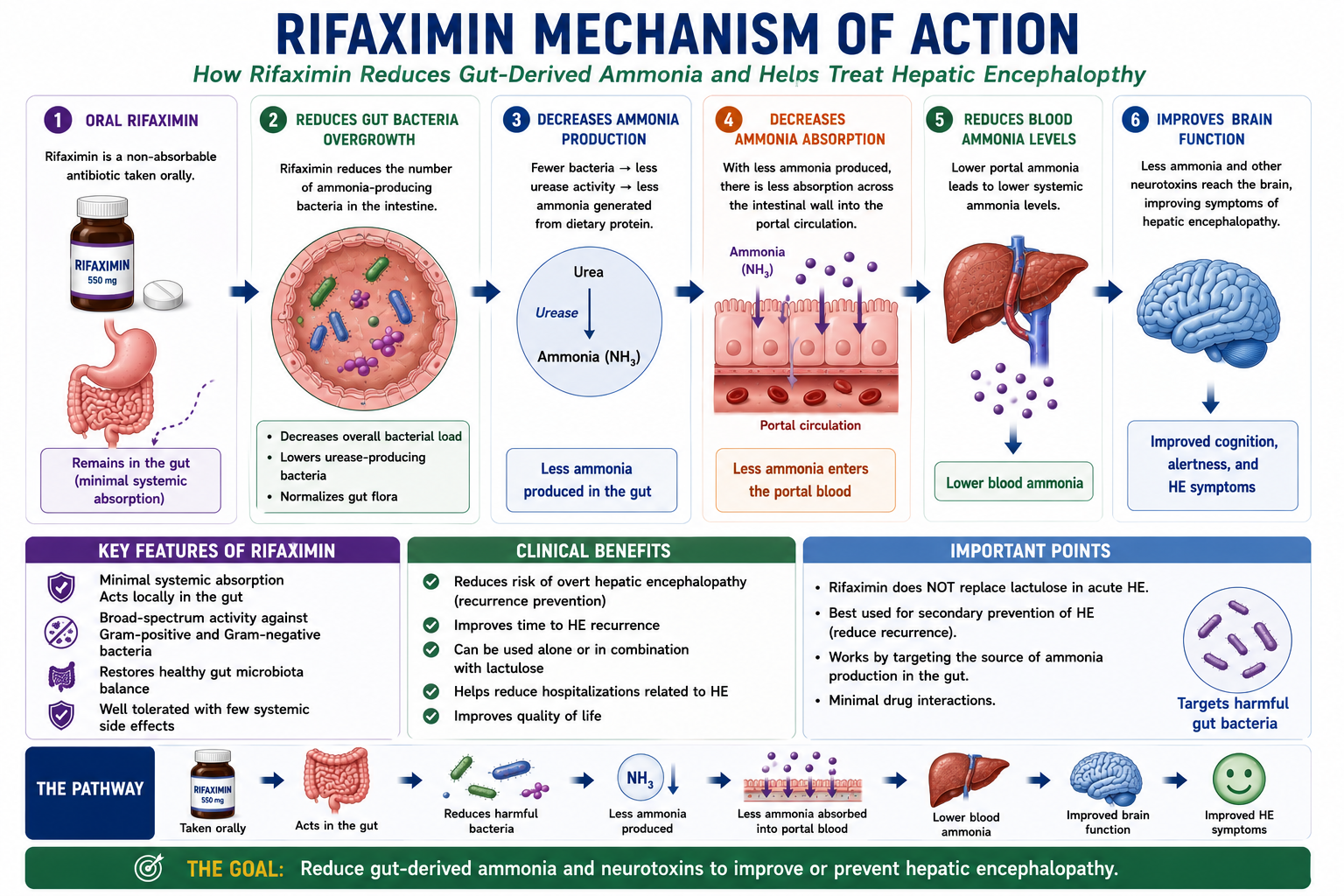
Rifaximin Explained
Rifaximin is a non-absorbable oral antibiotic that works at a different point in the ammonia pathway compared to lactulose. Rather than trapping produced ammonia, rifaximin reduces the bacterial populations responsible for producing it in the first place.
Lactulose — traps ammonia after it is produced (acidification).
Rifaximin — reduces ammonia production by targeting the bacteria that make it.
The two mechanisms are complementary. Rifaximin is primarily used for secondary prophylaxis — preventing recurrent overt HE in patients who have already had an episode — usually in combination with lactulose.
Minimal Hepatic Encephalopathy
Minimal HE (West Haven Grade 0 / covert HE) is present in up to 30–40% of patients with cirrhosis. It is not detectable on standard clinical examination but significantly impairs quality of life, cognitive function and safety.
| Feature | Details |
|---|---|
| Clinical examination | Normal — no asterixis, no confusion detectable on routine assessment |
| Psychometric tests | Abnormal — impaired attention, reaction time, visuospatial ability |
| Driving | Reduced driving performance and increased accident risk |
| Work performance | Reduced concentration and productivity |
| Quality of life | Significantly impaired despite appearing clinically normal |
| Progression risk | Predicts future overt HE episodes |
Patients with minimal HE have impaired reaction times and decision-making that compromises safe driving, even when they appear neurologically normal on examination. This is an important counselling point for patients with cirrhosis, particularly those with known prior HE episodes.
Severity, Recurrence and Prognosis
A single episode of hepatic encephalopathy may be fully reversible, especially when the precipitating factor is identified early and corrected. However, recurrent HE is clinically important because it reflects advanced liver disease and reduced physiological reserve.
Recurrent HE is associated with hospital admissions, falls, driving impairment, caregiver burden and reduced survival. It should prompt review of liver disease severity, precipitating factors, nutritional status and transplant suitability.
Hepatic encephalopathy is part of the Child-Pugh score and is a marker of decompensated cirrhosis. MELD helps quantify transplant priority using objective laboratory values, while Child-Pugh captures clinical decompensation including ascites and encephalopathy.
HE vs Delirium vs Dementia
In clinical practice, distinguishing hepatic encephalopathy from other causes of acute or chronic cognitive impairment is important — particularly in patients where the diagnosis of cirrhosis is not yet established.
| Feature | Hepatic Encephalopathy | Delirium | Dementia |
|---|---|---|---|
| Liver disease | Yes — essential for diagnosis | Variable — any systemic cause | No |
| Onset | Acute or subacute; episodic | Acute | Insidious, progressive |
| Reversibility | Often reversible with treatment | Often reversible when cause treated | Usually irreversible |
| Asterixis | Common (Grade 2) | Rare | Rare |
| Ammonia | Often elevated | Normal (unless HE is cause) | Normal |
| Fluctuation | Yes — worse at night | Yes — worse at night | Gradual worsening over months/years |
The combination of liver disease + acute/fluctuating confusion + asterixis strongly suggests HE rather than primary delirium or dementia. However, patients with cirrhosis can also develop delirium from other causes — always identify the precipitant rather than assuming all confusion is HE.
One-Minute Hepatic Encephalopathy Revision
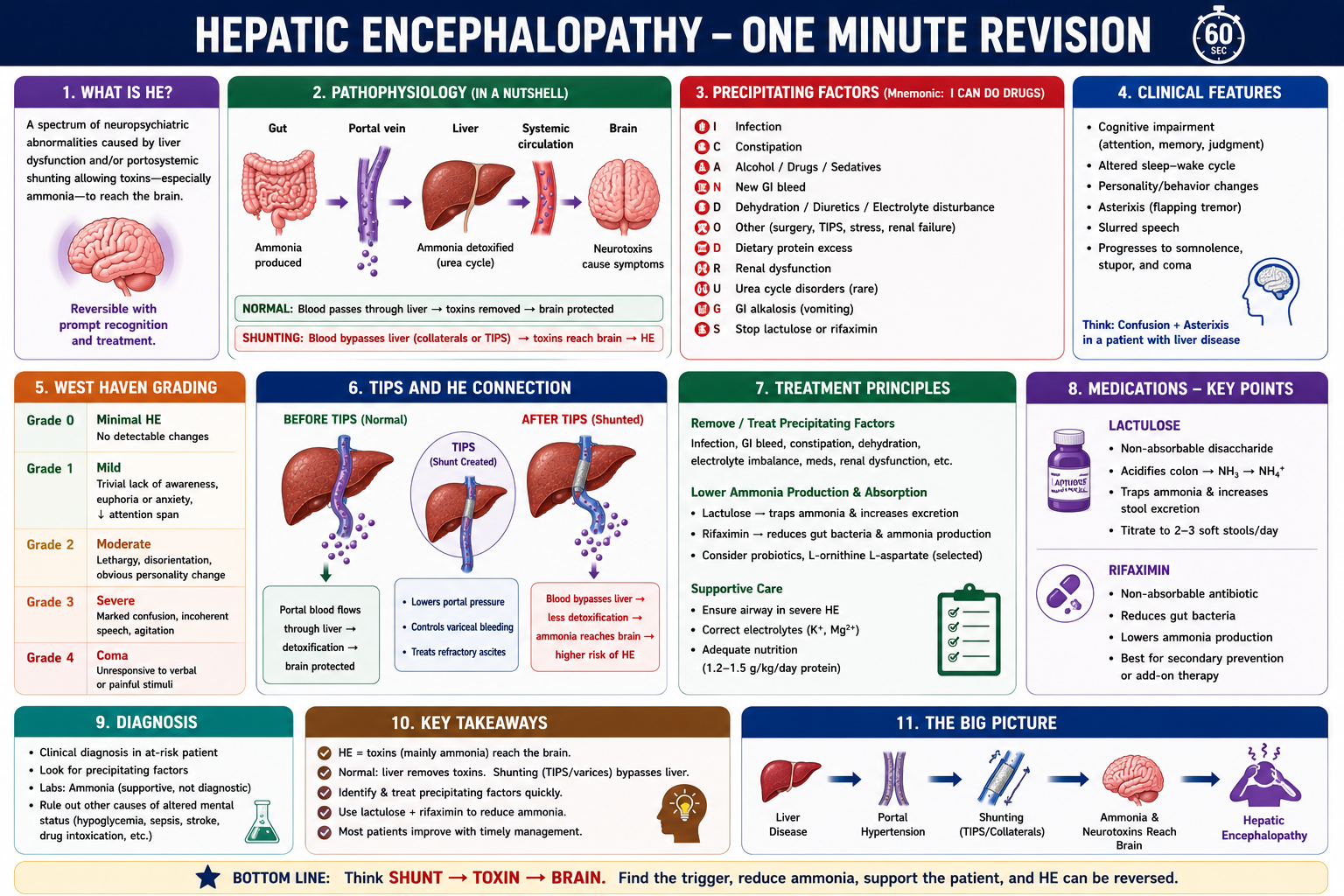
High-Yield Exam Pearls
Most important toxin = ammonia
Most important physical sign = asterixis (Grade 2)
Most common precipitant = infection
Grade 4 = coma
Lactulose = traps ammonia (acidification: NH₃ → NH₄⁺)
Rifaximin = reduces bacterial ammonia production
GI bleed → protein load → ammonia surge → HE
SBP → inflammation → brain more sensitive to toxins
TIPS → portal blood bypasses liver → HE risk ↑
HE is often reversible
- Always look for a trigger — most acute HE episodes have an identifiable precipitant; finding and treating it is the priority.
- SBP presents as HE — in a cirrhotic patient with confusion, always consider SBP and perform a diagnostic tap even if abdominal symptoms are absent.
- GI bleeding mechanism — blood is a large protein load in the gut; bacterial digestion releases a surge of ammonia that overwhelms the impaired liver.
- Lactulose mechanism — acidification of colon converts NH₃ (absorbable) to NH₄⁺ (non-absorbable, excreted in stool). Goal: 2–3 soft stools/day.
- Rifaximin is for secondary prophylaxis — not first-line for acute HE; used to prevent recurrence in patients who have already had overt HE.
- TIPS and HE — the mechanism is the same as for natural portosystemic shunting: portal blood bypasses liver detoxification. This is why pre-existing HE is a relative contraindication to TIPS.
- Ammonia vs clinical grade — ammonia does not always correlate with HE severity. HE is a clinical diagnosis; ammonia supports it but should not be used alone.
- Minimal HE — clinically silent but impairs driving ability and quality of life. Detectable only on psychometric testing.
- HE is clinical — ammonia supports the diagnosis but does not define severity or prove HE alone.
- Covert HE — may look normal on routine examination but affects driving, attention and work performance.
- Overt HE — clinically obvious HE, especially West Haven Grade 2 or above.
- Protein restriction — avoid prolonged severe restriction; malnutrition and sarcopenia worsen ammonia handling.
- Recurrent HE — suggests advanced decompensated cirrhosis and should prompt transplant-oriented thinking.
Key Takeaways
- Hepatic encephalopathy is a reversible neuropsychiatric syndrome caused by liver failure and/or portosystemic shunting
- The liver normally converts ammonia to urea via the urea cycle — in cirrhosis, this process fails
- Two mechanisms combine: impaired hepatic detoxification and portosystemic shunting that bypasses the liver
- Ammonia crosses the blood-brain barrier, causes astrocyte swelling, and impairs brain function
- Ammonia supports the diagnosis of HE, but HE remains a clinical diagnosis
- Elevated ammonia without symptoms does not prove hepatic encephalopathy
- Covert HE may impair driving and attention despite a normal routine examination
- Overt HE is clinically apparent and usually corresponds to West Haven Grades 2–4
- Recurrent HE is a marker of decompensated cirrhosis and should prompt specialist review and transplant consideration where appropriate
- Long-term severe protein restriction is usually avoided because malnutrition and sarcopenia can worsen outcomes
- West Haven grades: 0 = minimal (covert), 1 = mild confusion, 2 = lethargy + asterixis, 3 = marked confusion, 4 = coma
- Asterixis (flapping tremor) is the characteristic physical sign — typically present at Grade 2
- Common precipitants: GI bleeding, infection/SBP, constipation, dehydration, hypokalaemia, sedatives, TIPS
- GI bleeding triggers HE by providing a large protein load for bacterial ammonia production
- SBP triggers HE via systemic inflammation that increases brain sensitivity to existing toxin levels
- TIPS increases HE risk because portal blood bypasses hepatic detoxification via the stent
- Lactulose acidifies the colon, converting NH₃ to NH₄⁺ — reducing ammonia absorption. Goal: 2–3 soft stools/day
- Rifaximin reduces ammonia-producing gut bacteria — used for secondary prophylaxis of recurrent HE
- Minimal HE is clinically silent but impairs driving performance and quality of life
- HE is often reversible when the precipitant is identified and corrected promptly
Frequently Asked Questions
References
- Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014;60(2):715–735.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460.
- Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362(12):1071–1081.
- Sharma BC, Sharma P, Agrawal A, Sarin SK. Secondary prophylaxis of hepatic encephalopathy: an open-label randomized controlled trial of lactulose versus placebo. Gastroenterology. 2009;137(3):885–891.
- Prakash R, Mullen KD. Mechanisms, diagnosis and management of hepatic encephalopathy. Nat Rev Gastroenterol Hepatol. 2010;7(9):515–525.
- Ferenci P, Lockwood A, Mullen K, et al. Hepatic encephalopathy — definition, nomenclature, diagnosis, and quantification: final report of the working party at the 11th World Congresses of Gastroenterology, Vienna 1998. Hepatology. 2002;35(3):716–721.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist hepatological input when managing patients with hepatic encephalopathy.
- What Is Hepatic Encephalopathy?
- Normal Ammonia Detoxification
- Sources of Ammonia
- Pathophysiology
- Ammonia Levels
- Portosystemic Shunting
- Clinical Features & Asterixis
- West Haven Classification
- Covert vs Overt HE
- Precipitating Triggers
- Why GI Bleeding Triggers HE
- Why SBP Triggers HE
- Why TIPS Increases HE Risk
- Treatment Framework
- Lactulose Explained
- Rifaximin Explained
- Minimal Hepatic Encephalopathy
- Severity and Prognosis
- HE vs Delirium vs Dementia
- One-Minute Revision
- Exam Pearls
- Key Takeaways
- FAQ
- References