Most students memorise: Budd-Chiari syndrome = hepatic vein thrombosis.
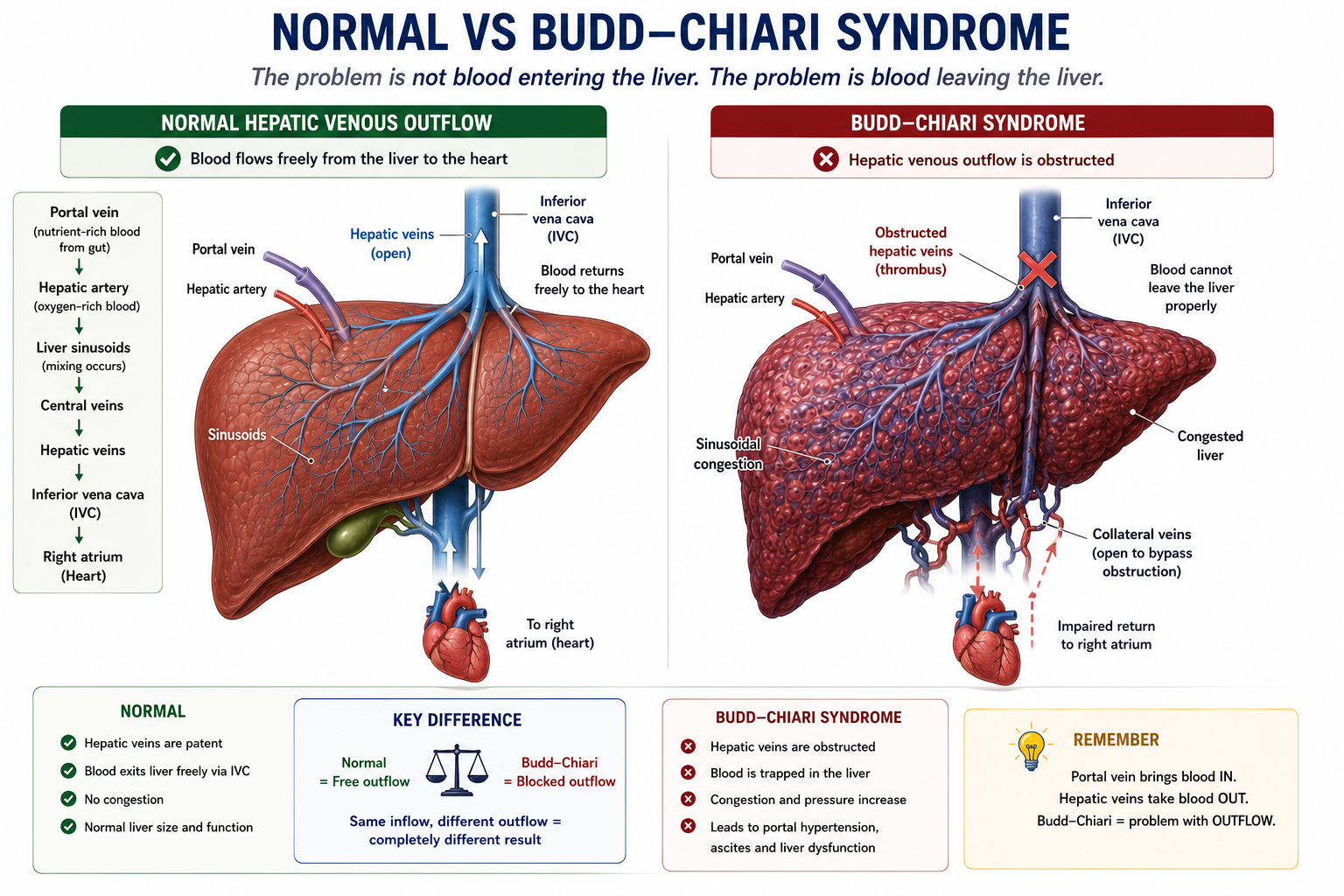
That is true, but it is not enough. The real learning point is the circulation problem: blood enters the liver normally, but cannot leave the liver normally.
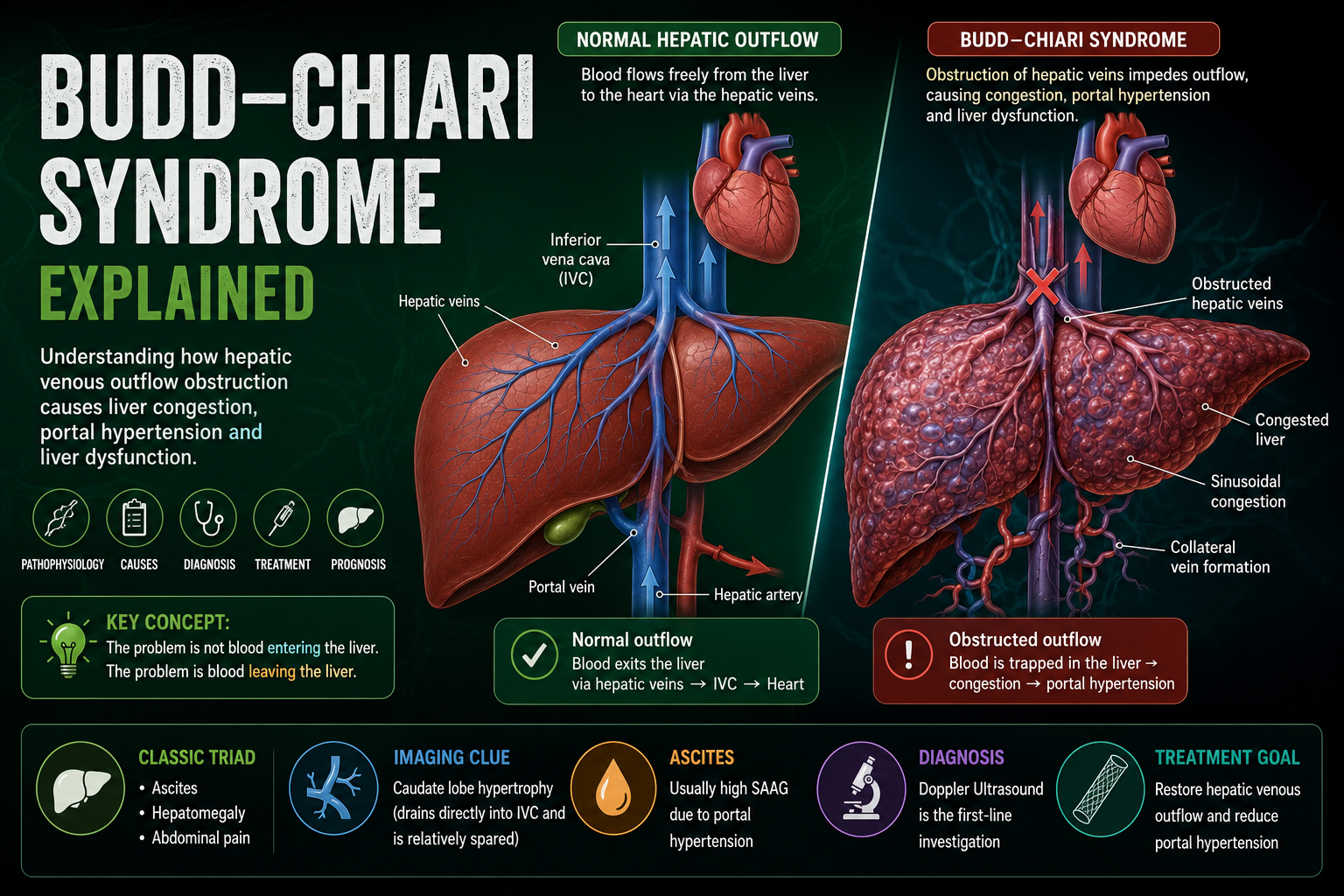
Once you see Budd-Chiari syndrome as a blocked hepatic venous drainage system, the classic findings become intuitive: painful hepatomegaly, ascites, portal hypertension and liver dysfunction.
Budd-Chiari syndrome is an outflow problem, not an inflow problem.
Learning Objectives
- Define Budd-Chiari syndrome
- Explain hepatic venous outflow obstruction
- Explain congestion, hepatomegaly, ascites and portal hypertension
- Explain caudate lobe hypertrophy
- Recognise common causes and clinical presentations
- Outline diagnosis and management
- Distinguish Budd-Chiari syndrome from portal vein thrombosis
What Is Budd-Chiari Syndrome?
Budd-Chiari syndrome is hepatic venous outflow obstruction occurring anywhere between the small hepatic veins and the junction of the inferior vena cava with the right atrium.
The obstruction is often due to hepatic vein thrombosis, but the key concept is broader than thrombosis alone. Anything that blocks hepatic venous drainage can produce the syndrome.
The problem is not blood entering the liver. The problem is blood leaving the liver.
Normal Hepatic Blood Flow
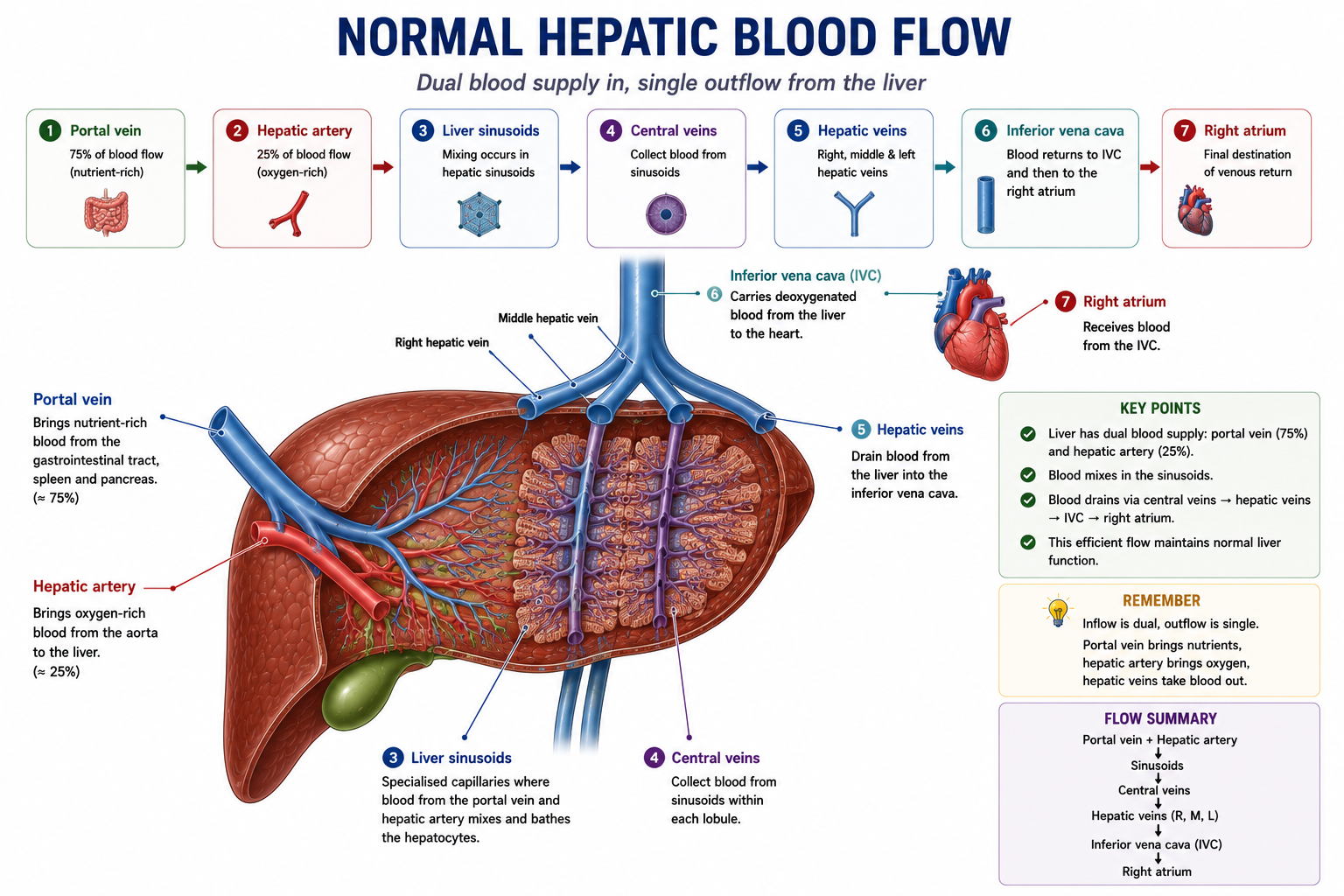
To understand Budd-Chiari syndrome, first understand normal hepatic outflow.
The portal vein and hepatic artery deliver blood into the liver. Blood then passes through sinusoids, drains into central veins, then exits through the hepatic veins into the inferior vena cava.
Understanding Budd-Chiari syndrome requires understanding normal hepatic outflow first.
Pathophysiology of Budd-Chiari Syndrome
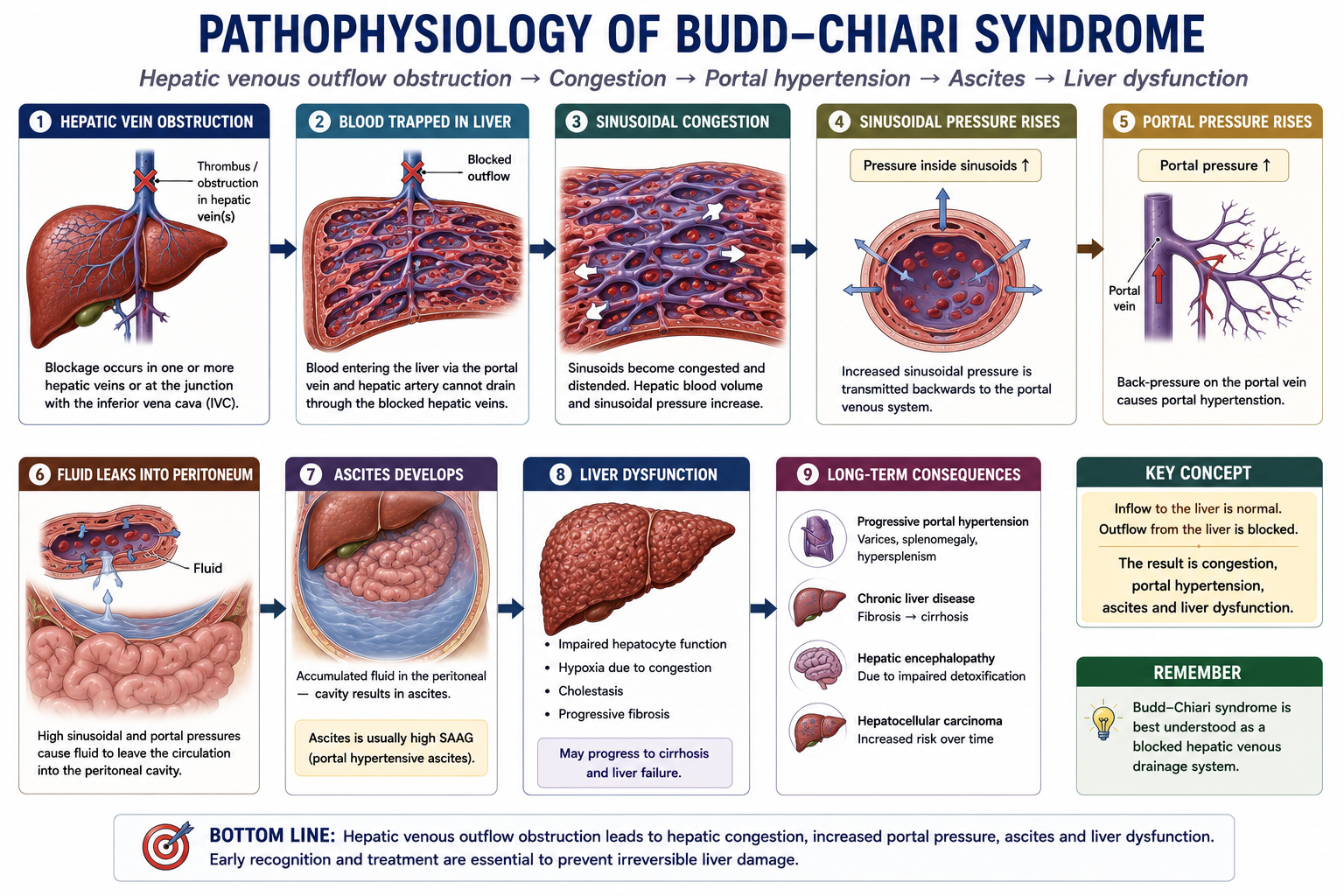
This is the most important section. Hepatic vein obstruction traps blood inside the liver. Sinusoidal pressure rises, portal pressure rises, and fluid begins to move out of the vascular space.
As congestion worsens, hepatocytes receive less effective oxygen delivery and become compressed by the congested sinusoidal circulation. This explains why severe or acute Budd-Chiari syndrome can progress to acute liver failure.
Budd-Chiari syndrome is the hepatic vein equivalent of a blocked drain.
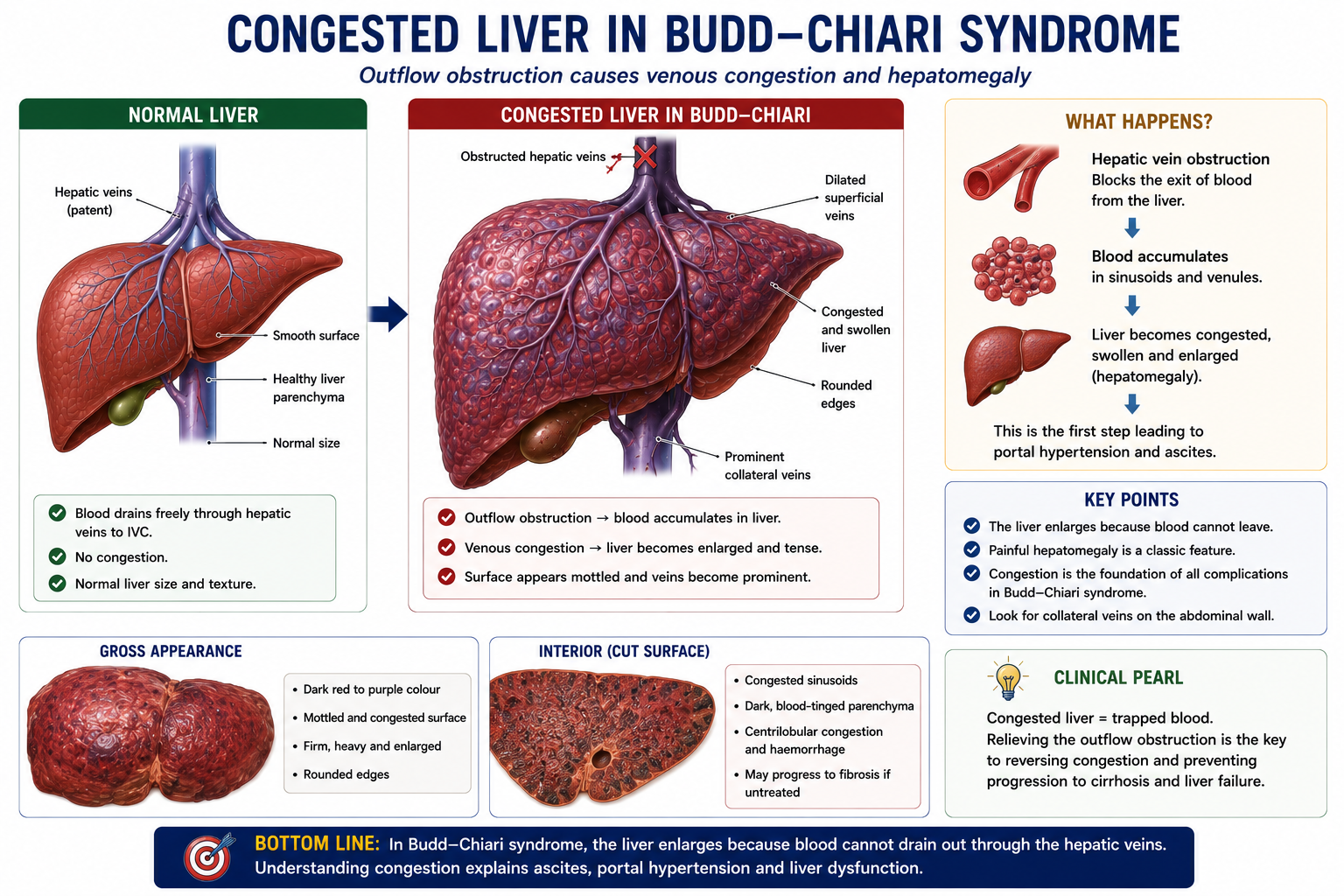
Why Does the Liver Become Enlarged?
The liver becomes enlarged because it fills with blood that cannot drain normally. This is venous congestion, not simply inflammation.
The liver capsule stretches as the organ enlarges. This stretching explains the right upper quadrant pain and tender hepatomegaly that classically appear in acute Budd-Chiari syndrome.
Painful hepatomegaly is a classic feature of Budd-Chiari syndrome.
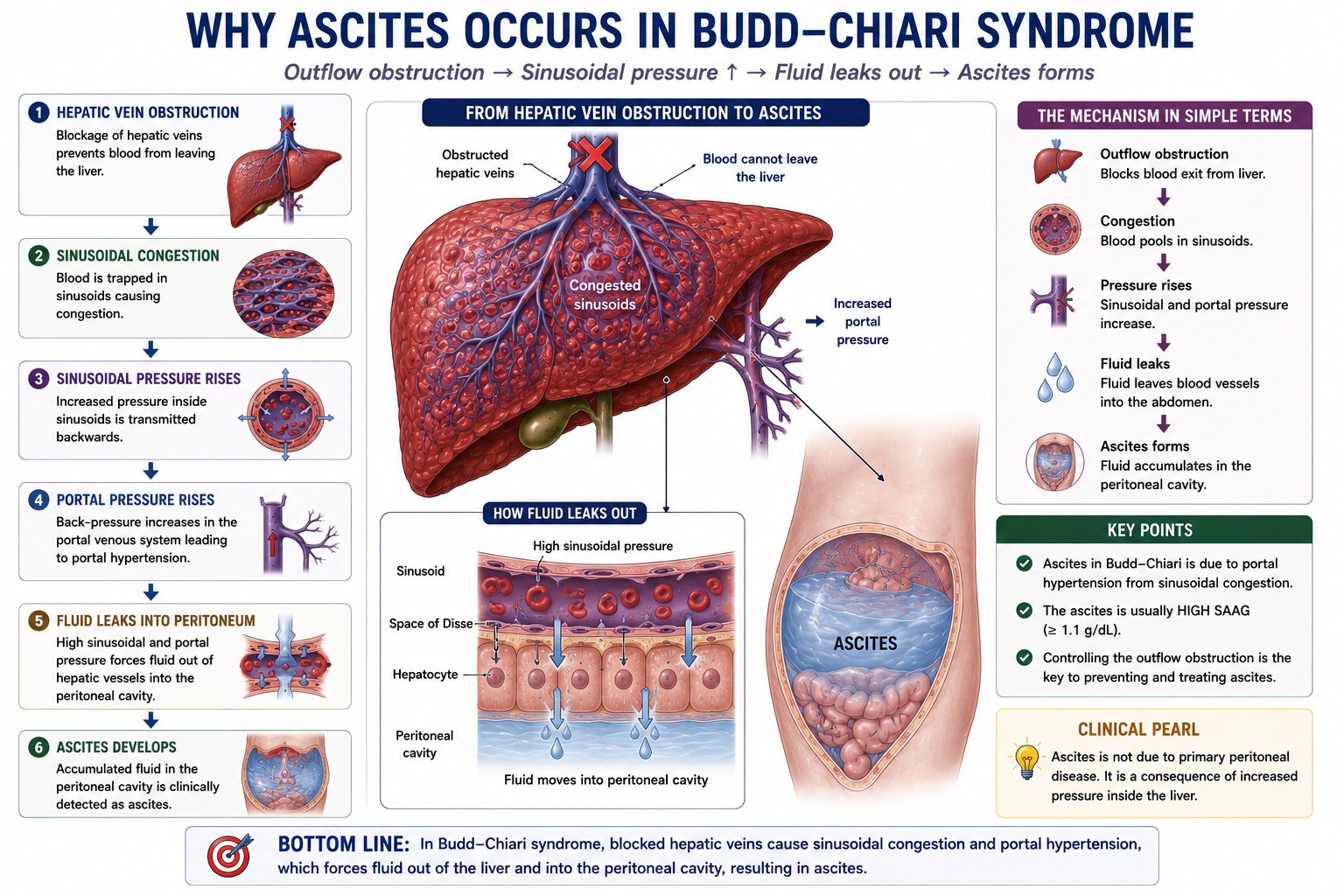
Why Does Ascites Develop?
Ascites develops because raised sinusoidal pressure drives fluid out of the hepatic and splanchnic vasculature into the peritoneal cavity.
Because the ascites is driven by raised portal pressure, Budd-Chiari syndrome usually produces a high-SAAG ascites. Read this alongside Ascites Explained and SAAG Explained.
Ascites in Budd-Chiari syndrome is usually high-SAAG because portal pressure is elevated.
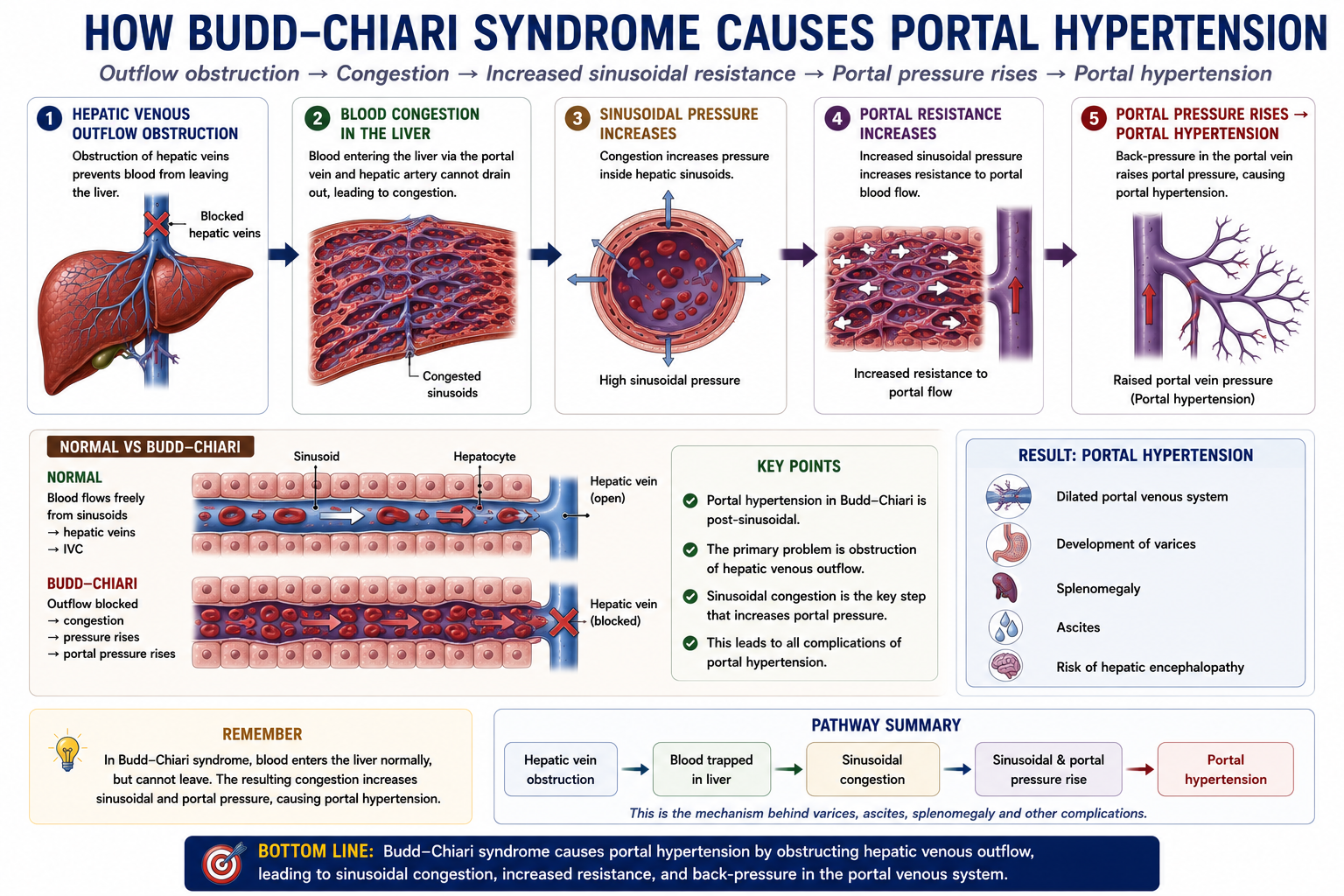
Why Does Portal Hypertension Develop?
Portal hypertension develops because hepatic venous blockage increases pressure within the sinusoidal vascular bed. Portal blood arriving from the gut now meets a congested, high-pressure liver.
This links Budd-Chiari syndrome to the wider portal hypertension cluster: ascites, varices, hepatic encephalopathy and TIPS all make more sense once the pressure pathway is clear. Review Portal Hypertension Explained for the foundation.
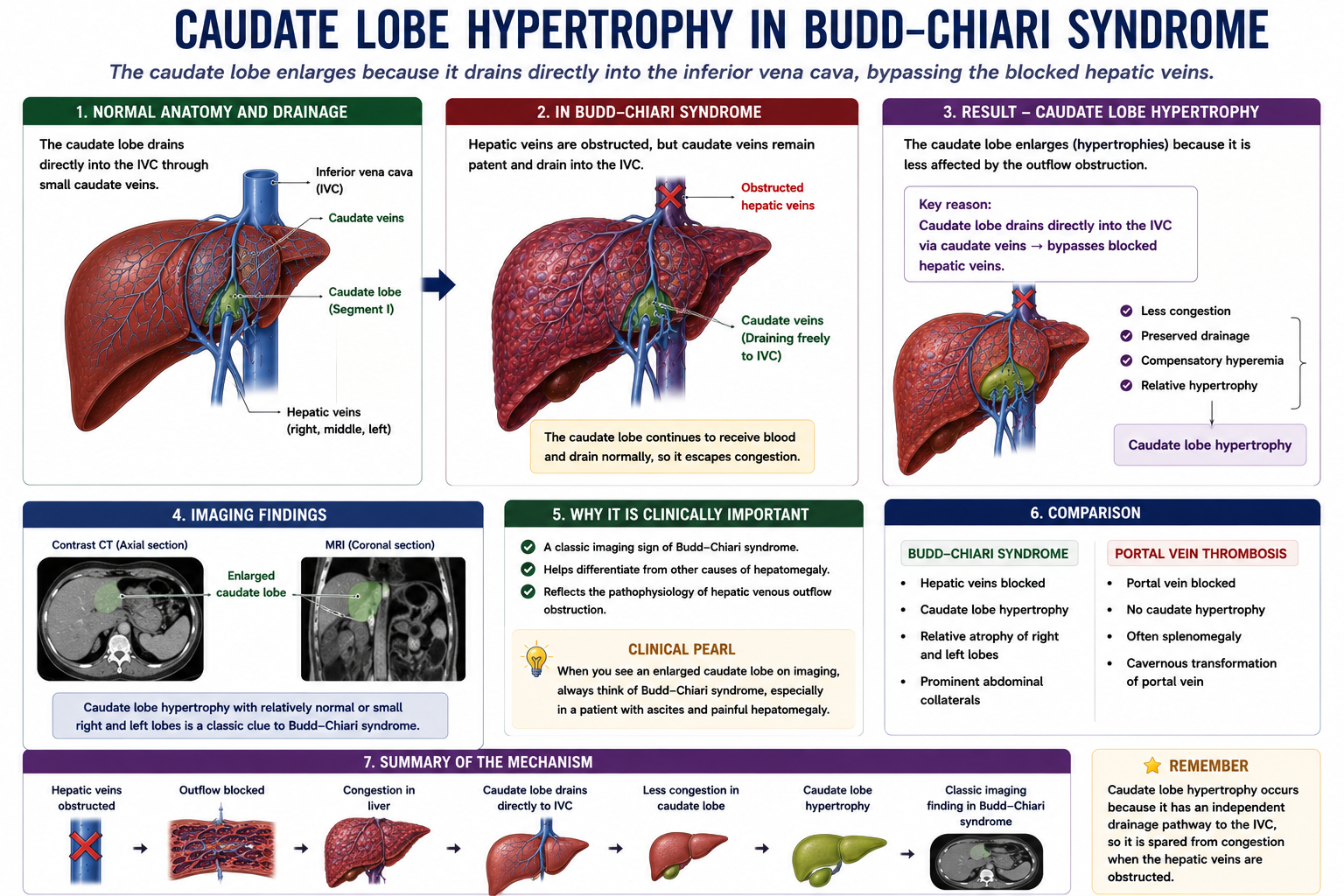
Why Does the Caudate Lobe Enlarge?
Caudate lobe hypertrophy is one of the highest-yield imaging clues in Budd-Chiari syndrome.
The caudate lobe has venous drainage that can empty directly into the inferior vena cava. When the main hepatic veins are obstructed, this direct drainage gives the caudate lobe a relative advantage, so it may enlarge.
Caudate lobe hypertrophy is a classic imaging finding in Budd-Chiari syndrome.
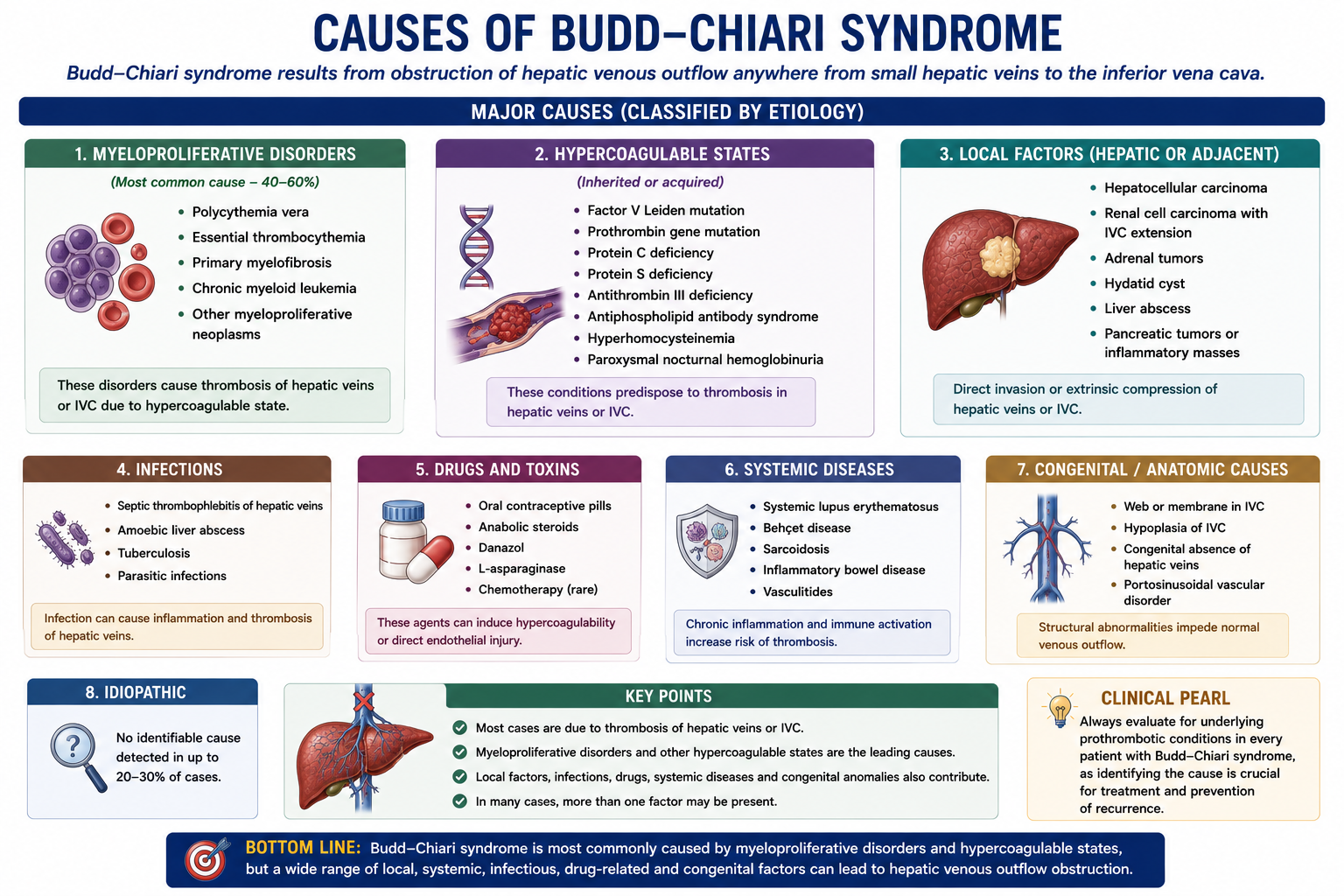
Causes of Budd-Chiari Syndrome
Most causes of Budd-Chiari syndrome share one theme: they increase the tendency to thrombosis.
| Category | Examples |
|---|---|
| Myeloproliferative disorders | Polycythaemia vera, essential thrombocythaemia |
| Inherited thrombophilia | Factor V Leiden, protein C deficiency, protein S deficiency, antithrombin deficiency |
| Acquired thrombophilia | Antiphospholipid syndrome, paroxysmal nocturnal haemoglobinuria |
| Hormonal | Oral contraceptive pill use, pregnancy |
| Malignancy | Hepatocellular carcinoma, renal cell carcinoma |
| Inflammatory and other | Behcet disease, webs or membranes involving the IVC |
When you diagnose Budd-Chiari syndrome, always ask: what pro-thrombotic condition caused the hepatic vein obstruction?
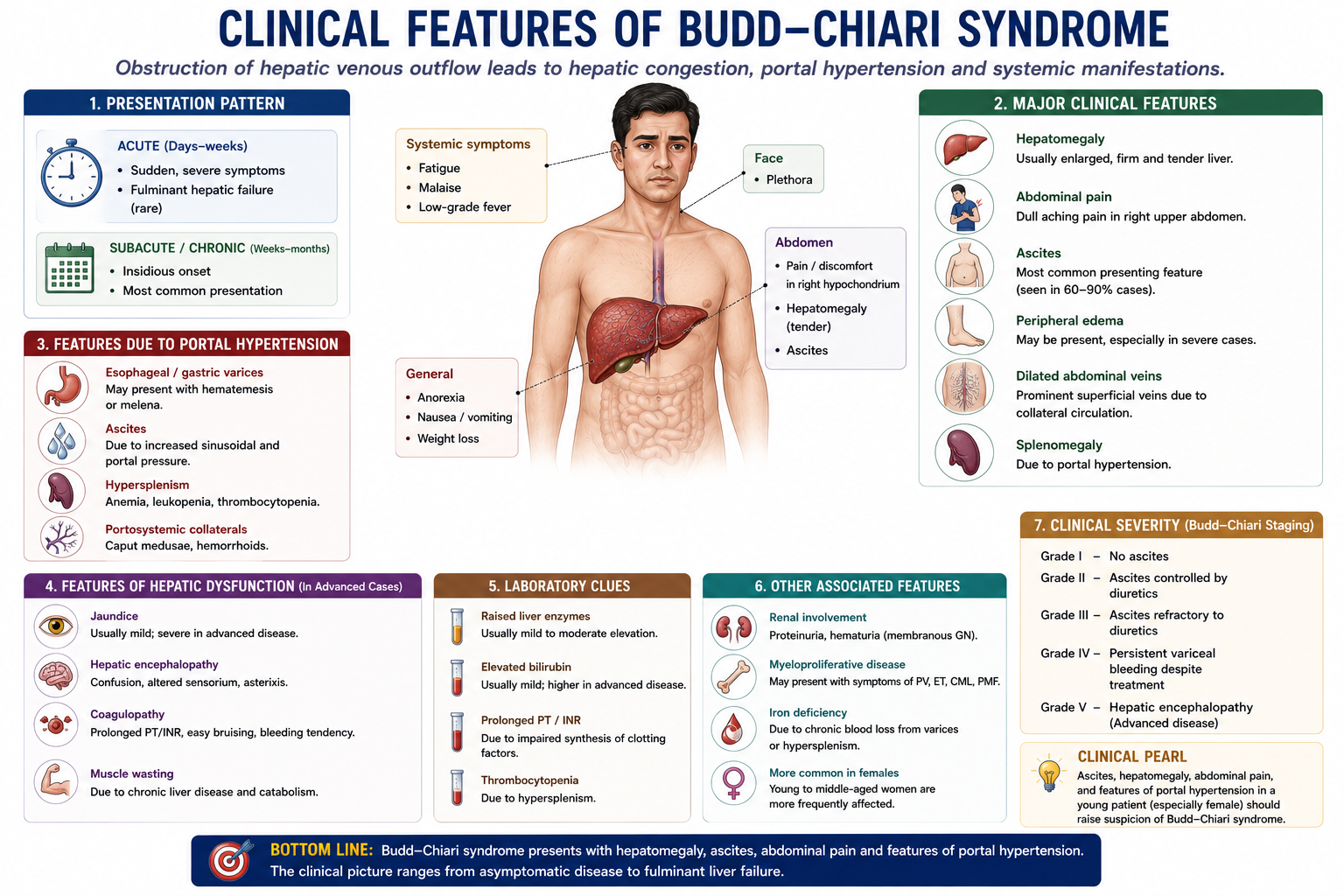
Clinical Presentation
The classic triad is abdominal pain, ascites and hepatomegaly. The presentation depends on how quickly hepatic venous outflow becomes obstructed.
Abdominal pain + ascites + hepatomegaly
| Acute Budd-Chiari | Chronic Budd-Chiari |
|---|---|
| Severe abdominal pain | Gradual abdominal distension |
| Rapid ascites | Progressive ascites |
| Tender hepatomegaly | Portal hypertension and varices |
| Jaundice and liver failure may occur | Cirrhosis-like complications may develop |
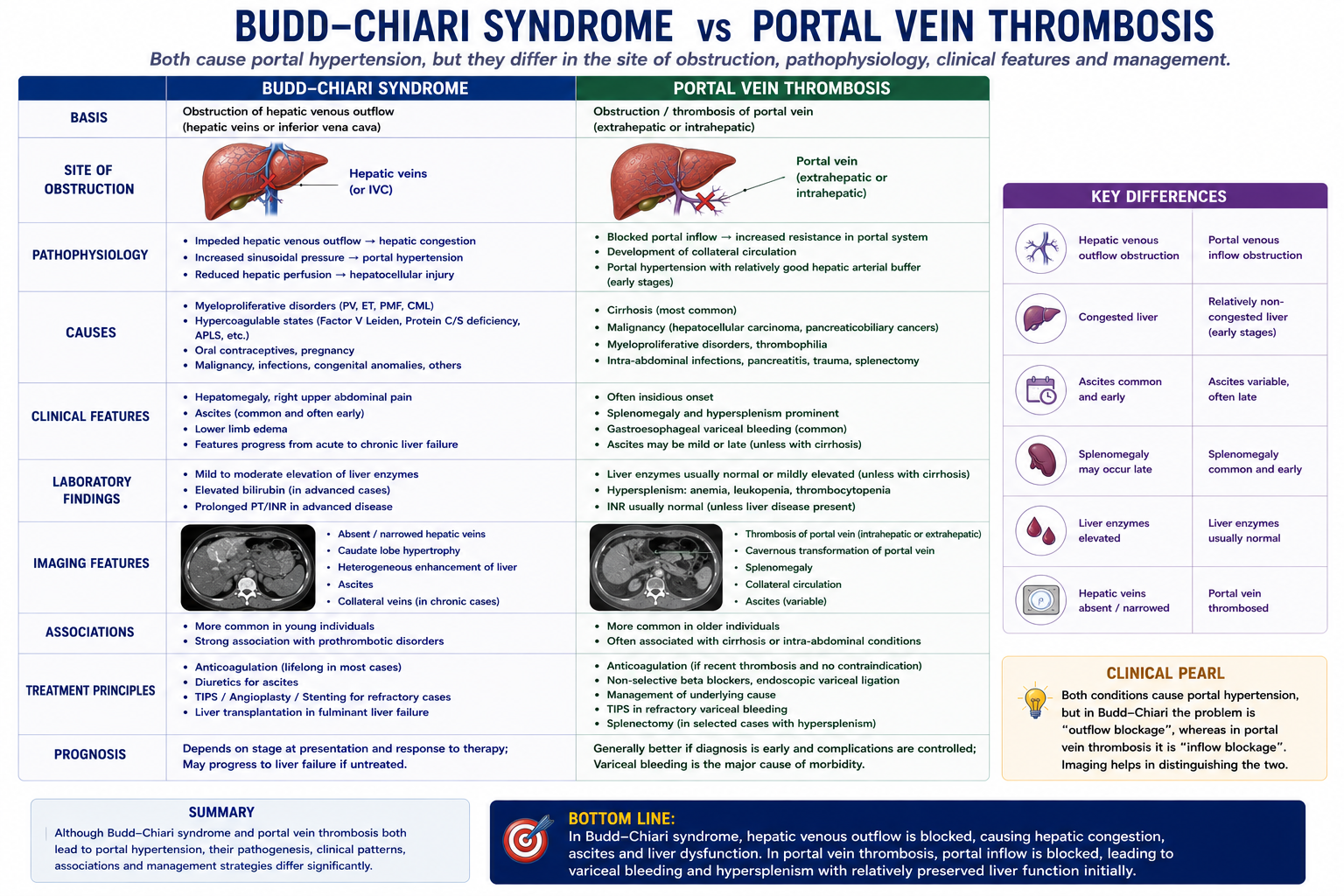
Budd-Chiari Syndrome vs Portal Vein Thrombosis
This distinction is central. Budd-Chiari syndrome is a hepatic venous outflow problem. Portal vein thrombosis is a portal venous inflow problem.
| Feature | Budd-Chiari Syndrome | Portal Vein Thrombosis |
|---|---|---|
| Blockage | Hepatic veins or hepatic venous outflow tract | Portal vein |
| Main problem | Outflow obstruction | Inflow obstruction |
| Hepatomegaly | Common, often painful | Less prominent |
| Caudate hypertrophy | Typical imaging clue | Absent |
| Ascites | Common | Variable |
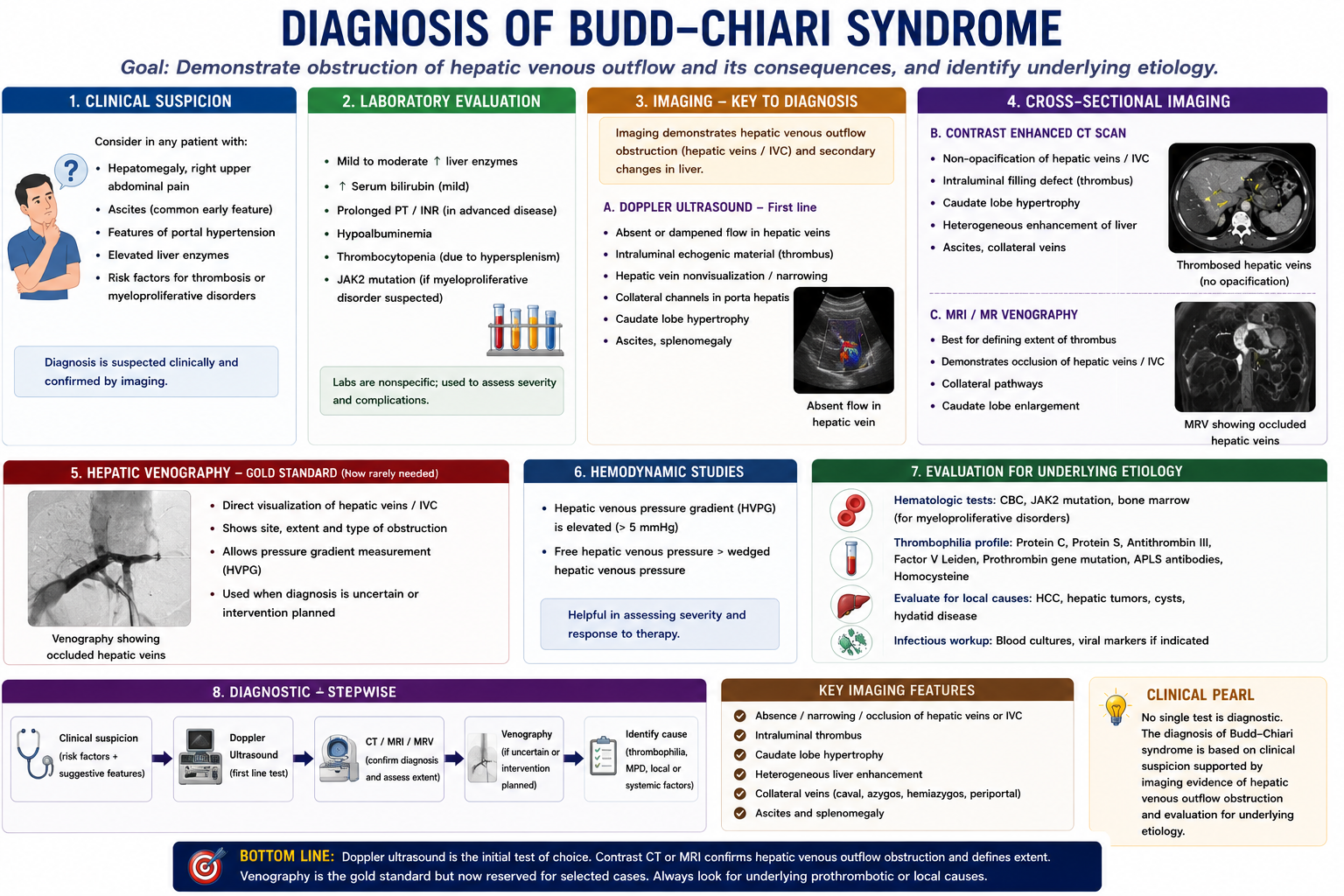
Diagnosis
Diagnosis begins with clinical suspicion: painful hepatomegaly, ascites, liver dysfunction and risk factors for thrombosis should prompt imaging.
Doppler ultrasound is usually the first-line imaging investigation. CT or MRI can define the level of obstruction, demonstrate caudate lobe hypertrophy, assess hepatic congestion and help plan intervention.
Doppler ultrasound is the first-line imaging investigation for suspected Budd-Chiari syndrome.
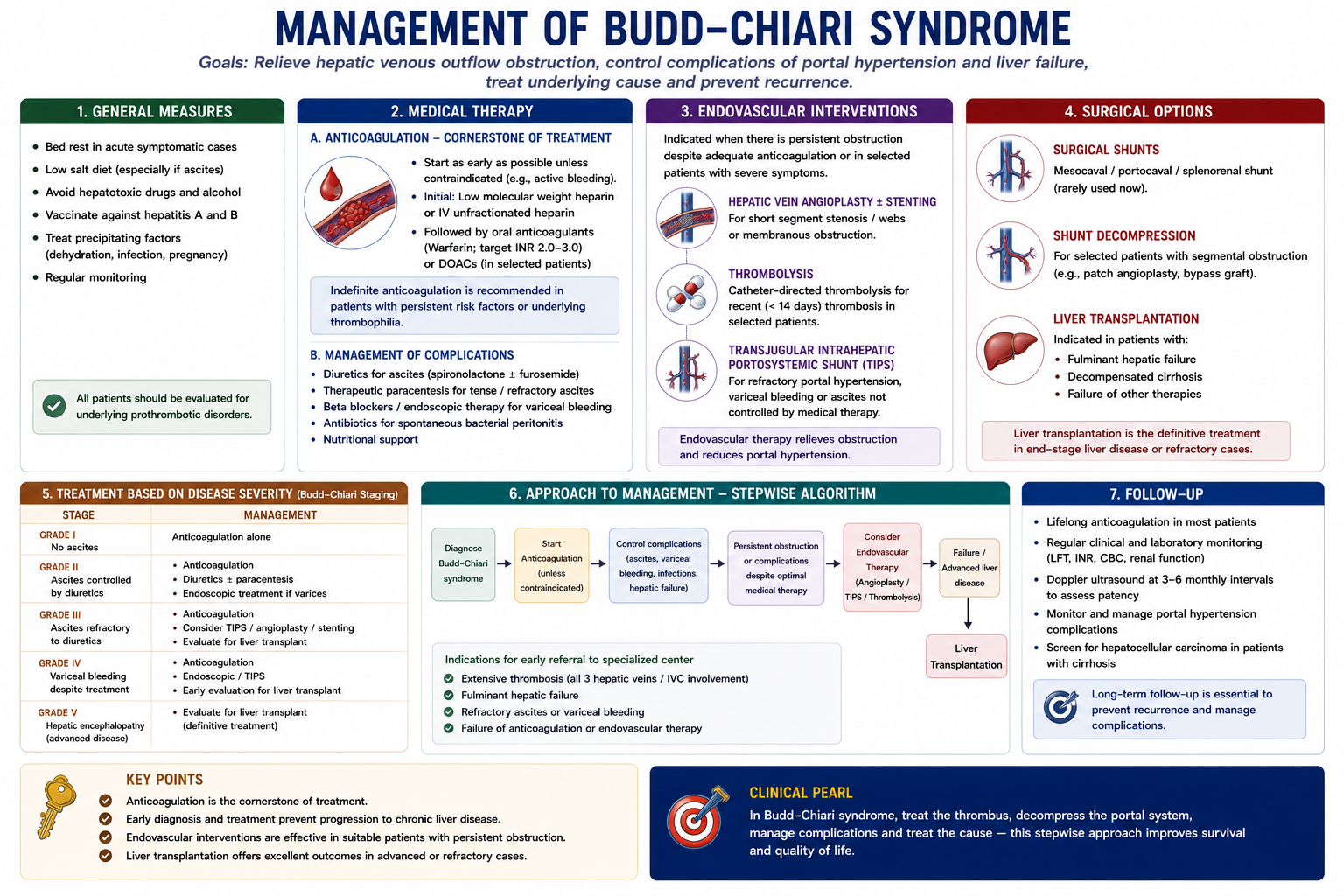
Management
Management has two goals: treat the underlying thrombotic tendency and restore or decompress hepatic venous outflow.
Anticoagulation
Anticoagulation prevents clot propagation and recurrent thrombosis. It is usually a key part of treatment unless contraindicated.
Angioplasty and Stenting
If there is a short hepatic vein or IVC stenosis, angioplasty and stenting may restore venous outflow.
TIPS
TIPS creates a decompressive channel from the portal system to the systemic venous circulation. It can reduce portal pressure and improve ascites when outflow cannot be restored directly.
Liver Transplantation
Transplantation is considered when there is fulminant liver failure, end-stage liver disease, or failure of other therapies.
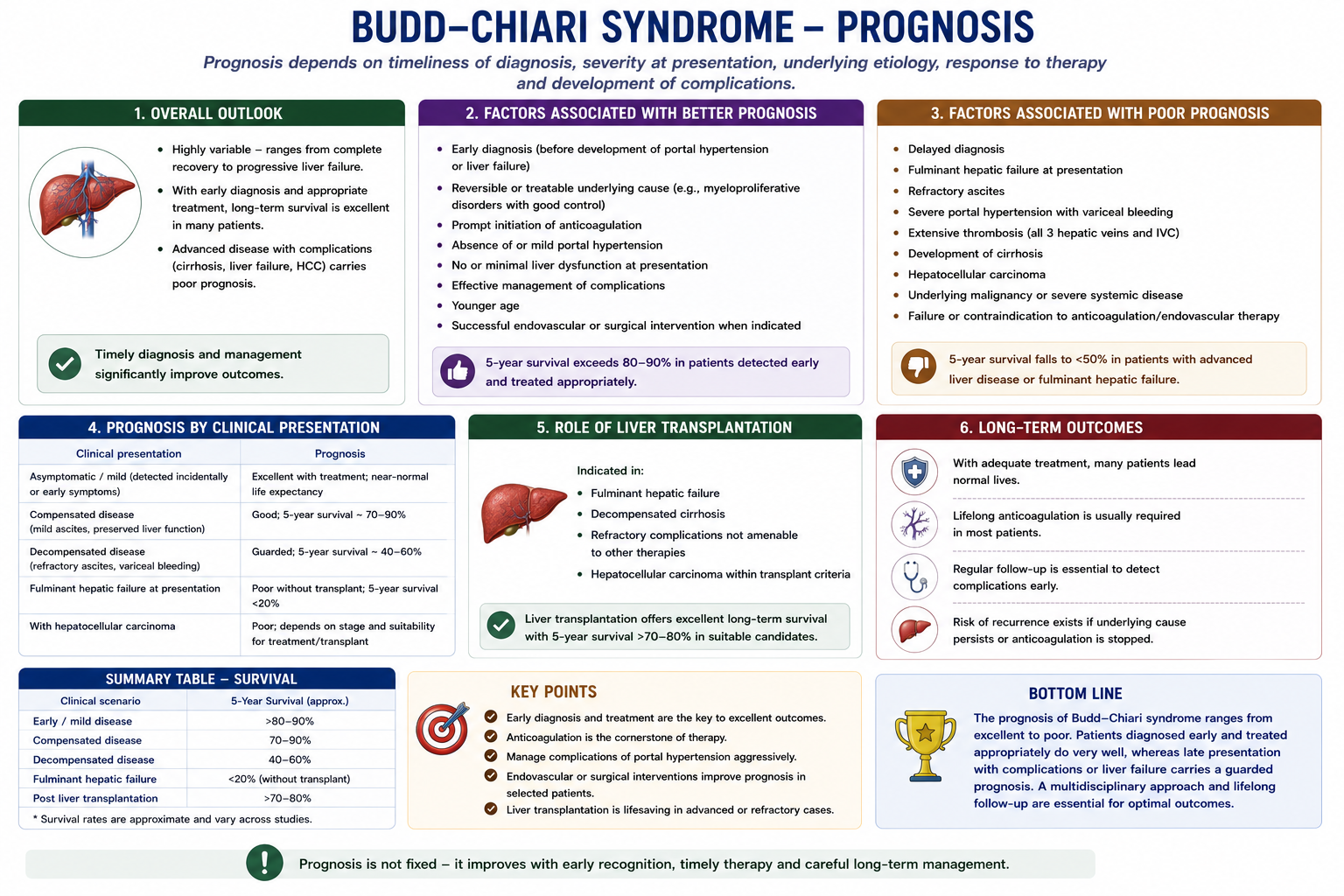
Prognosis
Untreated Budd-Chiari syndrome can progress to cirrhosis, liver failure and death. Outcomes are much better when the diagnosis is made early and hepatic venous drainage is restored or decompressed.
Modern therapy has dramatically improved survival, especially with early anticoagulation, interventional radiology and transplantation for selected patients.
Complications
- Portal hypertension
- Ascites
- Varices and variceal bleeding
- Hepatic encephalopathy
- Cirrhosis
- Liver failure
- Hepatocellular carcinoma, especially in chronic vascular liver disease
High-Yield Exam Pearls
- Budd-Chiari syndrome = hepatic venous outflow obstruction.
- Blood enters the liver normally, but blood cannot leave normally.
- Painful hepatomegaly is classic.
- Ascites is usually high-SAAG.
- Portal hypertension develops from sinusoidal congestion.
- Caudate lobe hypertrophy is a classic imaging clue.
- Most causes are pro-thrombotic disorders.
- Doppler ultrasound is first-line imaging.
- TIPS and transplantation are major treatment options.
Frequently Asked Questions
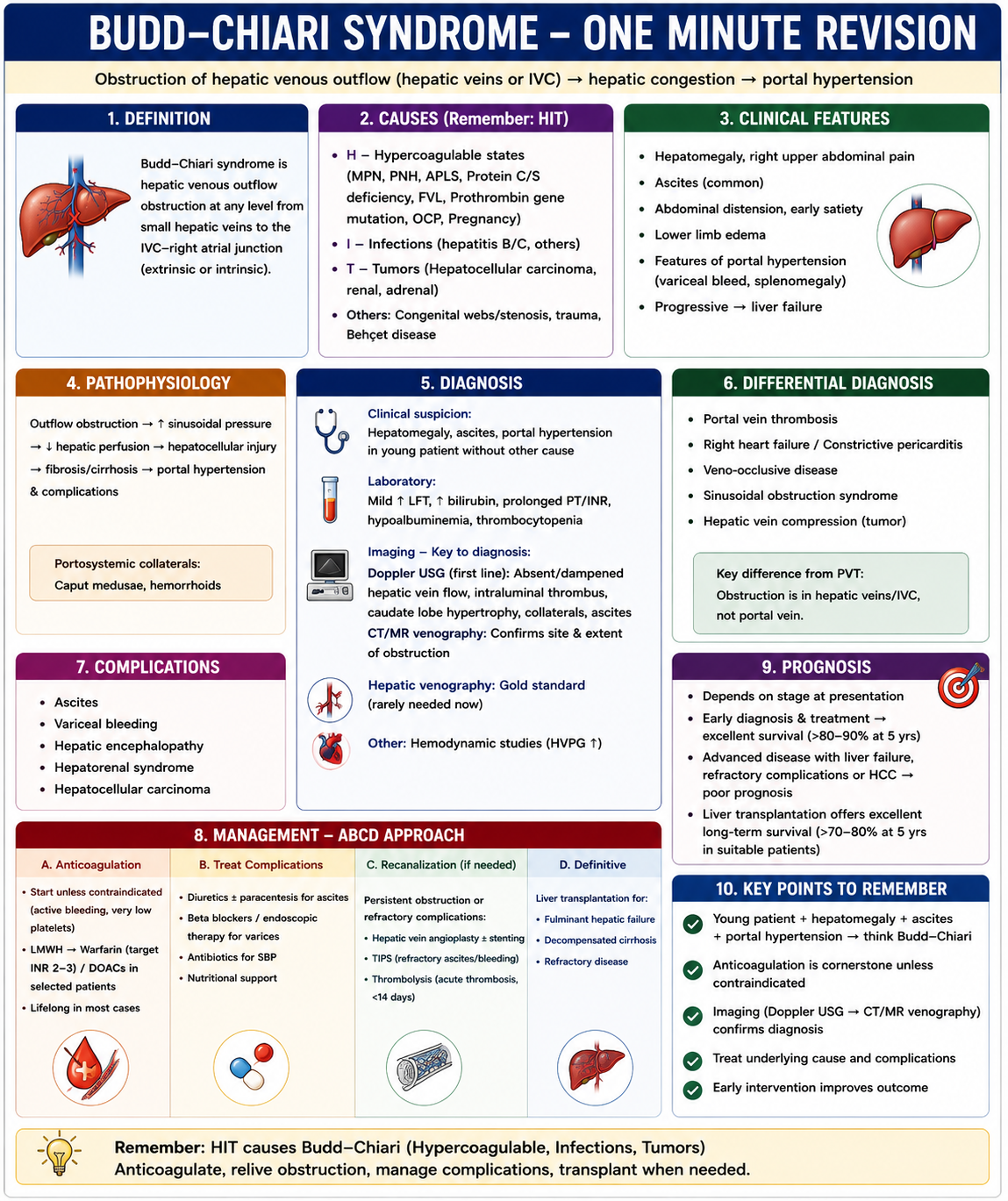
One-Minute Budd-Chiari Revision
Use this as a rapid revision frame before exams.
Classic Findings
Abdominal pain, painful hepatomegaly and ascites.
Imaging Clue
Caudate lobe hypertrophy due to direct drainage into the IVC.
Treatment ladder: anticoagulation → angioplasty/stenting → TIPS → liver transplantation.
Key Takeaways
- Budd-Chiari syndrome is hepatic venous outflow obstruction.
- It is easiest to understand as a blocked hepatic drainage system.
- Outflow obstruction causes congestion, hepatomegaly, portal hypertension and ascites.
- Caudate lobe hypertrophy is a high-yield imaging clue.
- Most causes are pro-thrombotic disorders.
- Doppler ultrasound is first-line imaging.
- Treatment escalates from anticoagulation to recanalisation, TIPS and transplantation.
References
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Vascular diseases of the liver. J Hepatol. 2016;64(1):179-202.
- DeLeve LD, Valla DC, Garcia-Tsao G. Vascular disorders of the liver. Hepatology. 2009;49(5):1729-1764.
- Valla DC. Budd-Chiari syndrome and veno-occlusive disease/sinusoidal obstruction syndrome. Gut. 2008;57(10):1469-1478.
- Martens P, Nevens F. Budd-Chiari syndrome. United European Gastroenterol J. 2015;3(6):489-500.
- Seijo S, Plessier A, Hoekstra J, et al. Good long-term outcome of Budd-Chiari syndrome with a step-wise management. Hepatology. 2013;57(5):1962-1968.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist hepatology input when investigating or managing suspected Budd-Chiari syndrome.