Portal hypertension has two major clinical branches.
One branch produces ascites, SBP and hepatorenal syndrome.
The other branch produces portosystemic collaterals, varices and variceal bleeding.
Variceal bleeding is therefore not a separate disease. It is the bleeding complication of portal hypertension — and understanding it requires understanding why portal pressure rises in cirrhosis, which was covered in Portal Hypertension Explained.
Varices form because the portal venous system is trying to bypass the high-resistance cirrhotic liver. This bypass is useful for decompressing portal pressure but dangerous because the collateral veins are thin-walled and carry high-pressure blood.
Branch 1: Portal hypertension → ascites → SBP → hepatorenal syndrome
Branch 2: Portal hypertension → portosystemic collaterals → varices → variceal bleeding
Learning Objectives
- Define variceal bleeding
- Explain why varices form in portal hypertension
- Identify common sites of portosystemic collaterals
- Explain why varices rupture
- Recognise clinical features of acute variceal bleeding
- Understand the role of endoscopy in diagnosis and treatment
- Explain band ligation in simple terms
- Distinguish primary from secondary prophylaxis
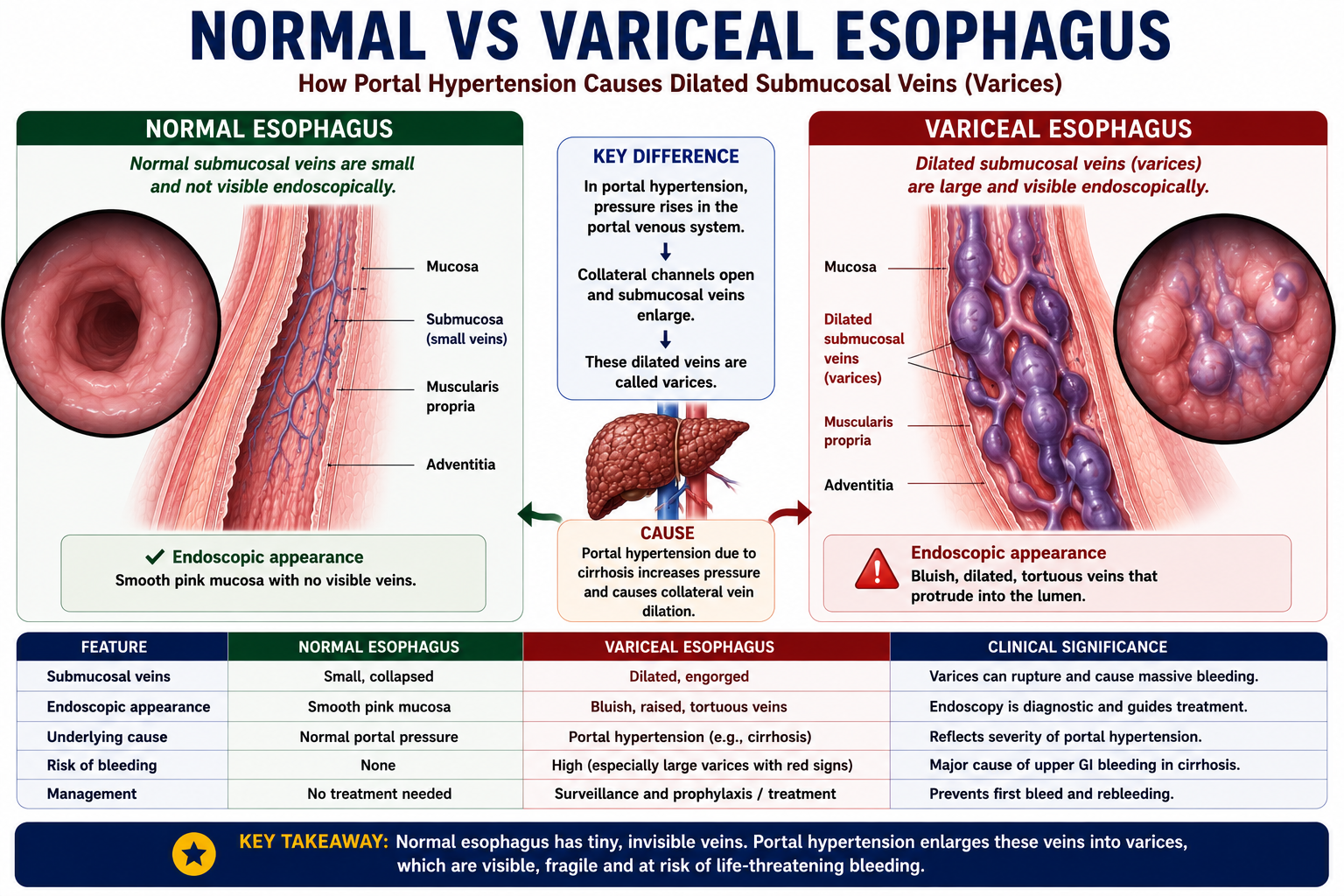
What Is Variceal Bleeding?
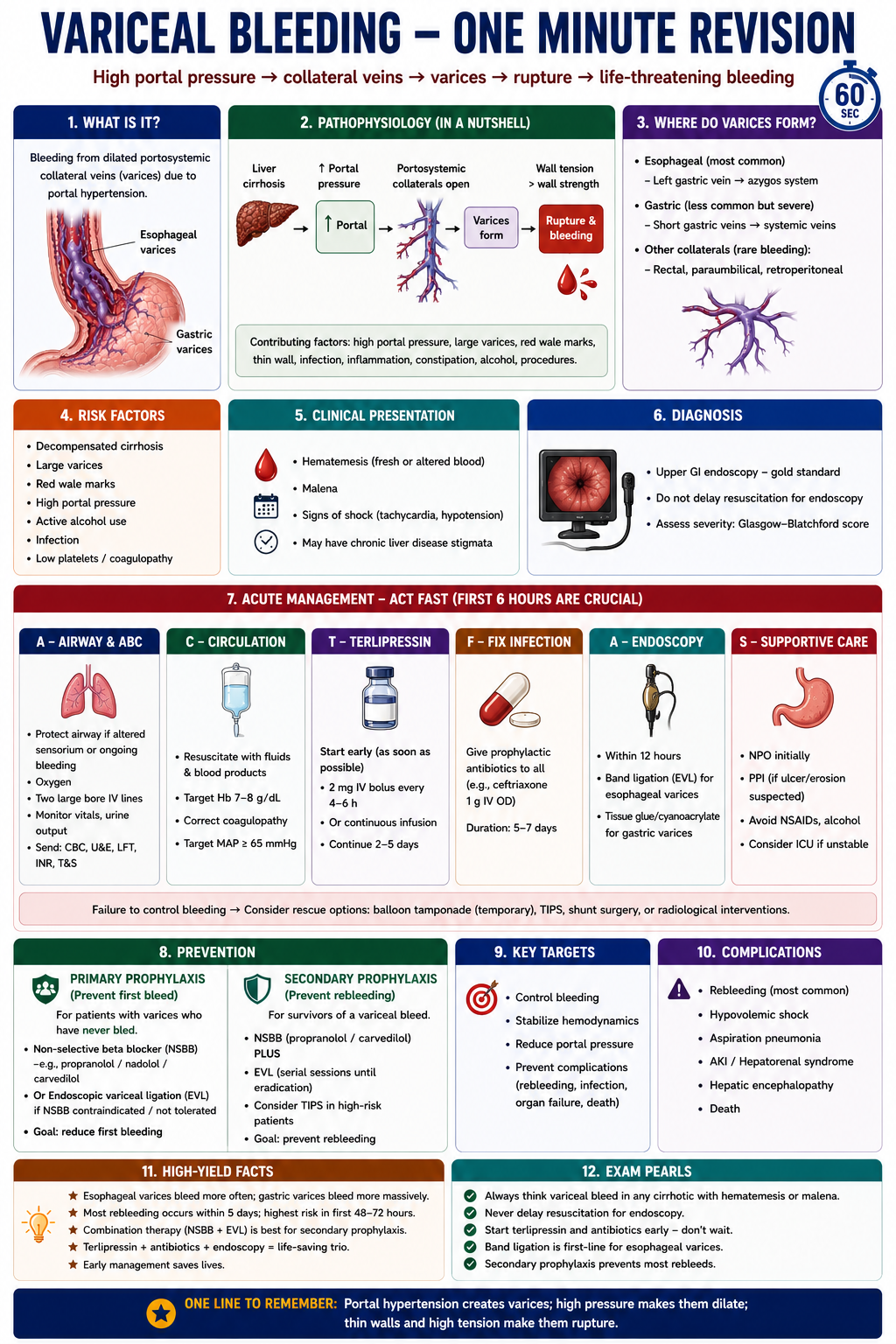
Variceal bleeding is bleeding from dilated portosystemic collateral veins that develop because of portal hypertension.
The most common clinically important site is the distal esophagus, where portal venous blood from the left gastric vein communicates with the azygos system (systemic venous drainage). When these collateral veins enlarge under sustained high pressure, they become esophageal varices.
Variceal bleeding is usually severe because portal venous pressure is high and variceal walls are thin. A single variceal rupture can cause massive haemorrhage with rapid haemodynamic compromise.
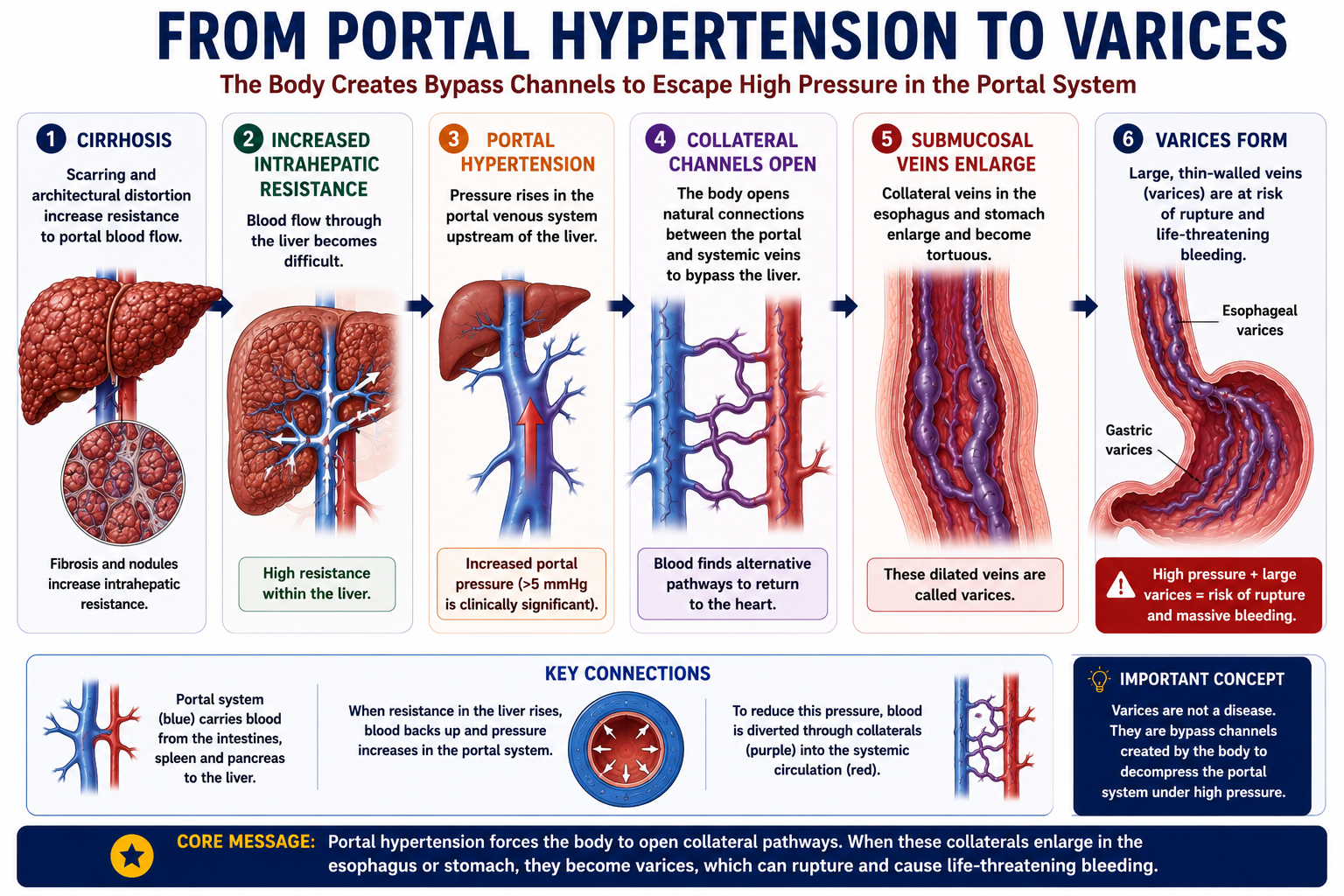
Why Do Varices Form?
In cirrhosis, scarring and architectural distortion increase resistance to portal blood flow. Portal pressure rises. The body responds by opening alternative venous channels to bypass the high-resistance liver and return blood to the systemic circulation.
These alternative channels are called portosystemic collaterals. When collaterals form and enlarge at the esophagus or stomach, they are termed varices.
When Does Portal Hypertension Become Dangerous?
Portal hypertension becomes clinically important when the pressure gradient is high enough to produce complications such as varices, ascites and bleeding.
The hepatic venous pressure gradient (HVPG) is used to estimate portal pressure in specialist settings. Two thresholds are especially important:
| HVPG Level | Clinical Meaning |
|---|---|
| >10 mmHg | Clinically significant portal hypertension. Varices and decompensation become more likely. |
| >12 mmHg | Bleeding from varices becomes possible. Reducing portal pressure below this level reduces bleeding risk. |
Varices usually form when portal pressure becomes clinically significant. Bleeding risk rises when portal pressure is high enough to overcome the strength of the variceal wall. This is why non-selective beta-blockers, vasoactive drugs and TIPS all work by reducing portal pressure.
Varices are bypass channels. They are physiologically useful — they decompress the portal system — but clinically dangerous because they carry high-pressure portal blood through thin-walled vessels that can rupture. The body's attempt to compensate creates the risk.
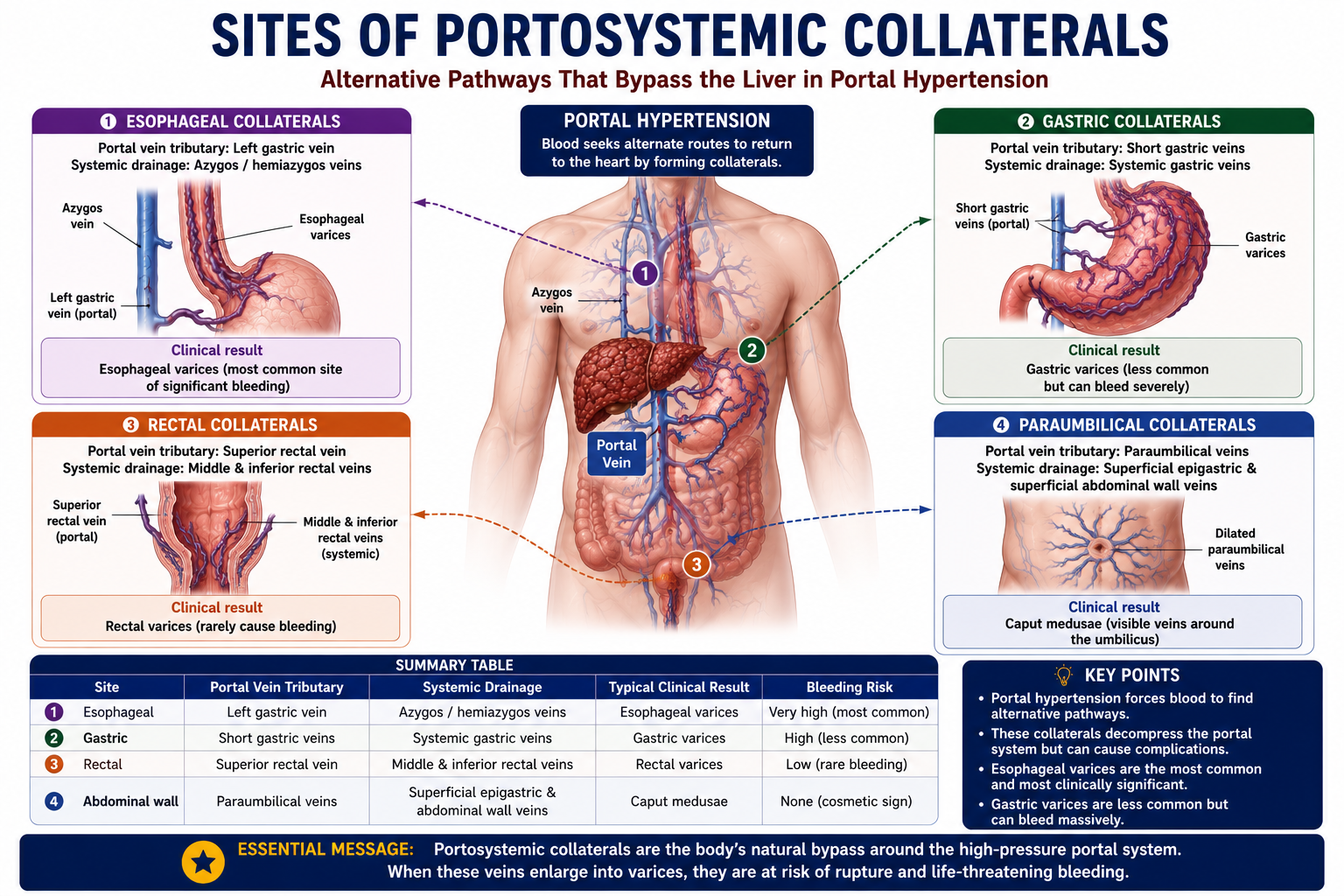
Common Sites of Portosystemic Collaterals
Portal hypertension opens collateral pathways wherever portal and systemic venous systems naturally communicate. Four clinically important sites exist:
| Site | Portal Tributary | Systemic Drainage | Clinical Result |
|---|---|---|---|
| Distal esophagus | Left gastric vein | Azygos system | Esophageal varices |
| Stomach | Short gastric veins | Systemic gastric veins | Gastric varices |
| Rectum | Superior rectal vein | Middle and inferior rectal veins | Rectal varices |
| Umbilicus | Paraumbilical veins | Superficial abdominal veins | Caput medusae |
Most important bleeding site = distal esophagus. The left gastric–azygos connection is where clinically significant bleeding most commonly occurs. All four collateral sites are testable, but esophageal varices carry the greatest clinical significance.
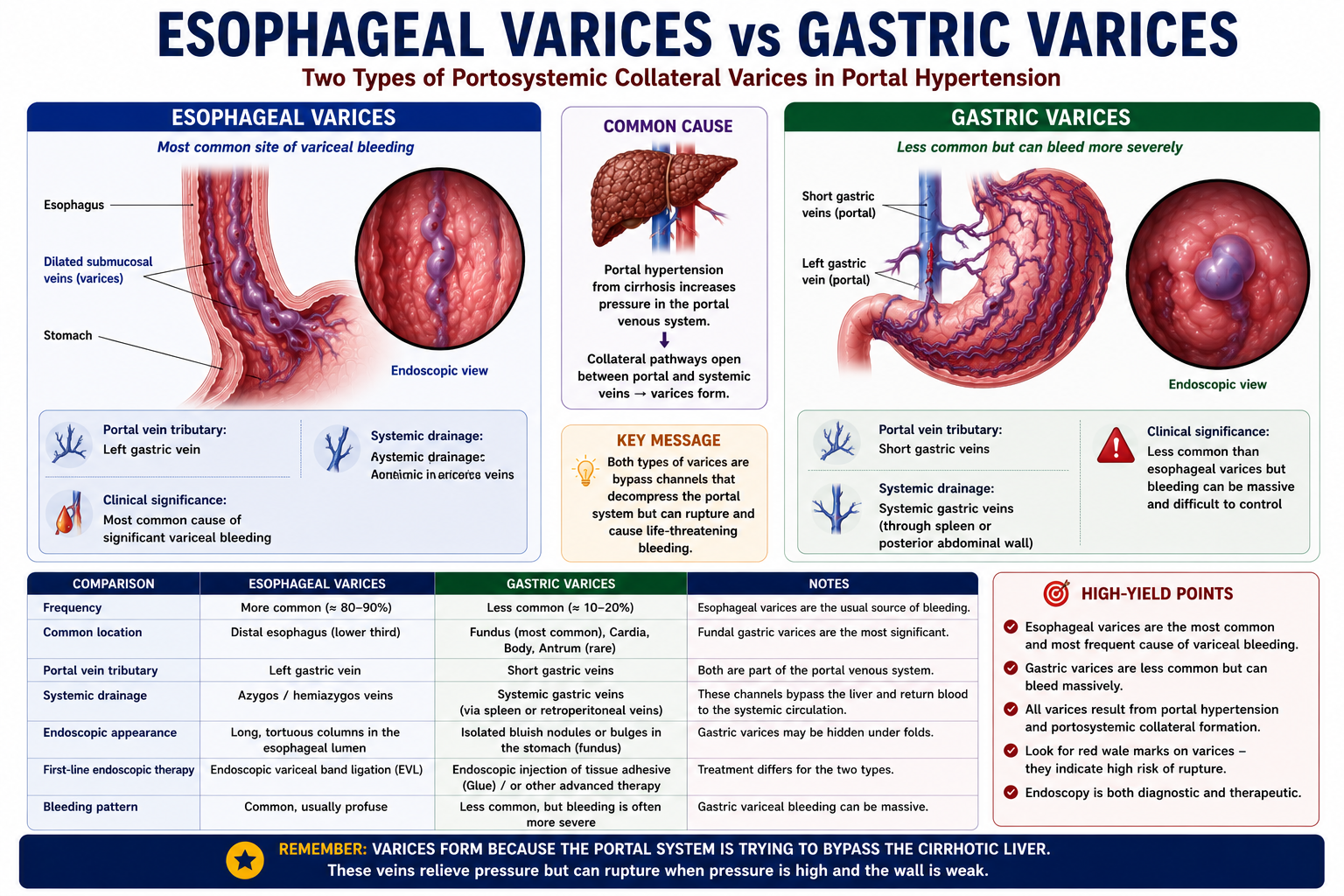
Esophageal vs Gastric Varices
Both esophageal and gastric varices are important, but they differ in frequency, bleeding pattern and management.
| Feature | Esophageal Varices | Gastric Varices |
|---|---|---|
| Frequency | More common | Less common |
| Common location | Distal esophagus | Fundus or cardia of stomach |
| Endoscopic treatment | Band ligation | Often glue injection or specialist therapy |
| Bleeding pattern | Common, can be massive | Less frequent but often severe |
| Exam focus | Very high priority | Moderate — know the difference |
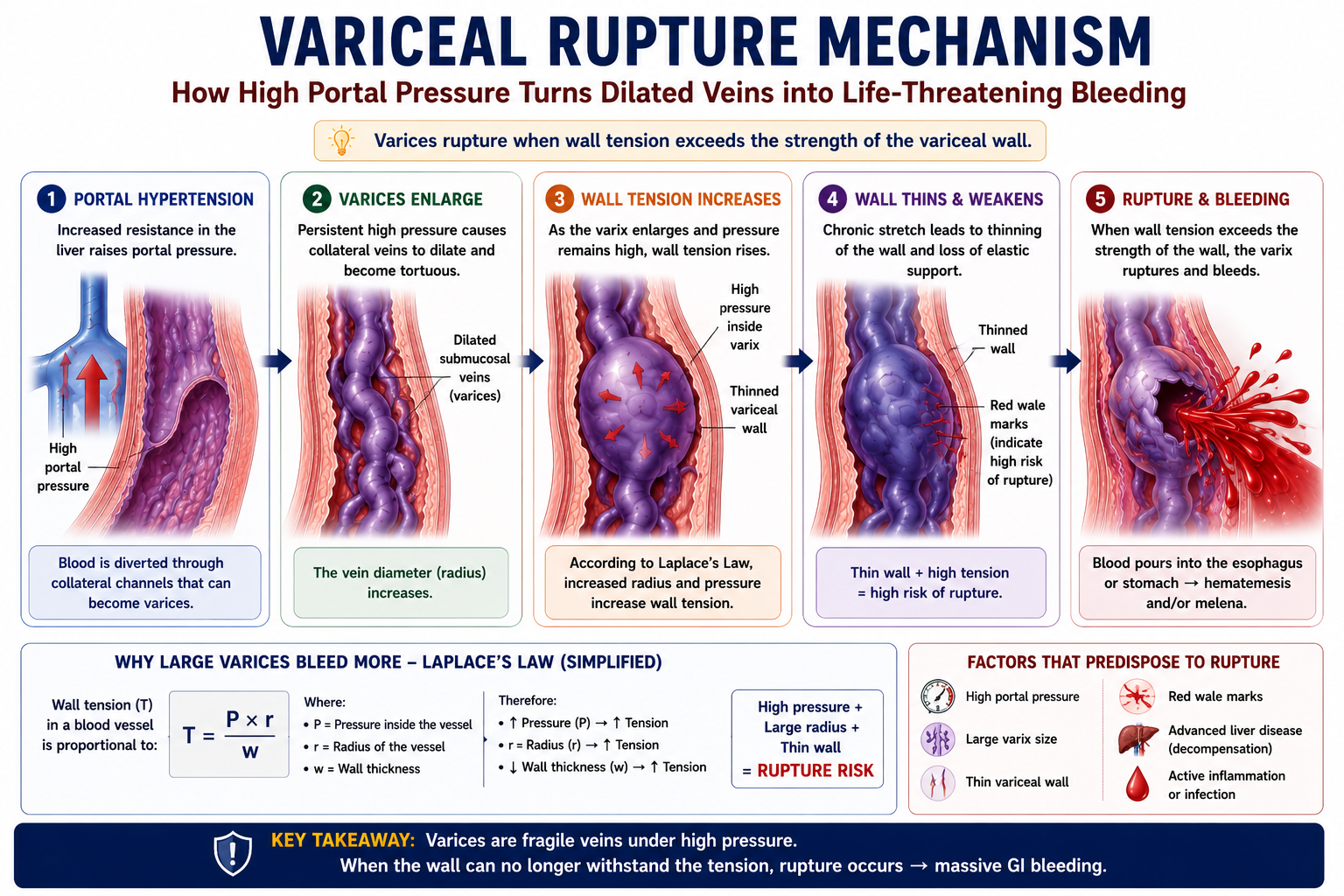
Why Do Varices Rupture?
Varices rupture when wall tension exceeds the structural strength of the variceal wall. Several factors combine to increase rupture risk:
- High portal pressure — the driving force transmitting pressure into varices
- Large variceal size — wall tension increases as vessel radius increases (Laplace's law)
- Thin variceal wall — varices have a thinner wall than normal blood vessels
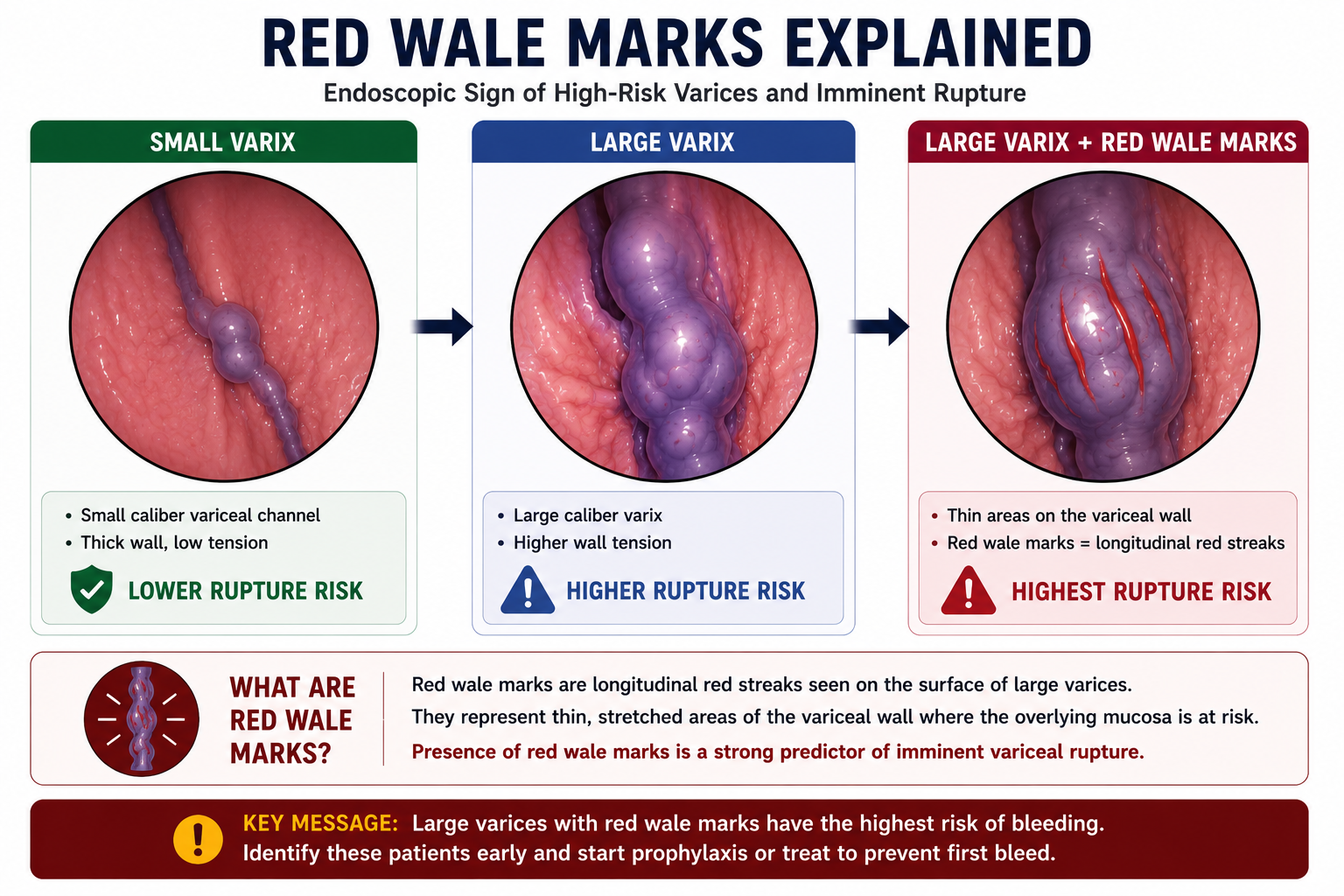
- Red wale marks — longitudinal red streaks visible on endoscopy indicating high rupture risk
- Severe liver disease — advanced liver failure worsens portal haemodynamics and reduces the ability to withstand haemorrhage
Large varix + high pressure + thin wall = rupture risk. The Laplace relationship means that as a varix enlarges, its wall tension rises disproportionately — small increases in size significantly increase rupture probability.
Red Wale Marks
Red wale marks are longitudinal red streaks on the surface of varices seen on endoscopy. They represent areas of thin epithelium over distended vessels and are an independent predictor of imminent variceal rupture. Their presence escalates the urgency of prophylactic treatment.
Risk Factors for First Variceal Bleed
Not all varices bleed. The risk of a first variceal bleed depends on variceal size, endoscopic appearance, portal pressure and severity of liver disease.
| Risk Factor | Why It Matters |
|---|---|
| Large varices | Larger radius increases wall tension, making rupture more likely. |
| Red wale marks | Endoscopic signs of thin, high-risk areas on the variceal wall. |
| Severe portal hypertension | Higher pressure increases variceal wall tension and rupture risk. |
| Advanced cirrhosis | Poor liver reserve increases bleeding risk and worsens outcome after bleeding. |
| Active alcohol use | May worsen portal pressure, liver inflammation and adherence to prophylaxis. |
The three highest-yield predictors of first variceal bleed are large varices, red wale marks, and advanced liver disease.
Clinical Presentation
Variceal bleeding is an upper gastrointestinal bleeding emergency. The presentation reflects both the site of bleeding and the underlying severity of liver disease.
- Haematemesis — vomiting of fresh red blood or altered blood (coffee grounds)
- Melaena — black tarry stools from digested upper GI blood
- Postural dizziness — reflects significant blood loss and hypovolaemia
- Syncope — in acute major haemorrhage
- Haemodynamic shock — hypotension, tachycardia, pallor, cold peripheries
- Features of chronic liver disease — jaundice, spider naevi, leukonychia, ascites, splenomegaly
In a patient with cirrhosis presenting with haematemesis, variceal bleeding must be assumed until proven otherwise by endoscopy. Resuscitation and urgent endoscopic assessment should not be delayed while waiting for other investigations.
Diagnosis
Upper gastrointestinal endoscopy (OGD) is the key diagnostic and therapeutic investigation. It should be performed urgently — usually within 12 hours of presentation, or immediately if there is haemodynamic instability.
Endoscopy identifies:
- Source of bleeding — confirms varices are responsible (versus peptic ulcer, Mallory-Weiss tear, etc.)
- Size of varices — small, medium or large
- Red wale marks — high rupture-risk stigmata
- Active bleeding or recent stigmata — confirms active haemorrhage
- Need for endoscopic therapy — allows immediate band ligation
Endoscopy is both diagnostic and therapeutic. In the same procedure, the diagnosis is confirmed and band ligation can be performed. This dual role makes urgent endoscopy essential in any suspected variceal bleed.
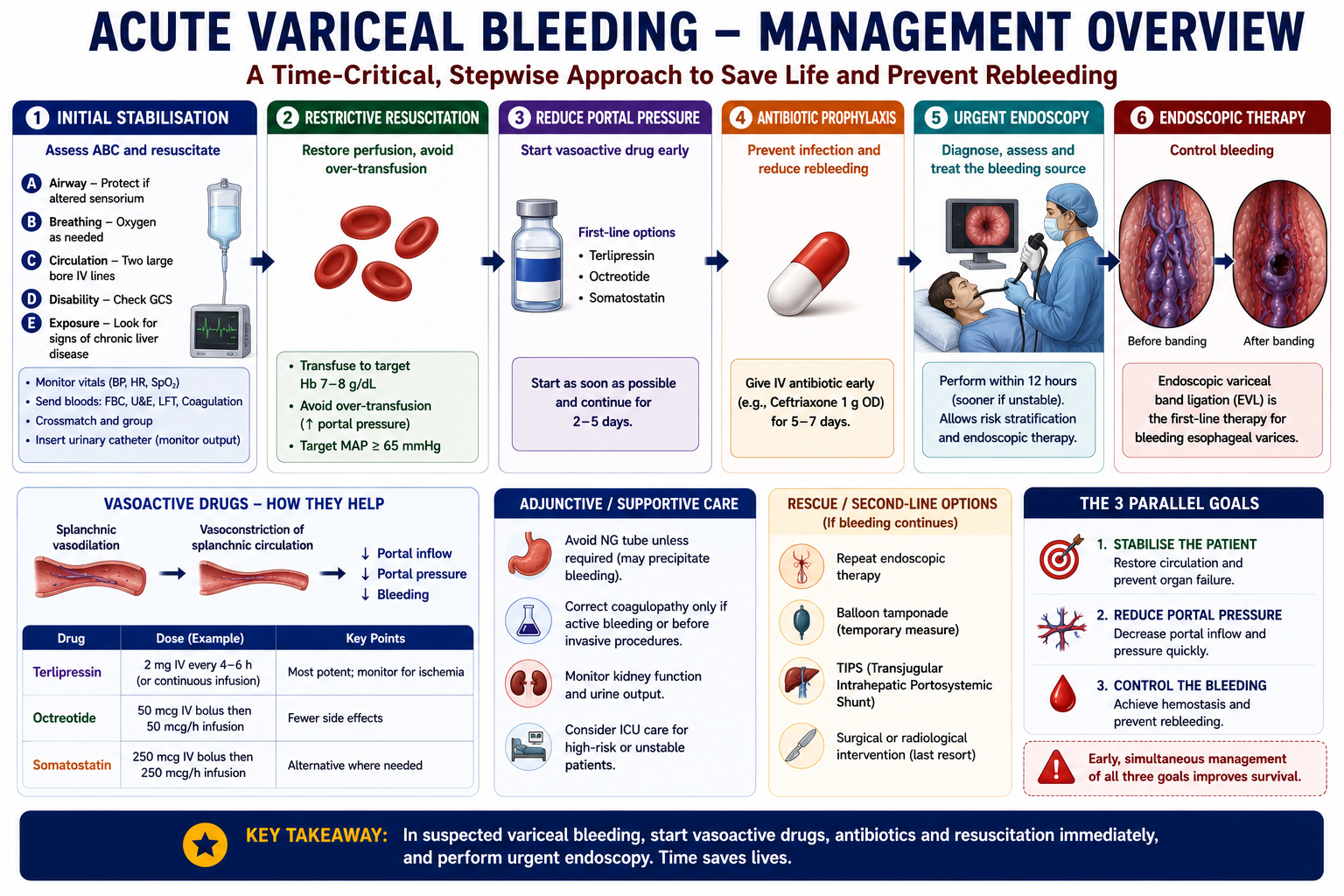
Acute Management Principles
Acute variceal bleeding management has three parallel goals: stabilise the patient, reduce portal pressure, and control the bleeding source.
- 1ABC resuscitation — airway protection (especially in encephalopathic patients), IV access, fluid resuscitation.
- 2Restrictive transfusion strategy — transfuse to haemoglobin of 70–80 g/L. Over-transfusion raises portal pressure and increases rebleeding risk.
- 3Vasoactive drug — terlipressin or somatostatin analogues (e.g. octreotide) reduce portal pressure, constrict splanchnic vasculature, and reduce variceal blood flow. Start before endoscopy.
- 4Antibiotic prophylaxis — given to all cirrhotic patients with GI bleeding. Reduces bacterial infection, SBP risk, and rebleeding. Quinolones or cephalosporins are typically used.
- 5Urgent endoscopy — confirms diagnosis and allows direct haemostatic therapy. Target within 12 hours of presentation.
- 6Band ligation — first-line endoscopic therapy for active esophageal variceal bleeding. Immediate haemostasis in most cases.
Three key concepts always tested: (1) vasoactive drugs reduce portal pressure before endoscopy, (2) antibiotics are mandatory in all GI bleeding in cirrhosis, (3) restrictive transfusion strategy — not liberal transfusion — is the evidence-based approach.
Band Ligation Explained
Endoscopic variceal band ligation (EVL) places small rubber bands around varices through the endoscope. It is the first-line endoscopic therapy for bleeding esophageal varices.
↓ Varix suctioned into a cap attached to the scope tip
↓ Rubber band deployed around the base of the varix
↓ Varix strangulated — blood flow cut off
↓ Varix thromboses over the following days
↓ Varix sloughs off, leaving a superficial ulcer that heals
↓ Bleeding controlled
Multiple bands may be placed in a single session. Sessions are typically repeated every 2–4 weeks until varices are eradicated. Band ligation is both a haemostatic and prophylactic procedure — it is used acutely to control bleeding and electively to eradicate varices and prevent future bleeds.
Endoscopic variceal ligation (EVL) has largely replaced injection sclerotherapy as the preferred endoscopic technique. EVL has fewer complications, lower rebleeding rates and better variceal eradication. Know that sclerotherapy exists as an alternative but EVL is now standard.
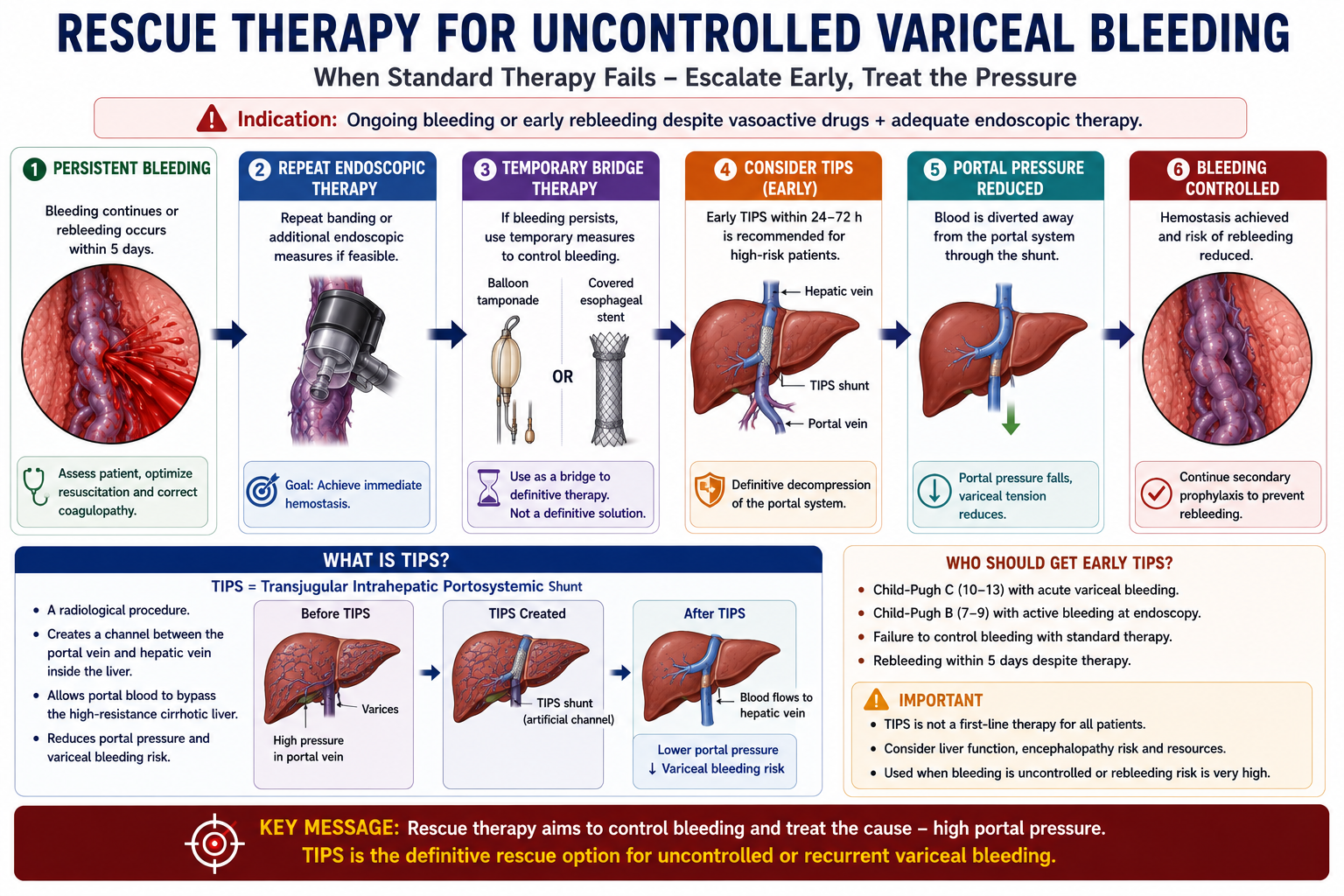
What If Bleeding Cannot Be Controlled?
Most esophageal variceal bleeds can be controlled with vasoactive drugs and endoscopic band ligation. However, some patients continue to bleed or rebleed early despite standard therapy.
In that situation, rescue therapy is needed. The goal is to temporarily control haemorrhage and reduce portal pressure more definitively.
TIPS stands for Transjugular Intrahepatic Portosystemic Shunt. It creates an artificial channel between the portal vein and hepatic vein inside the liver. This diverts blood away from the high-pressure portal system, lowers portal pressure and reduces variceal bleeding risk. TIPS is used for uncontrolled or recurrent variceal bleeding when standard therapy is insufficient.
Primary vs Secondary Prophylaxis
| Type | When Given | Aim |
|---|---|---|
| Primary prophylaxis | Varices present but no previous variceal bleed | Prevent the first bleed |
| Secondary prophylaxis | After a variceal bleed has occurred | Prevent recurrent bleeding |
Primary Prophylaxis
Patients with medium or large varices on endoscopy, or varices with red wale marks, are at significant risk of a first bleed. Non-selective beta-blockers (e.g. propranolol, carvedilol) reduce portal pressure by reducing cardiac output and splanchnic blood flow. Band ligation is an alternative for patients who cannot tolerate beta-blockers.
Secondary Prophylaxis
After a variceal bleed, rebleeding risk is high — historically up to 60–70% without prophylaxis. Secondary prophylaxis combines non-selective beta-blockers with repeated band ligation sessions until varices are eradicated. This combination is more effective than either alone.
Secondary prophylaxis is the highest-yield prophylaxis concept. After a first variceal bleed, always start non-selective beta-blocker + band ligation. Remember: non-selective (not cardioselective) beta-blockers are needed because splanchnic vasoconstriction requires beta-2 blockade.
Prognosis
Variceal bleeding indicates clinically significant portal hypertension and advanced liver disease. Mortality depends on several factors:
- Severity of underlying liver disease (Child-Pugh class, MELD score)
- Haemodynamic status at presentation — shock worsens outcomes
- Early rebleeding within the first five days
- Bacterial infection — including SBP precipitated by the bleed
- Renal dysfunction — including hepatorenal syndrome
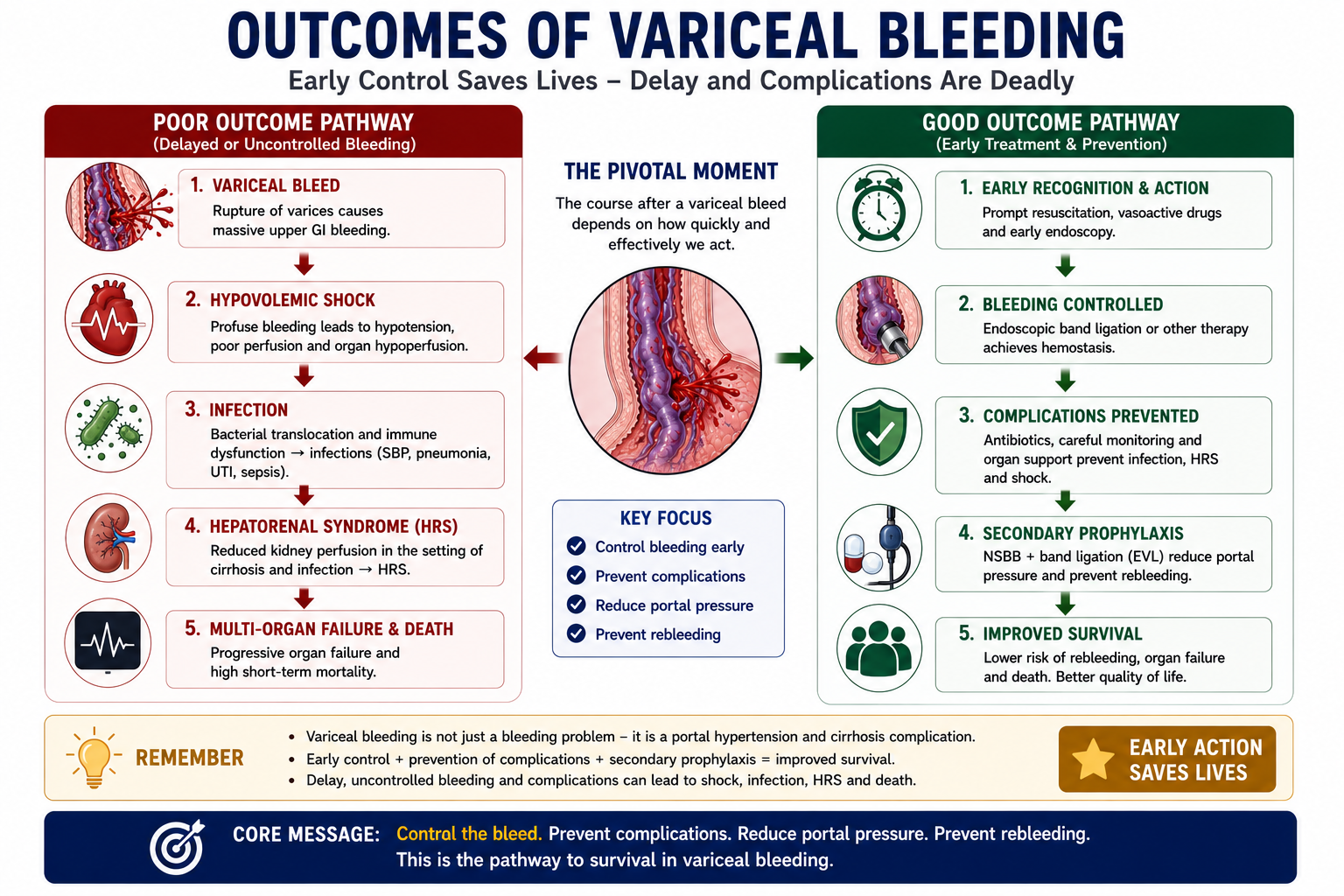
Variceal bleeding, SBP and HRS often interact. GI bleeding precipitates bacterial infection — which is why antibiotic prophylaxis is mandatory. Infection and haemorrhage together worsen circulatory dysfunction and increase the risk of hepatorenal syndrome. This interconnection explains why managing cirrhosis requires attention to all complications simultaneously.
One-Minute Variceal Bleeding Revision
High-Yield Exam Pearls
Varices = portosystemic collaterals
Most common site = distal esophagus (left gastric → azygos)
Varices form because portal blood bypasses the cirrhotic liver
Large varices bleed more — wall tension increases with radius
Red wale marks = high rupture risk
OGD = diagnostic AND therapeutic
Band ligation = first-line for esophageal varices
Antibiotics mandatory in all GI bleeding in cirrhosis
Restrictive transfusion — not liberal
Secondary prophylaxis = beta-blocker + band ligation
- Varices are bypass channels — not pathological growths. They form because portal blood is trying to return to the systemic circulation.
- Red wale marks — know what they are, what they predict, and that they are seen on endoscopy.
- Vasoactive drugs before endoscopy — terlipressin or octreotide should be started as soon as variceal bleeding is suspected, before endoscopy.
- Antibiotics are mandatory — all cirrhotic patients with GI bleeding, regardless of clinical signs of infection.
- Restrictive transfusion — target Hb 70–80 g/L. Over-transfusion raises portal pressure and worsens bleeding risk.
- Non-selective beta-blockers — must be non-selective (not cardioselective) to achieve both beta-1 and beta-2 blockade for portal pressure reduction.
- Secondary prophylaxis combines beta-blocker AND band ligation — combination is more effective than either alone.
- Caput medusae — dilated superficial abdominal veins radiating from umbilicus due to paraumbilical vein collaterals.
- HVPG thresholds — >10 mmHg = clinically significant portal hypertension; >12 mmHg = variceal bleeding risk rises.
- TIPS treats portal pressure — it is used when bleeding is uncontrolled or recurrent despite standard therapy.
- Risk of first bleed is highest with large varices, red wale marks and advanced liver disease.
Key Takeaways
- Variceal bleeding is the bleeding complication of portal hypertension, not a separate disease
- Varices are portosystemic collaterals — bypass channels that form when the cirrhotic liver obstructs portal flow
- Most important site is the distal esophagus via the left gastric–azygos connection
- Varices rupture when wall tension exceeds wall strength — large varices at highest risk (Laplace's law)
- Red wale marks on endoscopy predict high imminent rupture risk
- Clinically significant portal hypertension begins around HVPG >10 mmHg; bleeding risk rises especially above HVPG >12 mmHg
- Risk factors for first bleed include large varices, red wale marks, high portal pressure and advanced cirrhosis
- If bleeding cannot be controlled with standard therapy, rescue options include repeat endoscopy, temporary tamponade/stent and TIPS
- TIPS reduces variceal bleeding by treating the pressure problem — portal hypertension
- Acute management: resuscitate, give vasoactive drug, give antibiotics, perform urgent endoscopy with band ligation
- Restrictive transfusion strategy — target Hb 70–80 g/L to avoid raising portal pressure
- Band ligation strangulates varices, stops blood flow, and causes thrombosis and fibrosis
- Primary prophylaxis prevents the first bleed; secondary prophylaxis prevents rebleeding
- Secondary prophylaxis = non-selective beta-blocker combined with band ligation sessions
- Variceal bleeding precipitates infection and can trigger hepatorenal syndrome
- Prognosis depends on severity of liver disease, haemodynamic status, and early rebleeding
Frequently Asked Questions
References
- de Franchis R; Baveno VI Faculty. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop. J Hepatol. 2015;63(3):743–752.
- Garcia-Tsao G, Sanyal AJ, Grace ND, Carey W; Practice Guidelines Committee of the American Association for the Study of Liver Diseases. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. 2007;46(3):922–938.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460.
- Bosch J, Abraldes JG, Berzigotti A, Garcia-Tsao G. The clinical use of HVPG measurements in chronic liver disease. Nat Rev Gastroenterol Hepatol. 2009;6(10):573–582.
- Tripathi D, Stanley AJ, Hayes PC, et al. UK guidelines on the management of variceal haemorrhage in cirrhotic patients. Gut. 2015;64(11):1680–1704.
- Lo GH, Lai KH, Cheng JS, et al. A prospective, randomized trial of butyl cyanoacrylate injection versus band ligation in the management of bleeding gastric varices. Hepatology. 2001;33(5):1060–1064.
- Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med. 2013;368(1):11–21.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist hepatological input when managing patients with variceal bleeding.
- What Is Variceal Bleeding?
- Why Do Varices Form?
- Collateral Sites
- Esophageal vs Gastric
- Why Varices Rupture
- Risk Factors for First Bleed
- Clinical Presentation
- Diagnosis
- Acute Management
- Band Ligation
- Rescue Therapy / TIPS
- Primary vs Secondary Prophylaxis
- Prognosis
- Exam Pearls
- One-Minute Revision
- Key Takeaways
- FAQ
- References