Most students think HCC simply means liver cancer.
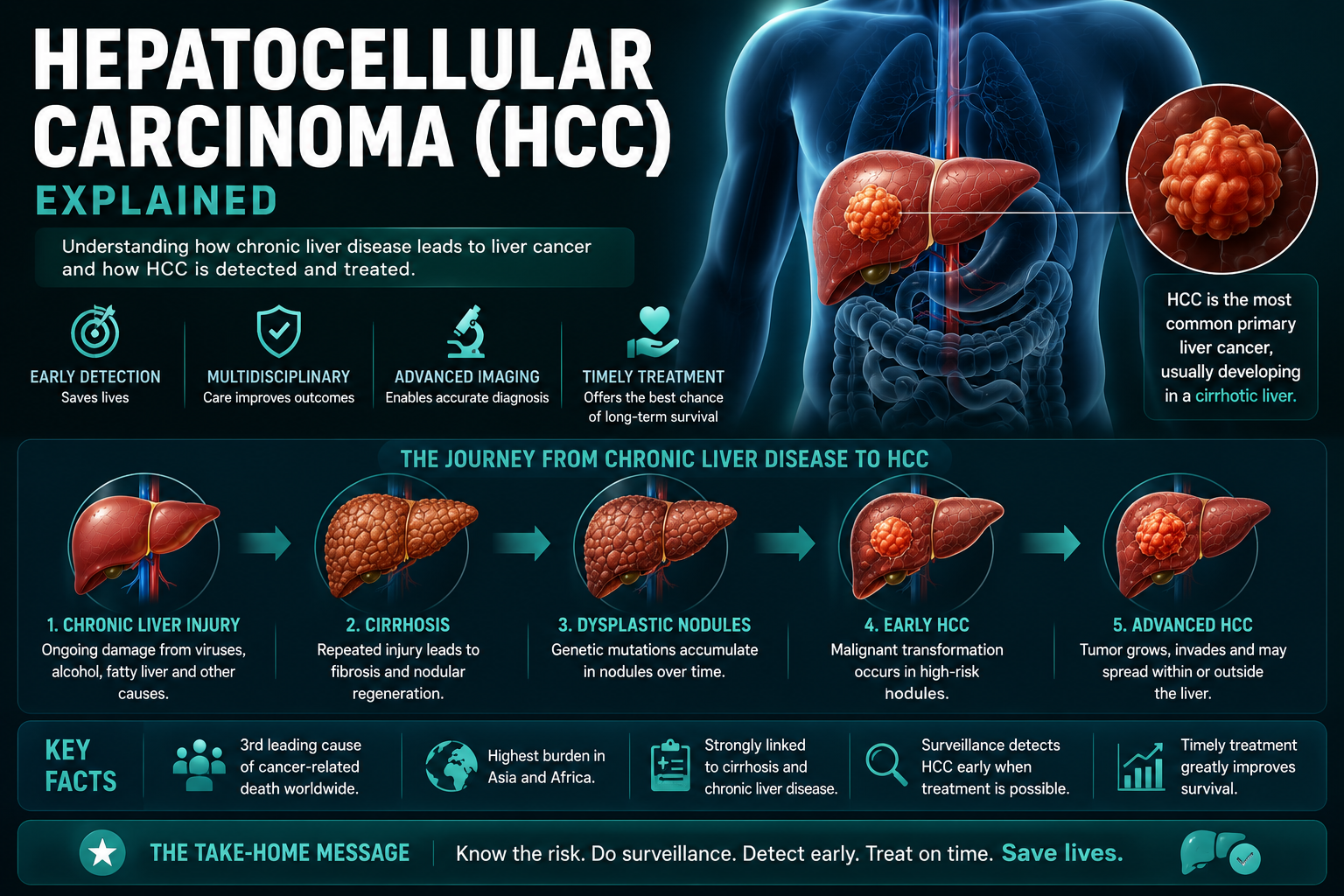
The better concept is: chronic liver injury creates repeated cell death and regeneration. Over time, genetic mutations accumulate and a malignant hepatocyte clone can develop into hepatocellular carcinoma.
HCC is best understood as cancer arising in a chronically injured and regenerating liver.
Learning Objectives
- Define hepatocellular carcinoma
- Explain why cirrhosis causes HCC
- Identify major hepatocellular carcinoma causes and risk factors
- Understand HCC surveillance and the AFP liver cancer test
- Recognize arterial enhancement and washout on multiphasic imaging
- Understand LI-RADS classification, BCLC staging system and major treatment options
What Is Hepatocellular Carcinoma?
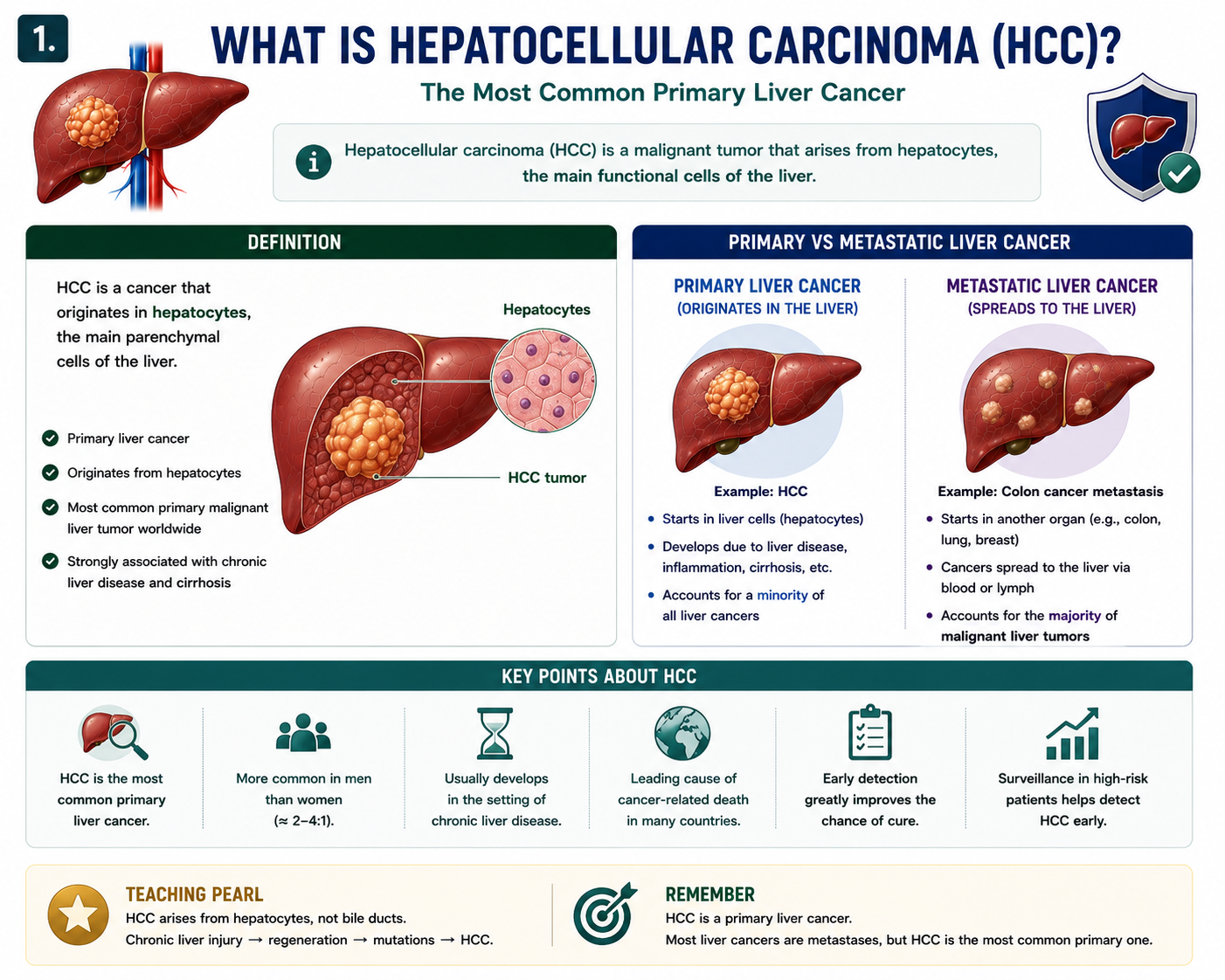
Hepatocellular carcinoma is a malignant tumor arising from hepatocytes. It is the most common primary liver cancer worldwide.
Primary liver cancer begins in the liver. Liver metastases are cancers that started elsewhere and spread to the liver. That distinction matters because the diagnostic pathway and treatment strategy are very different.
Most malignant tumors found in the liver are metastases, but HCC is the most common primary liver cancer.
HCC vs Cholangiocarcinoma
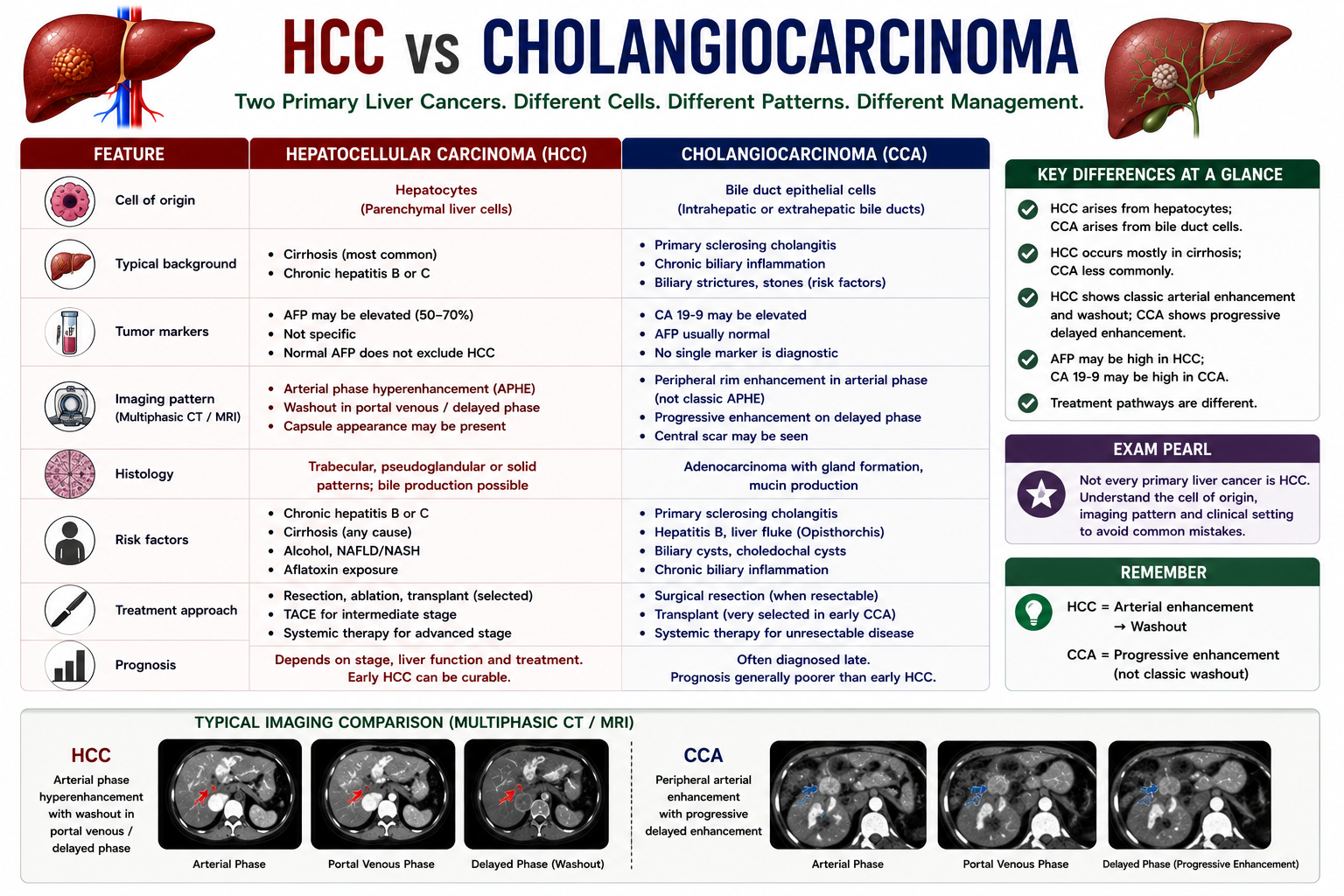
HCC and cholangiocarcinoma are both primary liver cancers, but they arise from different cells and behave differently.
| Feature | Hepatocellular Carcinoma | Cholangiocarcinoma |
|---|---|---|
| Cell of origin | Hepatocytes | Bile duct epithelial cells |
| Typical background | Cirrhosis or chronic hepatitis | Primary sclerosing cholangitis, biliary disease or chronic biliary inflammation |
| AFP | May be elevated | Usually not the main marker |
| Imaging pattern | Arterial enhancement followed by washout is classic | Often shows progressive delayed enhancement rather than classic HCC washout |
| Treatment pathway | Resection, ablation, transplant, TACE or systemic therapy depending on stage | Surgical resection when possible; transplant only in highly selected protocols |
HCC arises from hepatocytes. Cholangiocarcinoma arises from bile duct epithelium. Do not call every primary liver cancer HCC.
Why Does Cirrhosis Cause HCC?
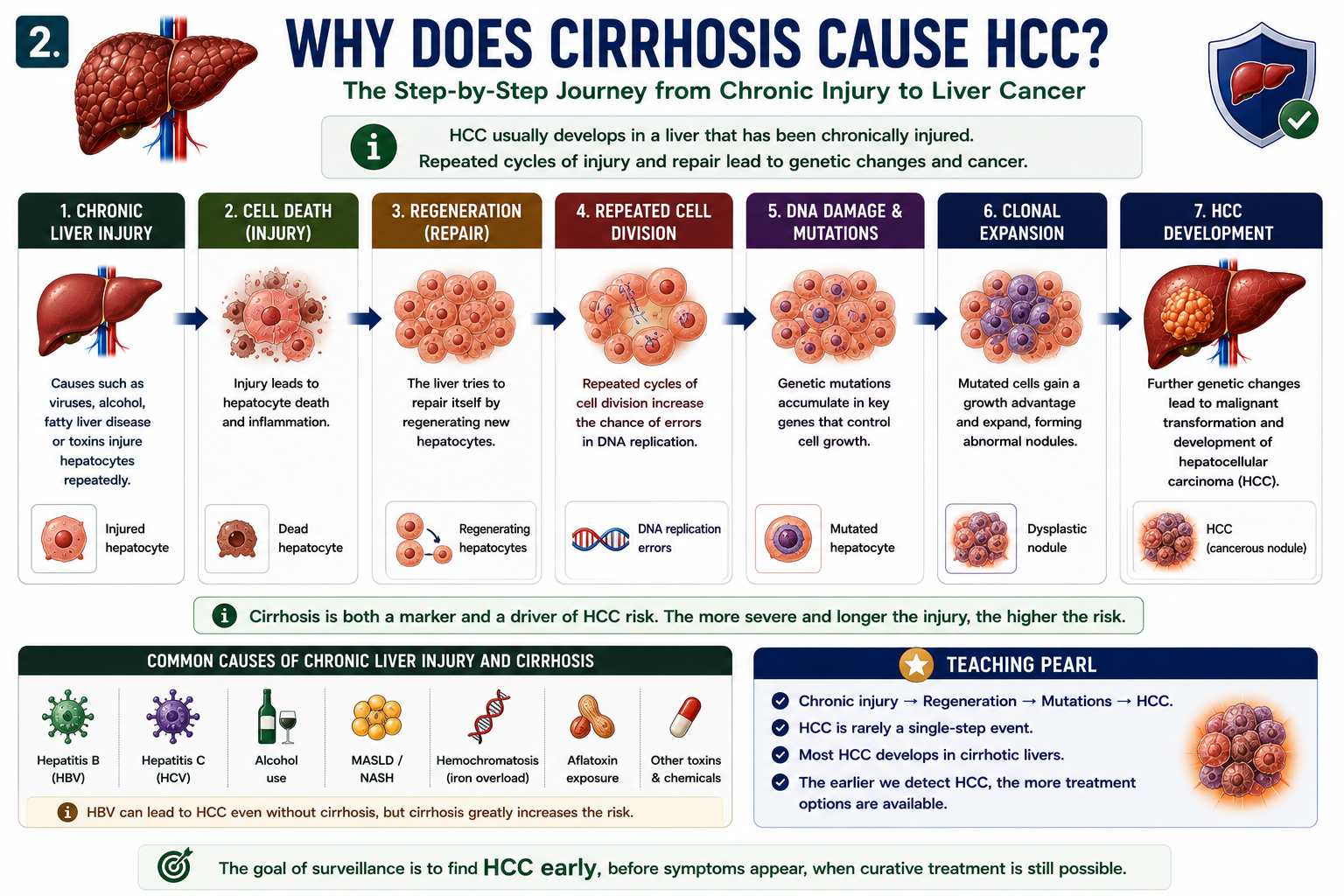
Cirrhosis creates a pro-cancer environment: inflammation, cell death, fibrosis, oxidative stress and repeated regeneration all increase the chance that mutations will accumulate.
Common background diseases include hepatitis B, hepatitis C, alcohol-related liver disease, MASLD/NASH and hemochromatosis. This is why HCC sits naturally after cirrhosis, portal hypertension and decompensation in the hepatology learning chain.
For cluster context, review Portal Hypertension Explained, Ascites Explained and Liver Transplantation Explained.
Most HCC develops in cirrhotic livers, but hepatitis B can occasionally cause HCC before cirrhosis develops.
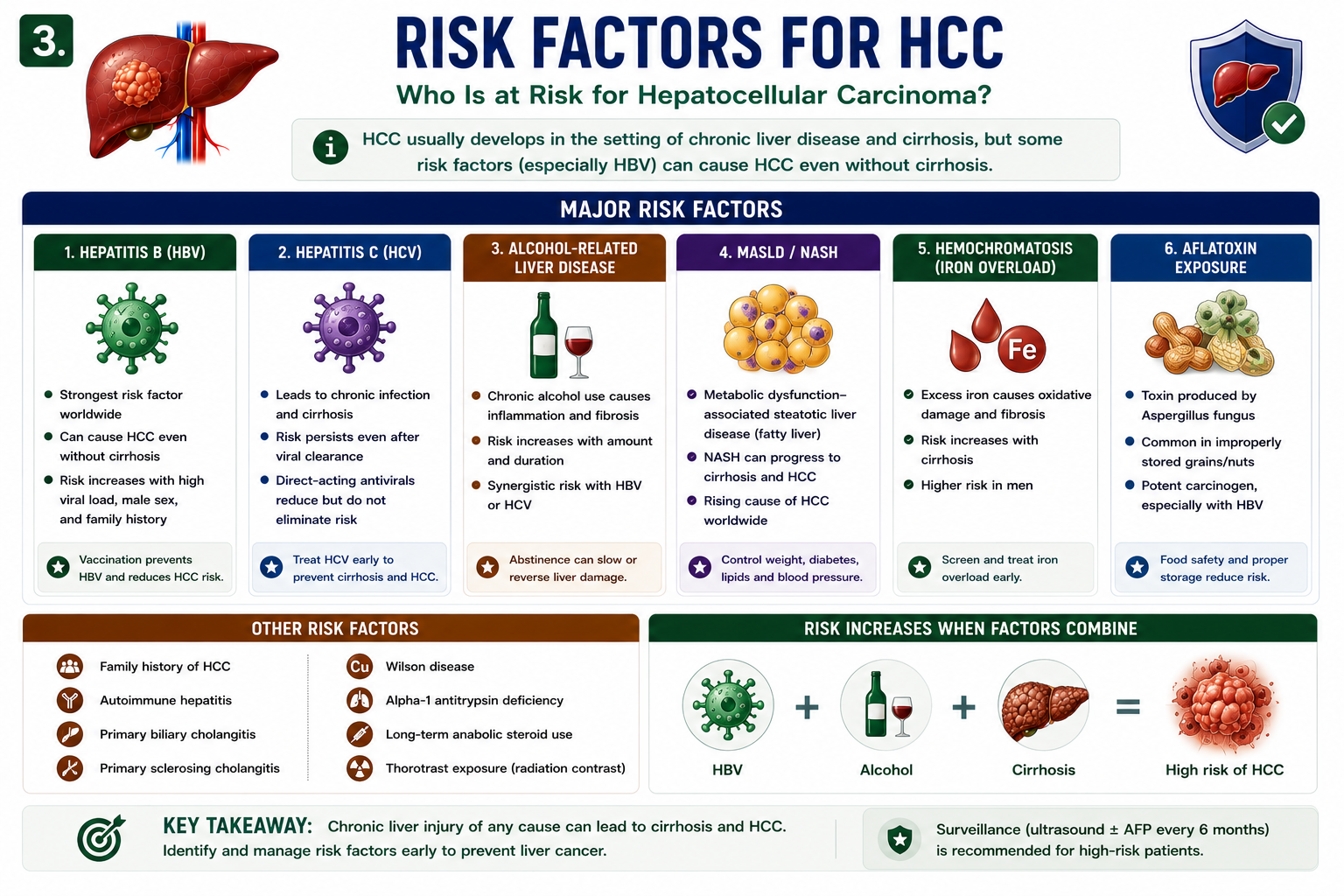
Risk Factors for HCC
The main hepatocellular carcinoma causes are conditions that chronically injure hepatocytes or increase genetic damage.
| Risk Factor | Mechanism |
|---|---|
| HBV | Chronic inflammation and viral effects; can cause HCC without established cirrhosis |
| HCV | Progressive fibrosis, cirrhosis and chronic inflammation |
| Alcohol | Chronic liver injury, cirrhosis and oxidative stress |
| MASLD/NASH | Metabolic inflammation, fibrosis and cirrhosis |
| Hemochromatosis | Iron-mediated oxidative injury |
| Aflatoxin | Direct DNA mutation risk, especially with HBV co-exposure |
HBV is the classic exception: it may cause HCC even before cirrhosis is present.
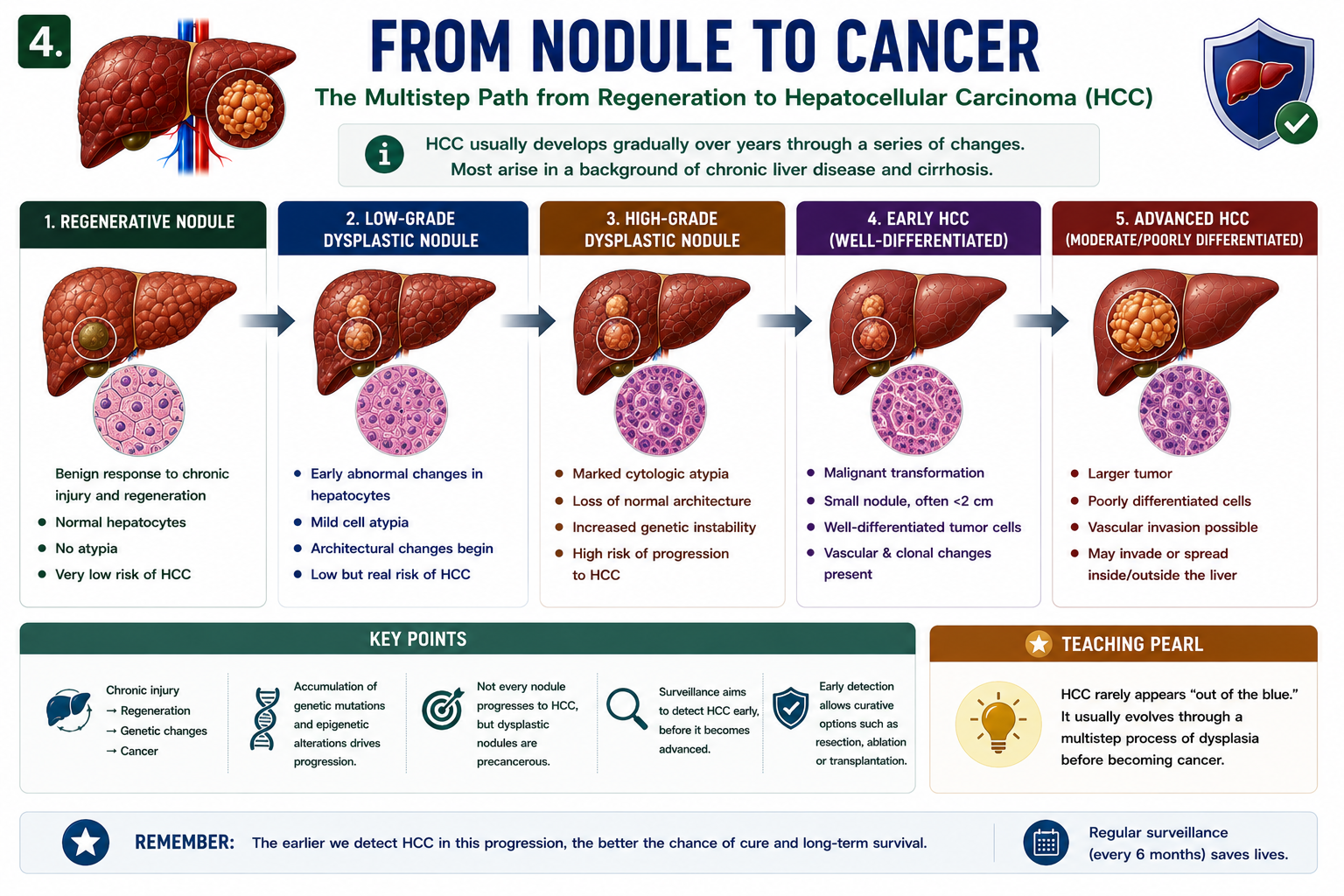
From Regenerative Nodule to HCC
HCC usually develops through a multistep sequence rather than appearing suddenly. In a cirrhotic liver, nodules can gradually acquire dysplastic and malignant features.
This explains why surveillance matters. The goal is to find a small early tumor while curative treatment is still possible.
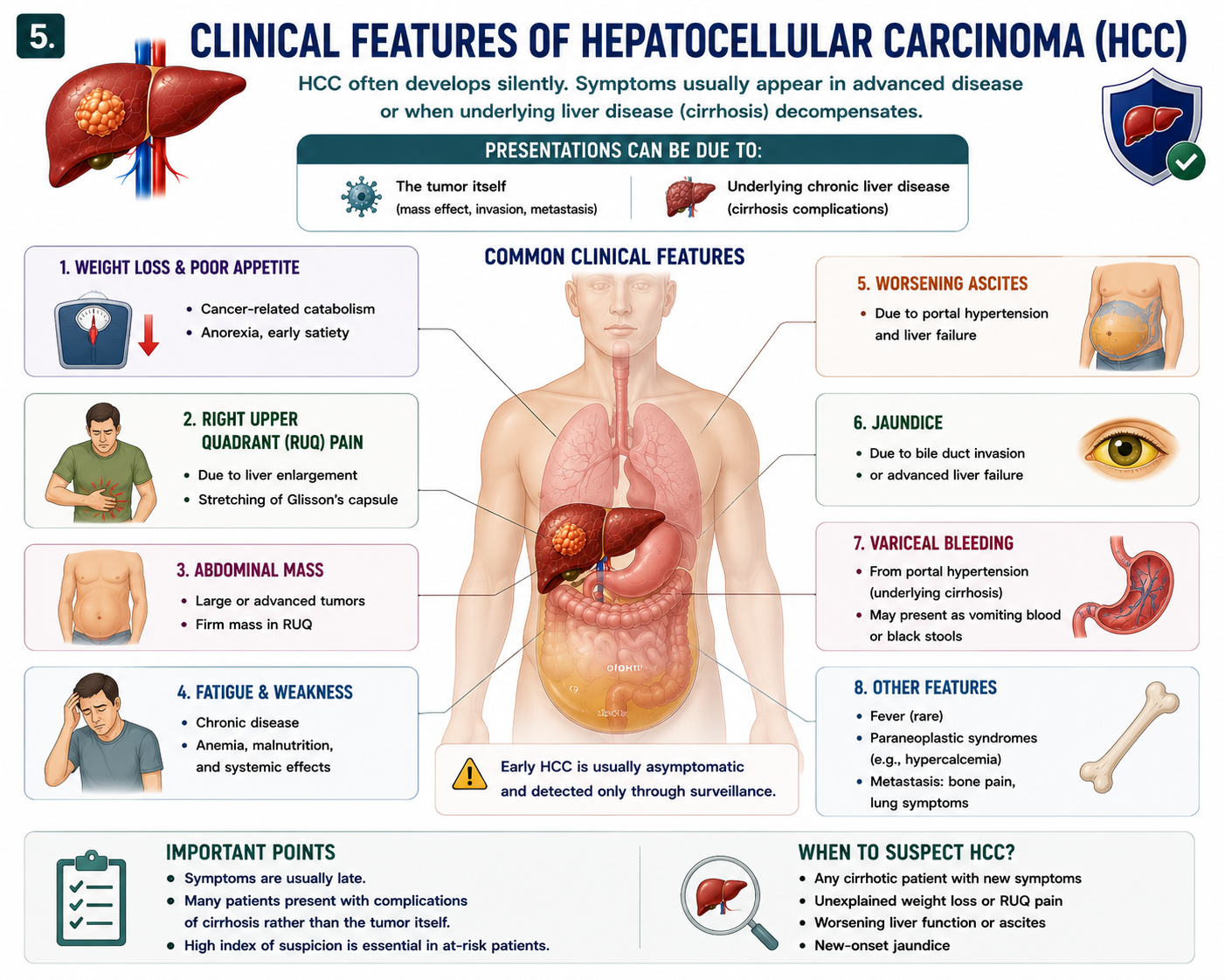
Clinical Features of HCC
Early HCC is often asymptomatic. By the time obvious hepatocellular carcinoma symptoms appear, disease may be more advanced or the underlying cirrhosis may have decompensated.
| Symptom or Sign | Explanation |
|---|---|
| Weight loss | Systemic cancer effect |
| Right upper quadrant pain | Tumor enlargement or capsular stretch |
| Abdominal mass | Large tumor burden |
| Worsening ascites | Cirrhosis decompensation or portal vein involvement |
| Jaundice | Advanced tumor, liver failure or biliary involvement |
| Variceal bleeding | Underlying portal hypertension |
Because symptoms are late, surveillance is the key tool for early detection in high-risk groups.
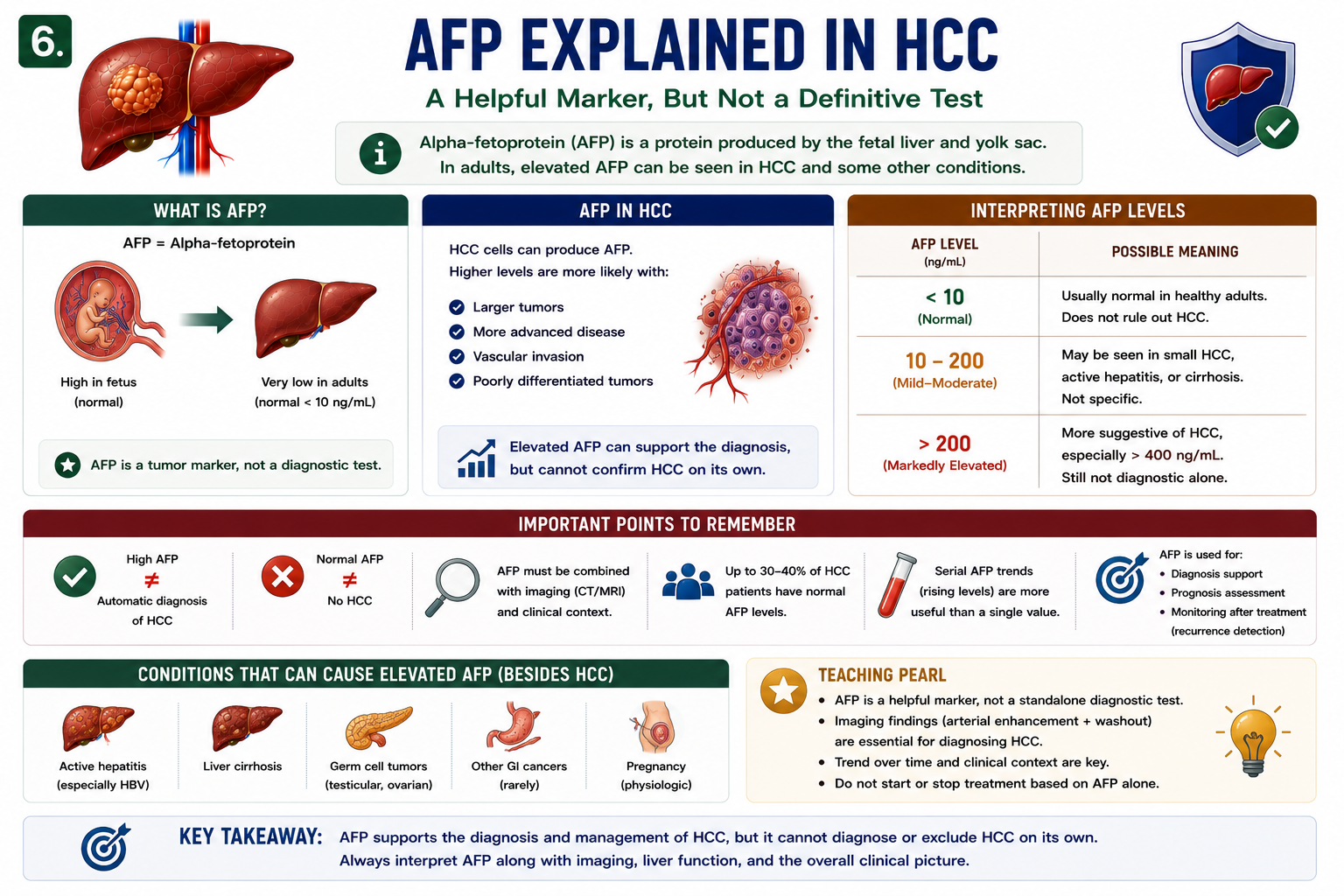
AFP Explained
AFP means alpha-fetoprotein. Some HCC tumors produce AFP, so AFP may rise in the blood.
The key teaching point is that the AFP liver cancer test is supportive, not definitive. High AFP does not automatically diagnose HCC, and normal AFP does not exclude HCC.
AFP alone cannot confirm or exclude HCC. Imaging pattern and clinical context are central to hepatocellular carcinoma diagnosis.
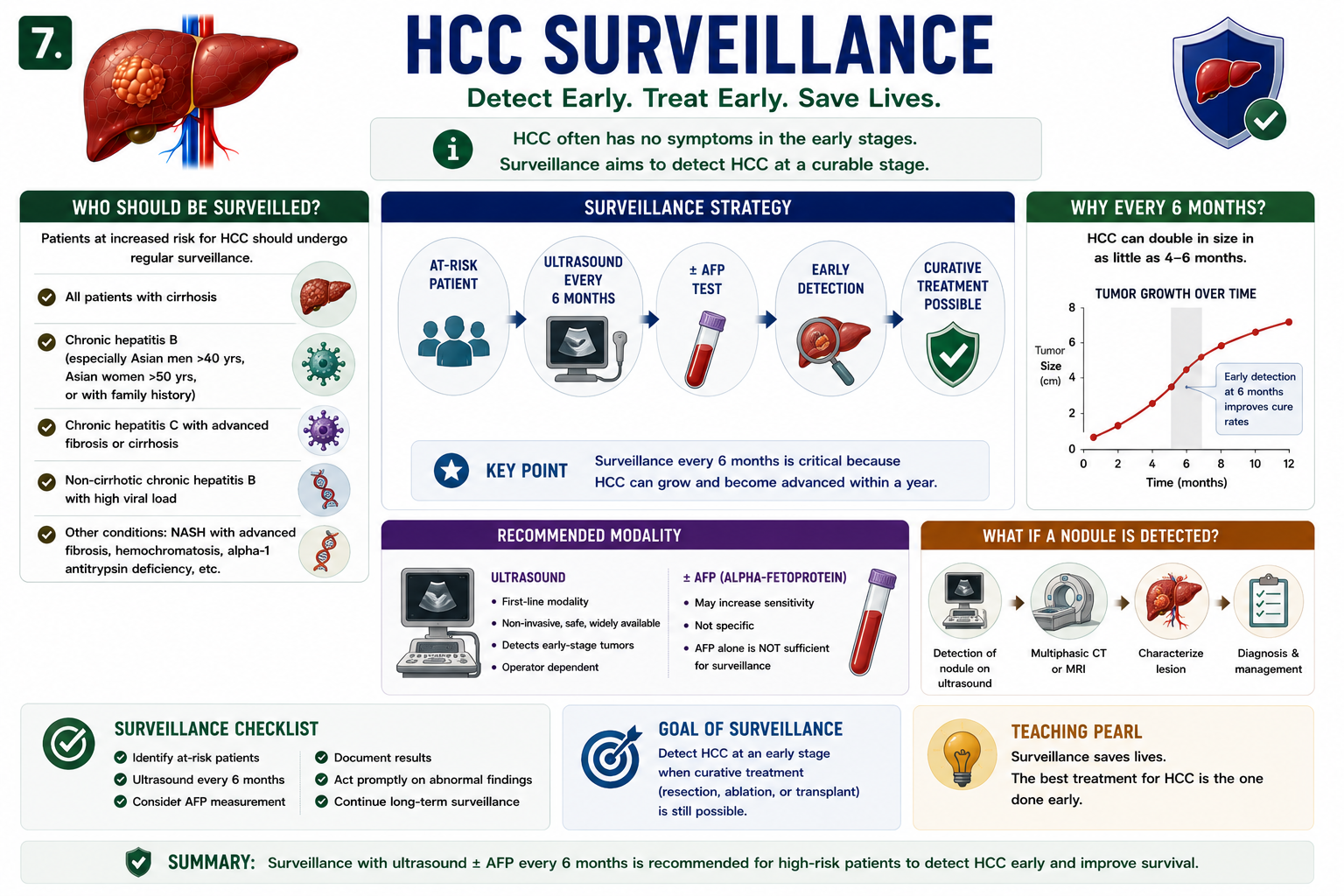
HCC Surveillance
HCC surveillance aims to detect cancer before symptoms develop. In many guidelines, patients with cirrhosis who are candidates for HCC treatment undergo ultrasound every 6 months, with or without AFP.
Students often search for HCC surveillance guidelines as a list of rules. The practical concept is simpler: surveillance only helps if the patient is at meaningful risk and could benefit from treatment if early HCC is found.
In patient-facing language, HCC surveillance is often described as liver cancer screening, but in medical education the term surveillance is more precise for high-risk groups.
Surveillance is not diagnosis. It is an early-warning system that triggers proper diagnostic imaging when a concerning lesion is found.
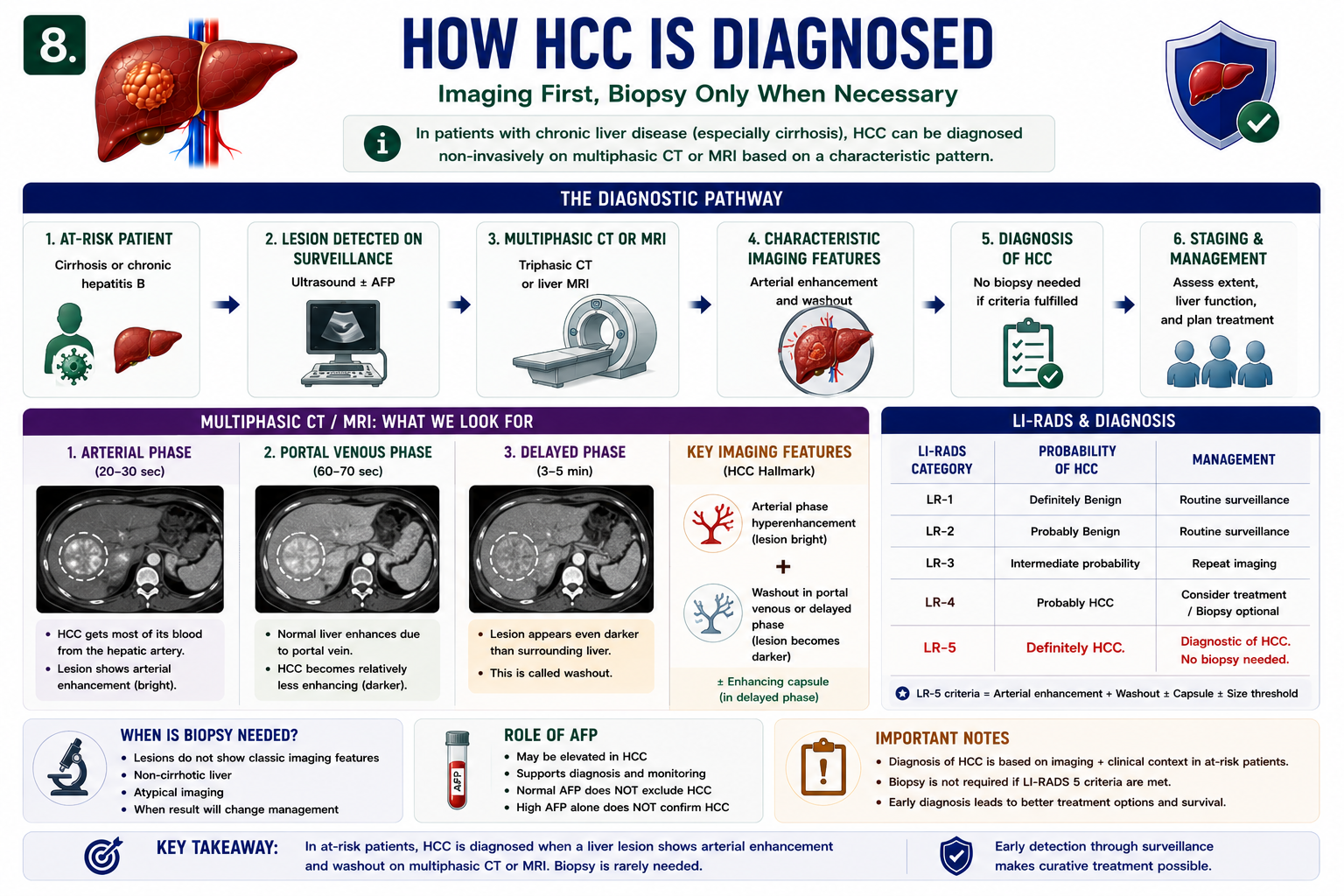
How HCC Is Diagnosed
Hepatocellular carcinoma diagnosis usually starts when surveillance detects a lesion or when symptoms prompt imaging. A lesion larger than 1 cm in an at-risk patient is commonly evaluated with multiphasic CT or MRI.
Multiphasic imaging captures the liver during arterial, portal venous and delayed phases. HCC has a characteristic blood supply shift, and that shift creates the classic imaging appearance.
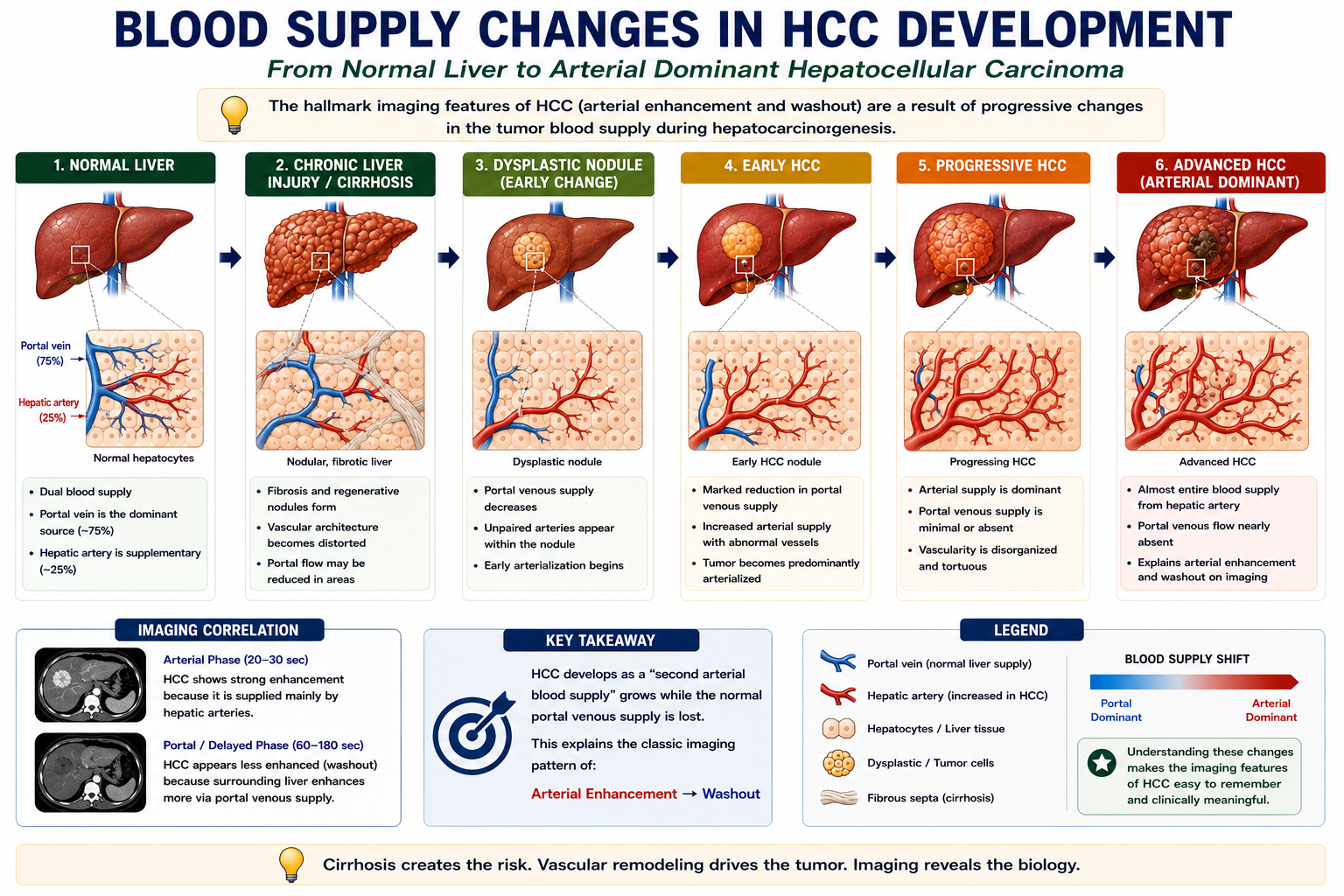
Tumor Blood Supply Changes During HCC Development
The imaging appearance of HCC is easiest to understand if you first understand how the blood supply changes during cancer development.
Normal liver tissue receives most of its blood from the portal vein. As a dysplastic nodule becomes HCC, portal venous supply falls and new abnormal arterial vessels develop. This process is called arterialization.
HCC becomes bright in the arterial phase because it is supplied mainly by arteries. It washes out later because the surrounding liver enhances more during the portal venous and delayed phases.
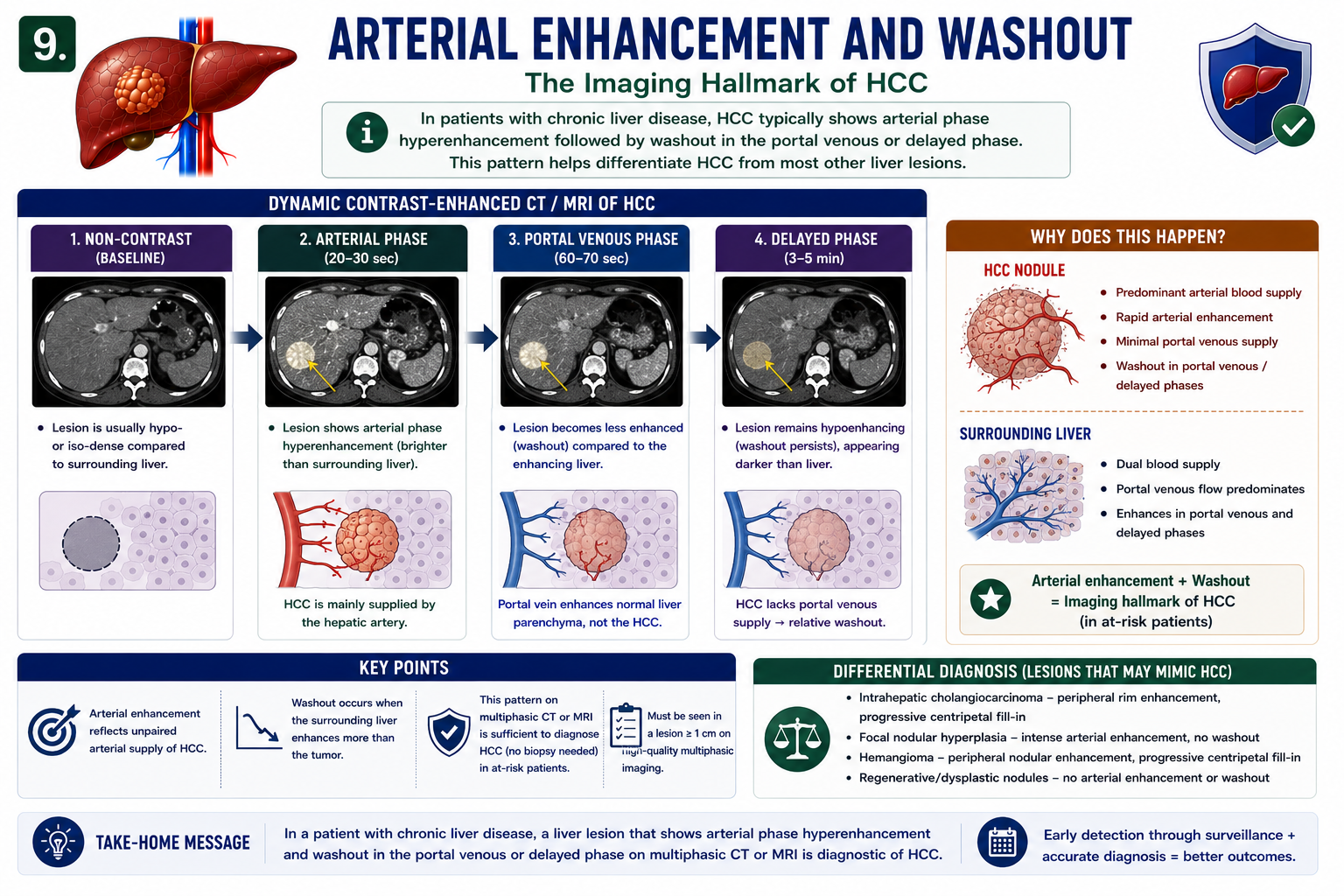
Arterial Enhancement and Washout
Normal liver receives most blood from the portal vein. HCC increasingly relies on arterial blood supply. That difference explains arterial enhancement and washout.
The phrase arterial enhancement washout means the lesion enhances more than liver during the arterial phase, then becomes relatively less enhanced than liver later. This is the classic imaging signature of HCC in the correct clinical setting.
HCC behaves like an arterialized tumor sitting inside a portal-venous liver. That vascular mismatch creates the bright-then-dark pattern.
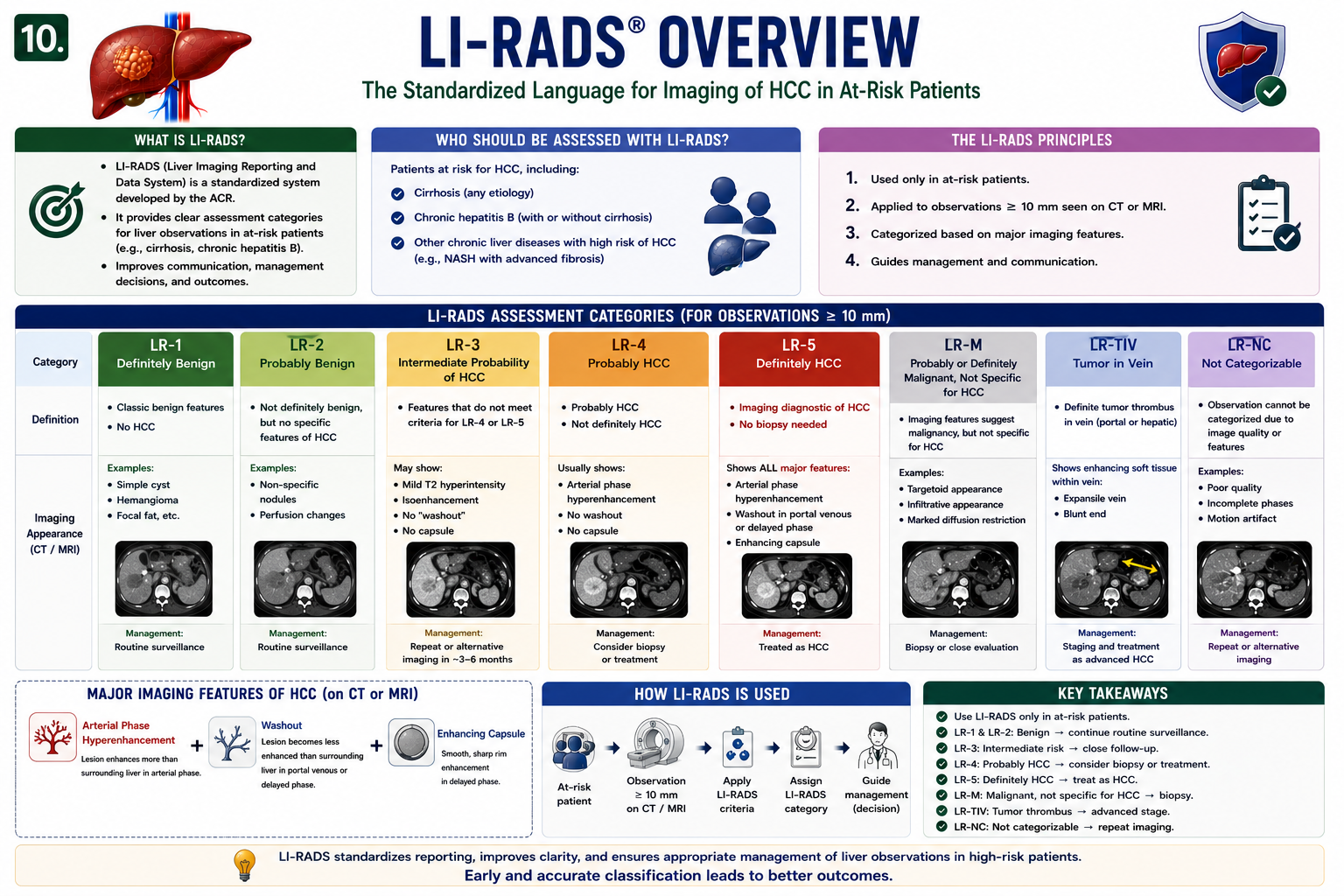
LI-RADS Explained
LI-RADS classification standardizes how radiologists describe liver observations in patients at risk for HCC. It helps clinicians communicate probability of malignancy consistently.
| Category | Meaning |
|---|---|
| LR-1 | Definitely benign |
| LR-2 | Probably benign |
| LR-3 | Intermediate probability |
| LR-4 | Probably HCC |
| LR-5 | Definitely HCC |
At student level, LI-RADS explained means this: the closer the lesion gets to LR-5, the more confidently the imaging features fit HCC.
LR-5 lesions are considered diagnostic of HCC on imaging in the appropriate at-risk population.
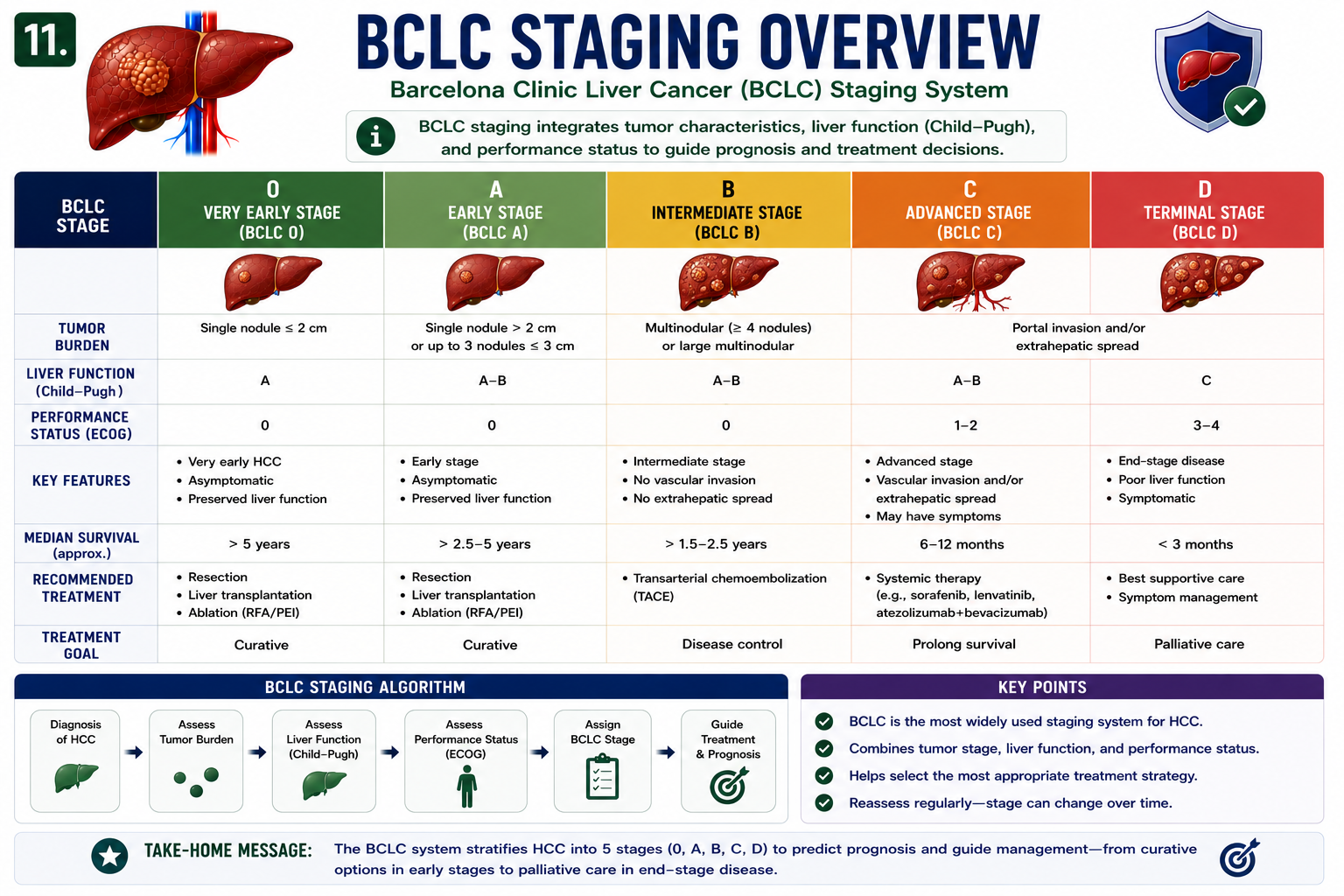
BCLC Staging Overview
The BCLC staging system is widely used because HCC prognosis depends on more than tumor size. The same tumor can mean different things in a patient with well-preserved liver function versus advanced decompensated cirrhosis.
BCLC incorporates tumor burden, liver function and performance status. This matters because treatment selection must protect both oncologic control and remaining liver reserve.
Hepatocellular carcinoma staging is clinically useful only when it links tumor burden with liver function and treatment options.
| BCLC Domain | Why It Matters |
|---|---|
| Tumor burden | Size, number, vascular invasion and extrahepatic spread |
| Liver function | Determines whether resection, ablation, transplant or systemic therapy is safe |
| Performance status | Shows how well the patient can tolerate treatment |
Curative Treatments for HCC
Hepatocellular carcinoma treatment depends on tumor stage, liver function and patient fitness. Selected early tumors can be treated with curative intent.
| Treatment | Typical Use |
|---|---|
| Resection | Solitary tumor with preserved liver function and adequate future liver remnant |
| Ablation | Small tumors, especially when surgery is not ideal |
| Transplant | Selected early HCC with cirrhosis within accepted transplant criteria |
Transplantation is unique because it removes both the tumor and the cirrhotic liver that produced the tumor.

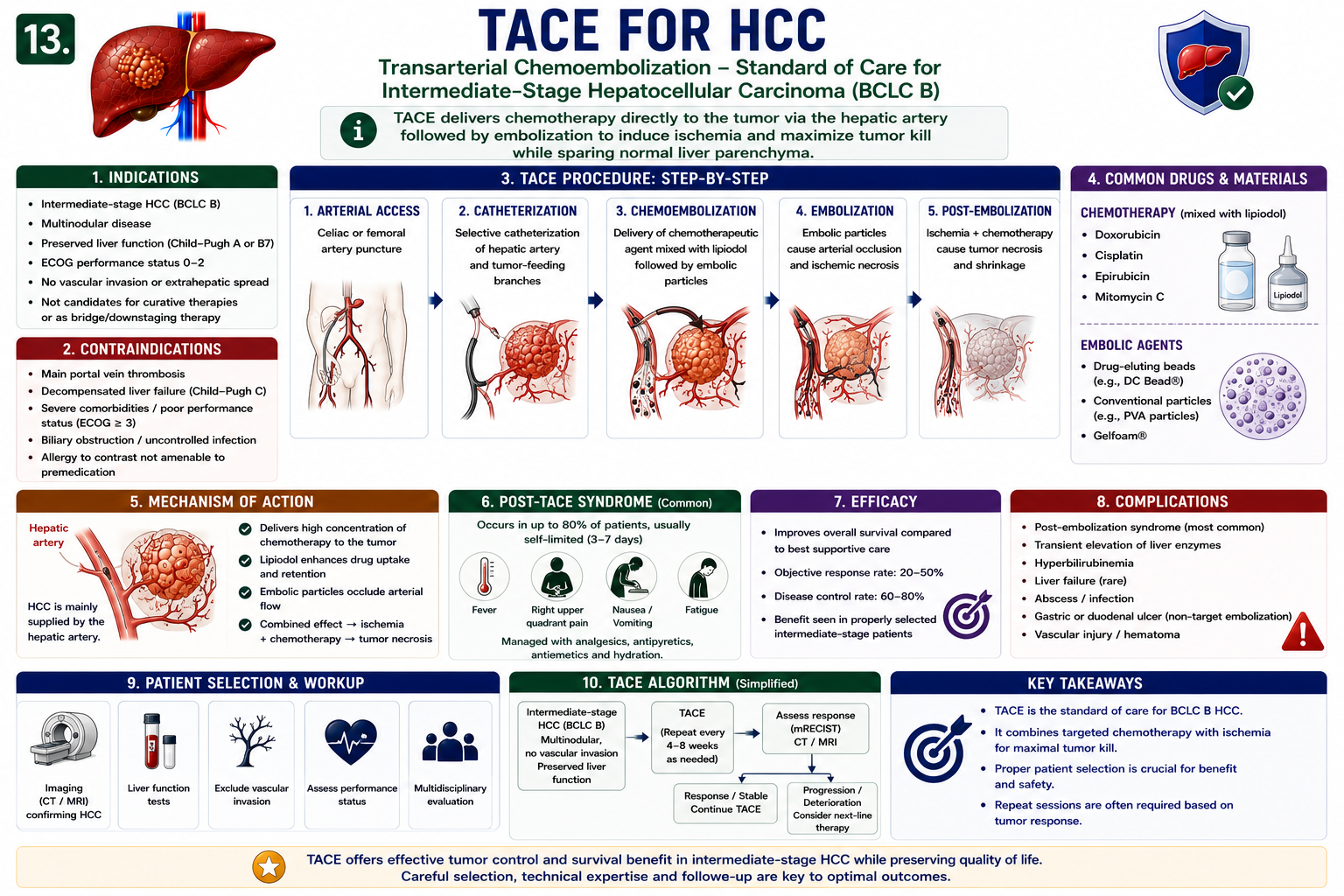
TACE Explained
TACE means transarterial chemoembolization. It uses the arterial blood supply of HCC against the tumor.
TACE liver cancer treatment is usually not curative by itself. It is commonly used to control unresectable intermediate-stage disease, downstage tumor burden or bridge selected patients to transplant.
TACE works because HCC is more arterial than the surrounding liver. Blocking the tumor-feeding artery can starve the tumor while delivering local chemotherapy.
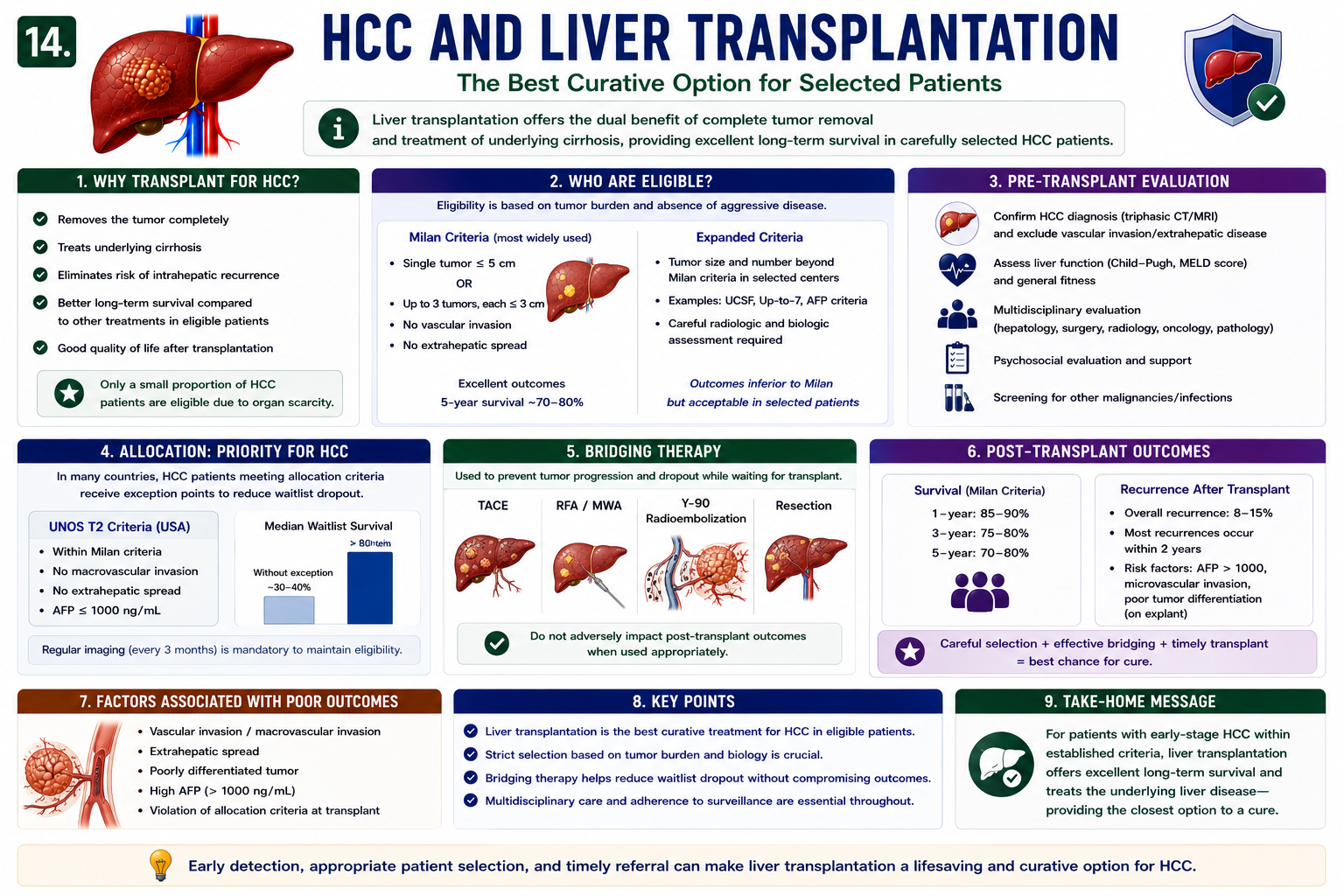
HCC and Liver Transplantation
Liver transplant for HCC is considered when the cancer is early enough and the patient meets transplant criteria. The classic teaching idea is: small tumor burden, no vascular invasion and no spread outside the liver.
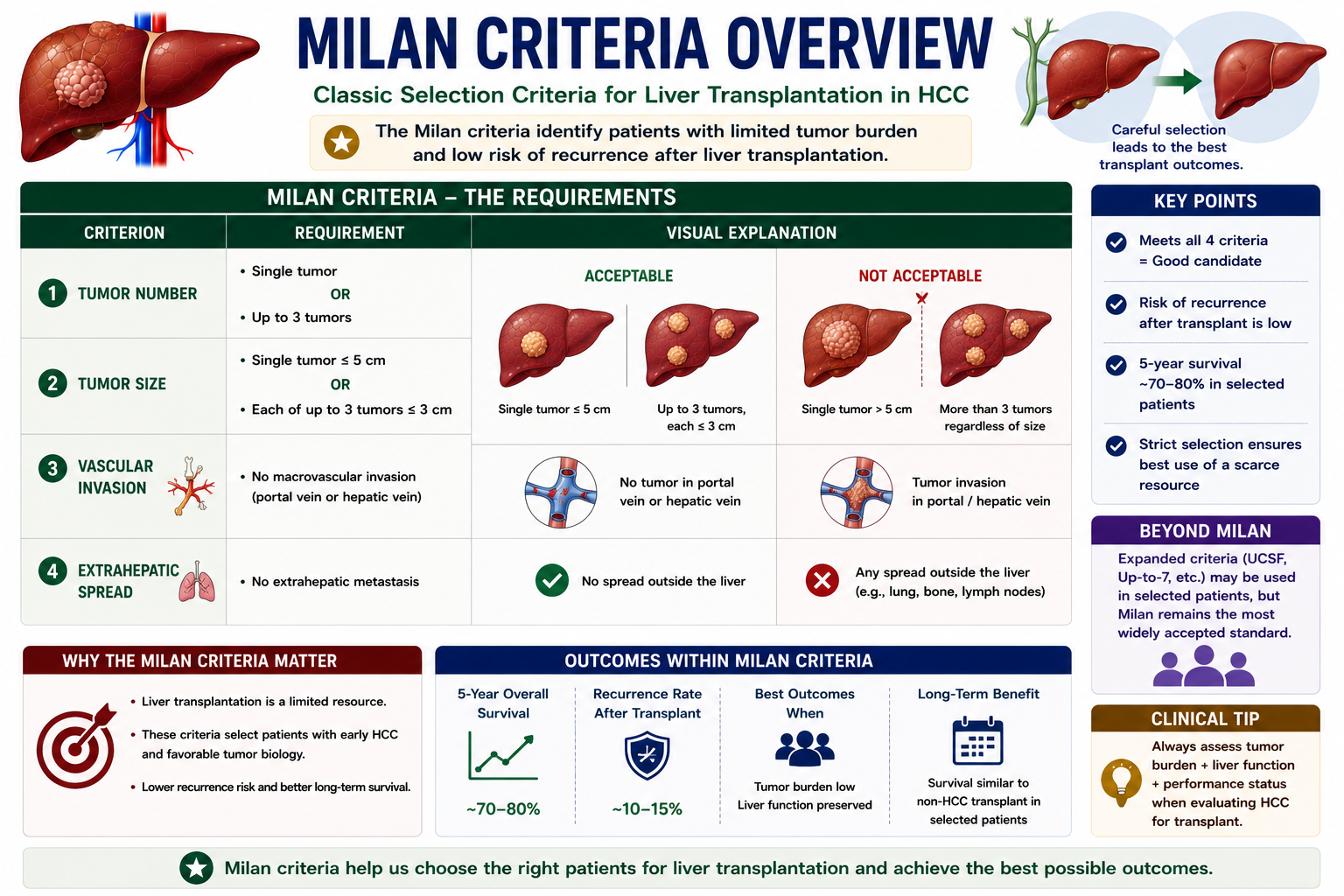
Milan Criteria Overview
The Milan criteria are the classic selection framework for liver transplantation in HCC. They identify patients with limited tumor burden and low risk of recurrence after transplant.
| Criterion | Requirement |
|---|---|
| Single tumor | One lesion ≤ 5 cm |
| Multiple tumors | Up to 3 lesions, each ≤ 3 cm |
| Vascular invasion | Absent |
| Extrahepatic spread | Absent |
The Milan criteria remain the classic framework for selecting HCC patients for liver transplantation. They are important because transplant benefit is highest when tumor biology is favorable and recurrence risk is low.
Liver transplantation is a scarce resource. Selection criteria try to identify patients who are most likely to benefit with low recurrence risk after transplant.
Transplantation can be powerful because it solves two problems at once: the tumor is removed, and the cirrhotic liver that created the cancer risk is removed. See Liver Transplantation Explained for the full transplant pathway.
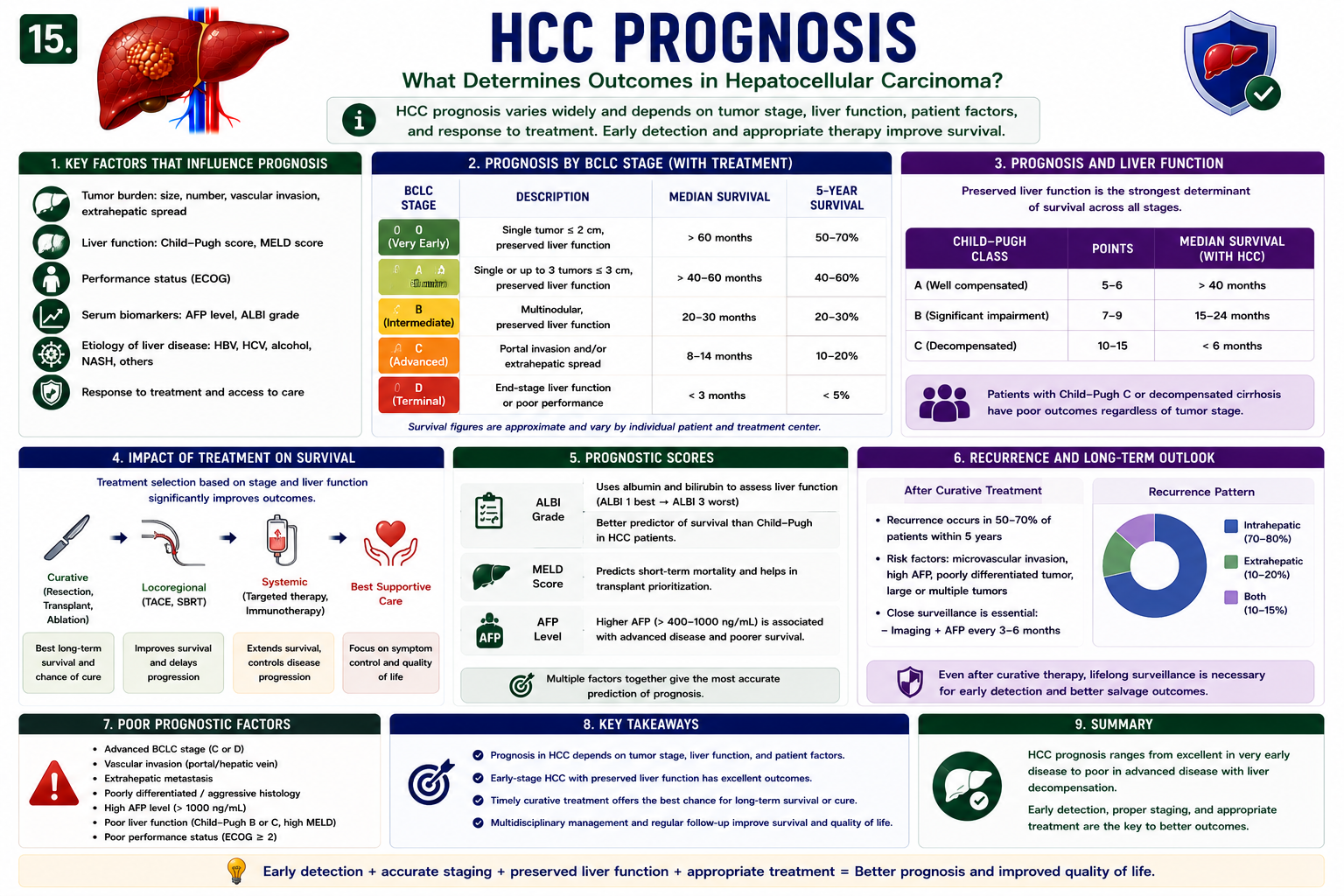
Prognosis
HCC prognosis depends on tumor stage, liver function, performance status, treatment eligibility and response to treatment.
| Better Prognosis | Worse Prognosis |
|---|---|
| Early stage | Advanced stage |
| Curative therapy possible | Untreatable or metastatic disease |
| Preserved liver function | Severe liver failure |
| Small tumor burden | Vascular invasion or extrahepatic spread |
Vascular invasion, extrahepatic spread, advanced BCLC stage, poor liver function, poor performance status, high AFP and poor tumor differentiation are associated with worse outcomes.
Hepatocellular carcinoma prognosis and hepatocellular carcinoma survival depend on tumor stage, liver function, performance status and access to appropriate treatment.
This is why BCLC is useful: it does not stage the tumor in isolation. It asks what the tumor means inside the whole patient.
High-Yield Exam Pearls
- Most HCC develops in cirrhosis.
- HBV can cause HCC without cirrhosis.
- AFP alone cannot diagnose HCC.
- Ultrasound surveillance is commonly performed every 6 months in eligible at-risk patients.
- Arterial enhancement plus washout suggests HCC in the correct clinical setting.
- LI-RADS LR-5 is diagnostic of HCC in an at-risk population.
- Transplantation removes both tumor and cirrhotic liver.
- TACE is usually disease-control or bridge therapy, not definitive cure.
- BCLC staging guides treatment by combining tumor burden, liver function and performance status.
Frequently Asked Questions
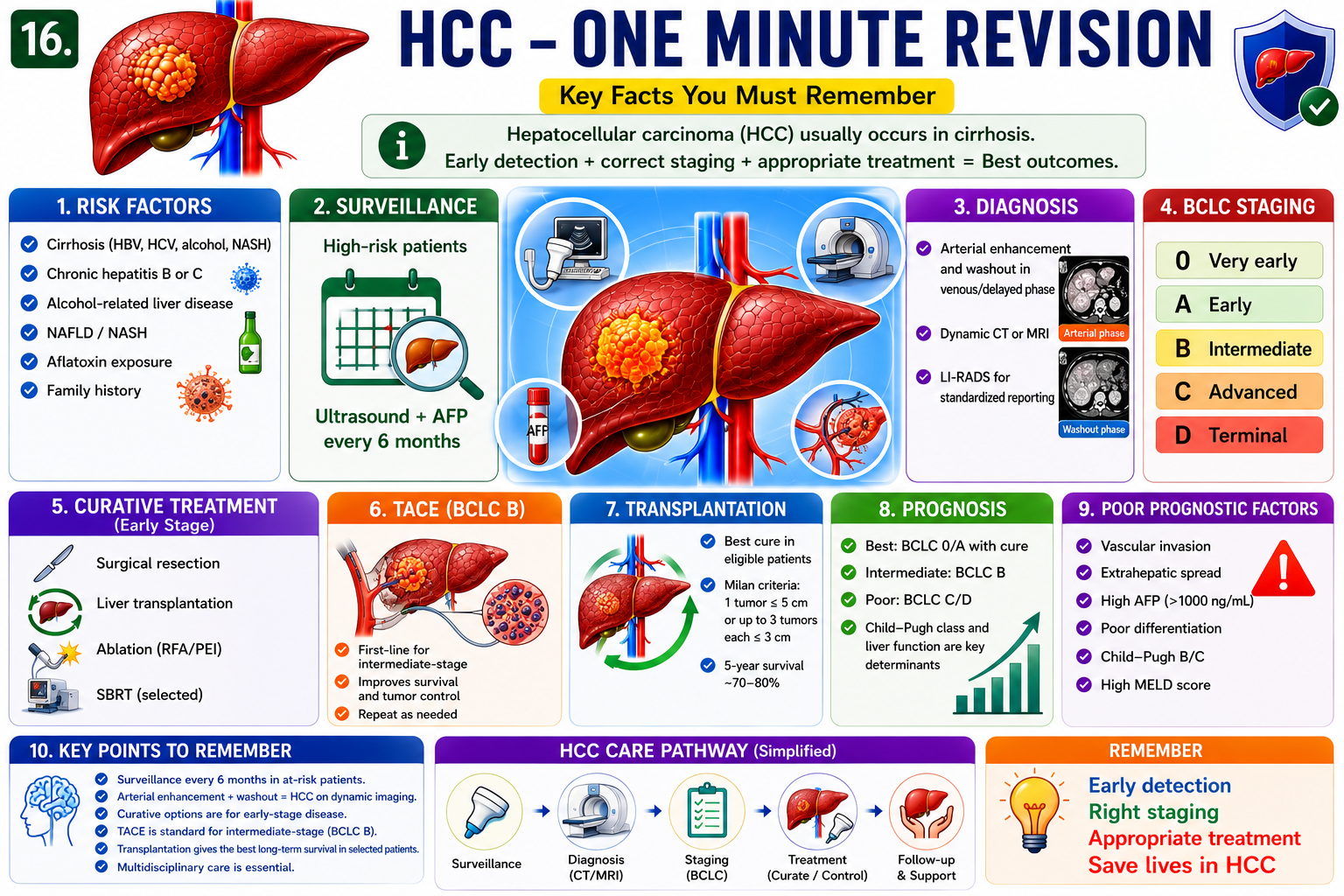
One-Minute Revision
If you remember one pathway, remember this: chronic liver injury creates HCC risk, surveillance finds early lesions, multiphasic imaging confirms the pattern, staging chooses treatment, and transplant may cure selected early HCC by removing both tumor and diseased liver.
Key Takeaways
- HCC is the most common primary liver cancer and usually arises in chronic liver disease.
- Cirrhosis increases risk through repeated injury, regeneration and mutation accumulation.
- AFP supports assessment but cannot diagnose or exclude HCC alone.
- Surveillance aims to detect asymptomatic early HCC before curative options are lost.
- The classic imaging pattern is arterial enhancement followed by washout.
- LI-RADS standardizes radiology language; LR-5 means definitely HCC in the right population.
- Treatment ranges from resection, ablation and transplant to TACE and systemic therapy depending on stage.
Hepatocellular carcinoma is best understood as cancer arising from chronically injured and regenerating hepatocytes. Cirrhosis creates the risk, surveillance detects early tumors, multiphasic imaging identifies arterial enhancement and washout, LI-RADS standardizes diagnosis, BCLC links stage to treatment, and selected early HCC may be cured by resection, ablation or transplantation.
References
- Singal AG, Llovet JM, Yarchoan M, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922-1965.
- National Cancer Institute. Primary Liver Cancer Treatment (PDQ): Health Professional Version. Updated 2025.
- American College of Radiology. Liver Imaging Reporting and Data System (LI-RADS).
- Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J Hepatol. 2022;76(3):681-693.
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334(11):693-699.
This article is intended for medical education only. It does not constitute clinical advice. HCC diagnosis and treatment require specialist hepatology, radiology, oncology, interventional radiology, transplant surgery and multidisciplinary tumor-board assessment.
- What Is HCC?
- HCC vs Cholangiocarcinoma
- Cirrhosis to HCC
- Risk Factors
- Nodule Progression
- Clinical Features
- AFP
- Surveillance
- Diagnosis
- Blood Supply Changes
- Enhancement + Washout
- LI-RADS
- BCLC Staging
- Curative Treatment
- TACE
- HCC and Transplant
- Prognosis
- Exam Pearls
- FAQ
- One-Minute Revision
- Key Takeaways
- References