Most students think liver transplant simply means replacing the liver.
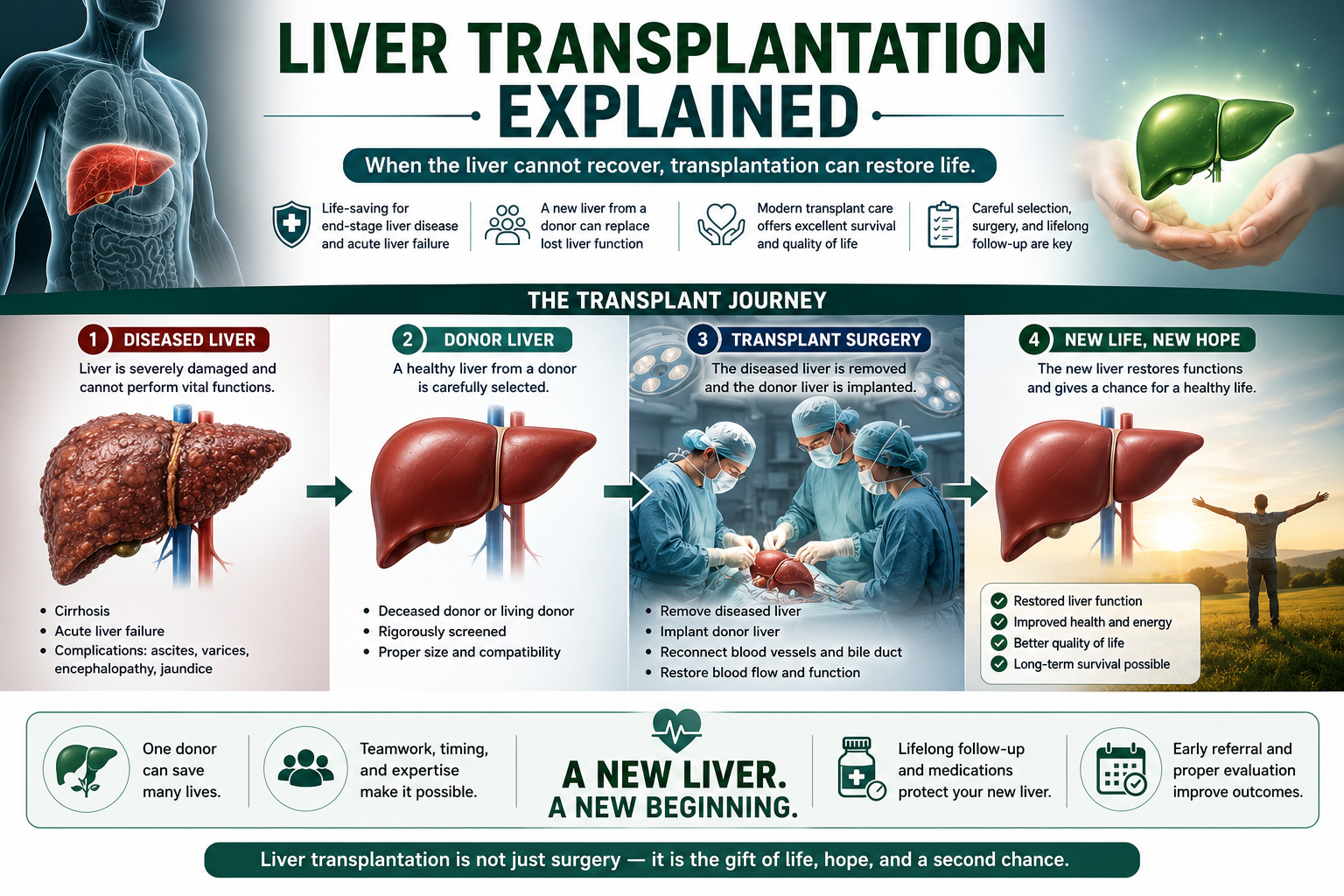
The better concept is functional rescue: irreversible liver failure means the native liver can no longer sustain life, so a healthy donor liver replaces the failing organ and restores essential liver functions.
Transplantation replaces liver function, not simply liver tissue.
Learning Objectives
- Define liver transplantation
- Explain major transplant indications
- Understand MELD score and organ allocation
- Describe donor liver sources and the basic surgical concept
- Explain rejection and immunosuppression
- Recognize complications and long-term outcomes
What Is Liver Transplantation?
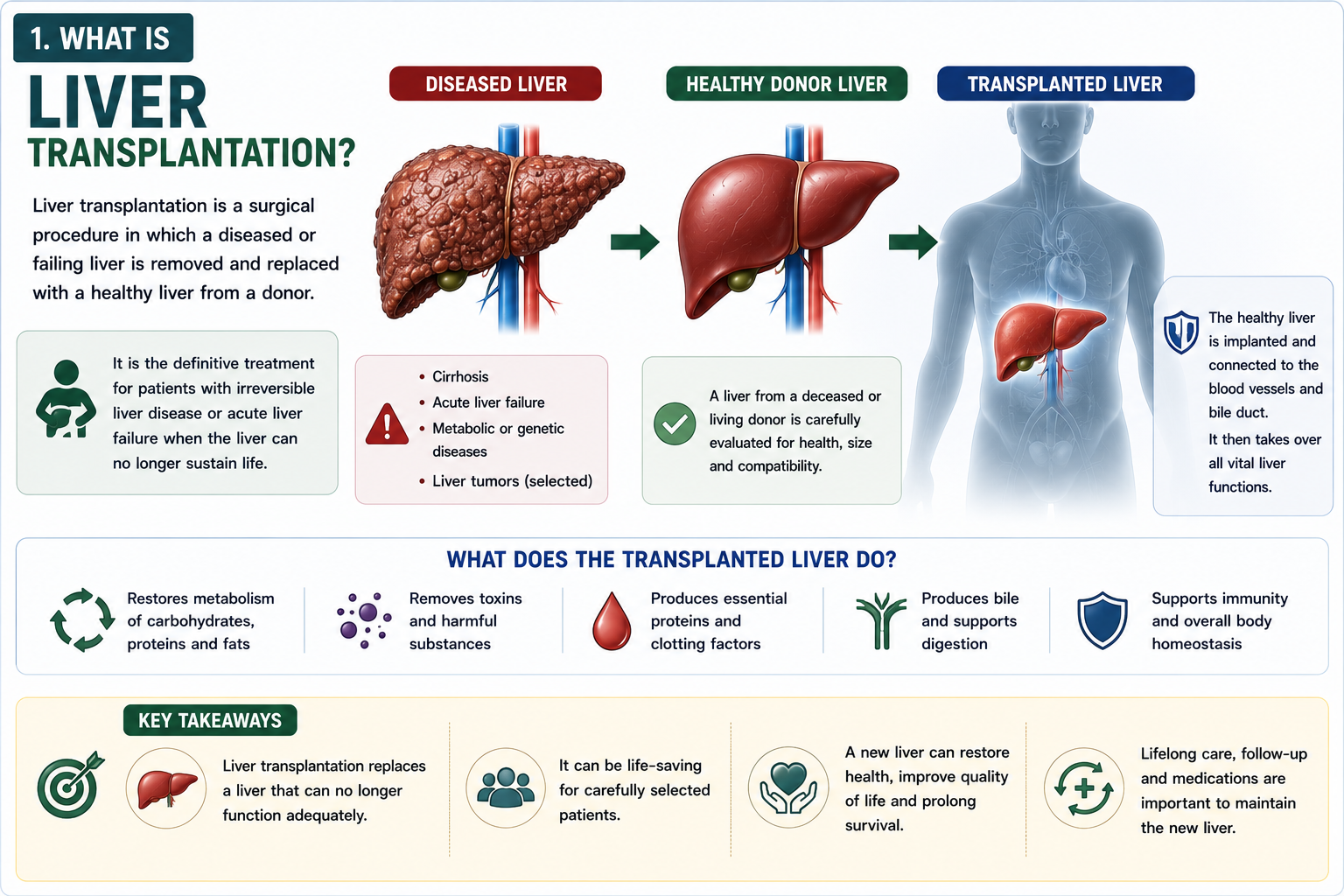
Liver transplantation is a surgical procedure in which a diseased liver is removed and replaced with a healthy donor liver.
The goal is to restore synthesis, detoxification, metabolism, bile production and portal circulation in a patient whose native liver cannot recover.
Transplantation replaces liver function, not simply liver tissue.
Why Is Liver Transplantation Needed?
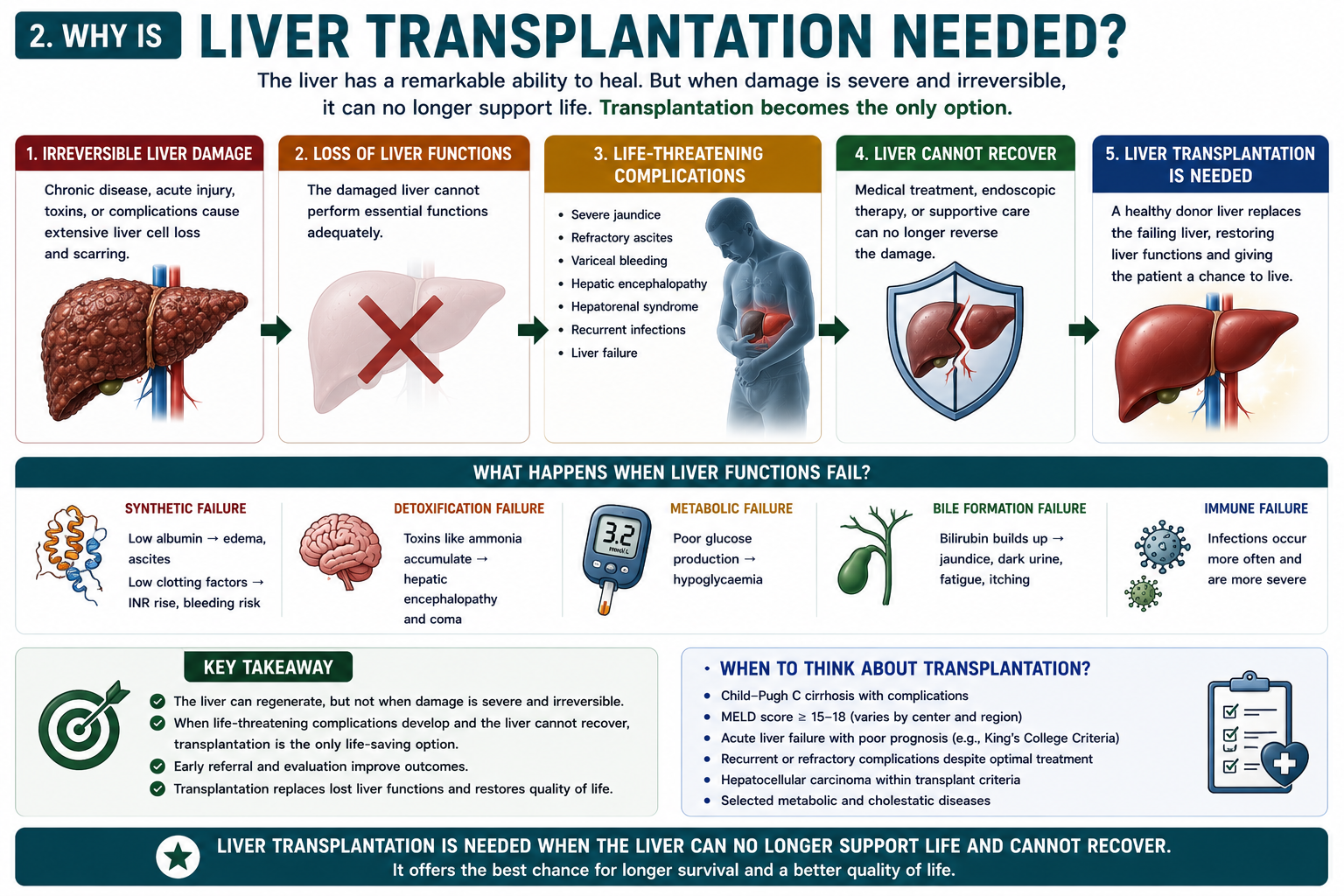
The liver has remarkable regenerative capacity, but regeneration only helps when enough viable liver remains and the injury is reversible.
When is liver transplantation needed? It is considered when liver failure becomes irreversible or when complications cannot be controlled by medical, endoscopic or radiological therapy.
Synthetic failure, detoxification failure, portal hypertension and cancer risk cannot always be reversed. At that point, transplantation becomes the definitive treatment.
Major Indications for Liver Transplantation
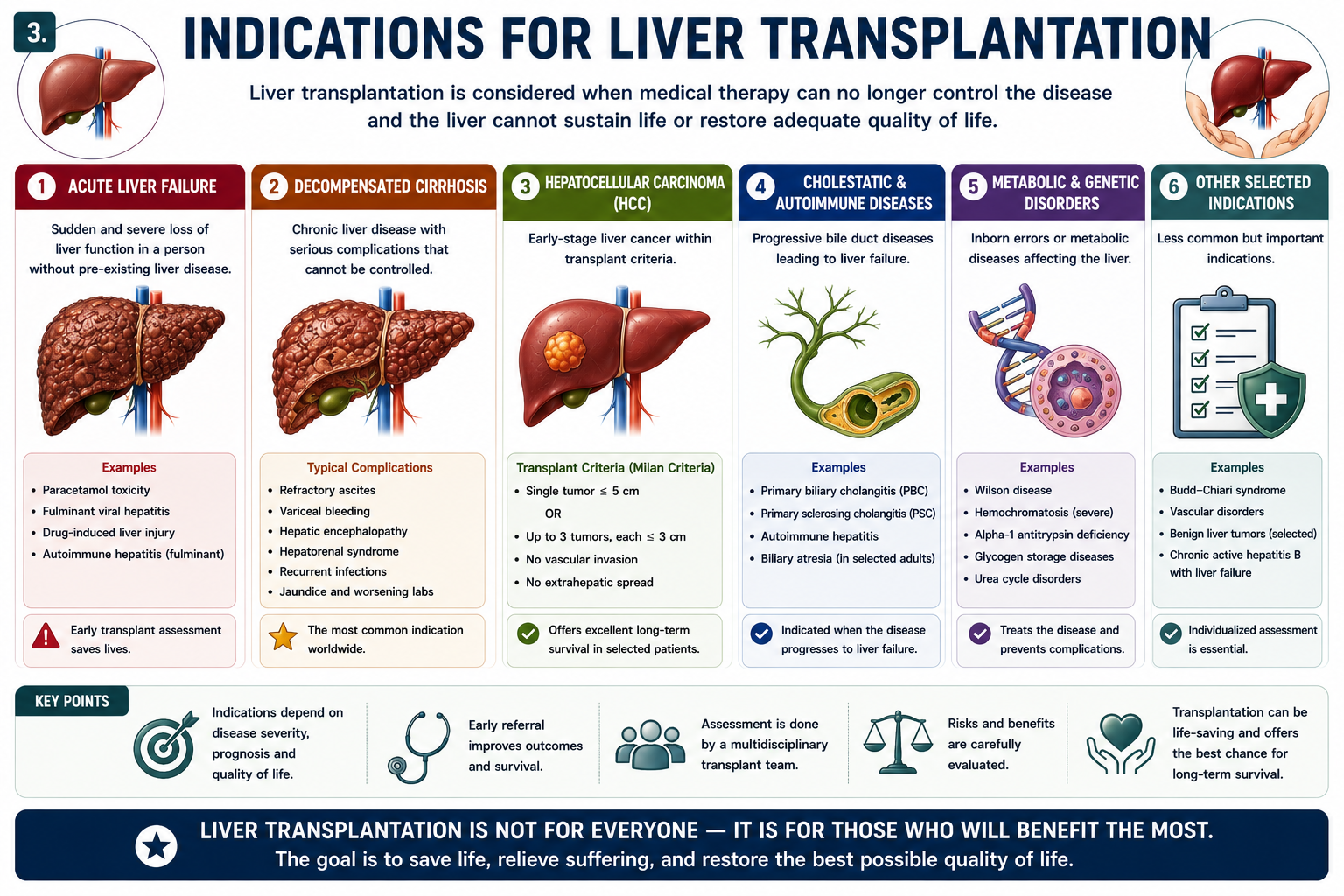
Liver transplant indications include both acute and chronic liver diseases. The common thread is failure of the native liver to provide safe, durable function.
| Category | Examples |
|---|---|
| Acute liver failure | Paracetamol toxicity, fulminant viral hepatitis, Wilson disease |
| Decompensated cirrhosis | Ascites, variceal bleeding, hepatic encephalopathy, hepatorenal syndrome |
| Hepatocellular carcinoma | Selected early tumors within transplant criteria |
| Cholestatic disease | Primary biliary cholangitis, primary sclerosing cholangitis |
| Metabolic disease | Wilson disease, alpha-1 antitrypsin deficiency, selected inherited disorders |
Why Each Disease May Need Transplantation
| Disease | Why Transplantation Is Considered |
|---|---|
| Acute liver failure | The native liver suddenly loses function and may not recover before death or irreversible brain injury occurs. |
| Decompensated cirrhosis | Portal hypertension and liver failure cause ascites, variceal bleeding, encephalopathy or hepatorenal syndrome despite treatment. |
| Hepatocellular carcinoma | Transplant can remove both the tumor and the cirrhotic liver that carries future cancer risk, when tumor burden is within accepted criteria. |
| Wilson disease | Transplant replaces the liver-based copper metabolism defect in severe or fulminant disease. |
| Primary sclerosing cholangitis / primary biliary cholangitis | Progressive cholestatic damage can lead to cirrhosis, recurrent cholangitis, severe symptoms or liver failure. |
| Metabolic liver diseases | Some inherited liver-based metabolic defects can be corrected by replacing the liver. |
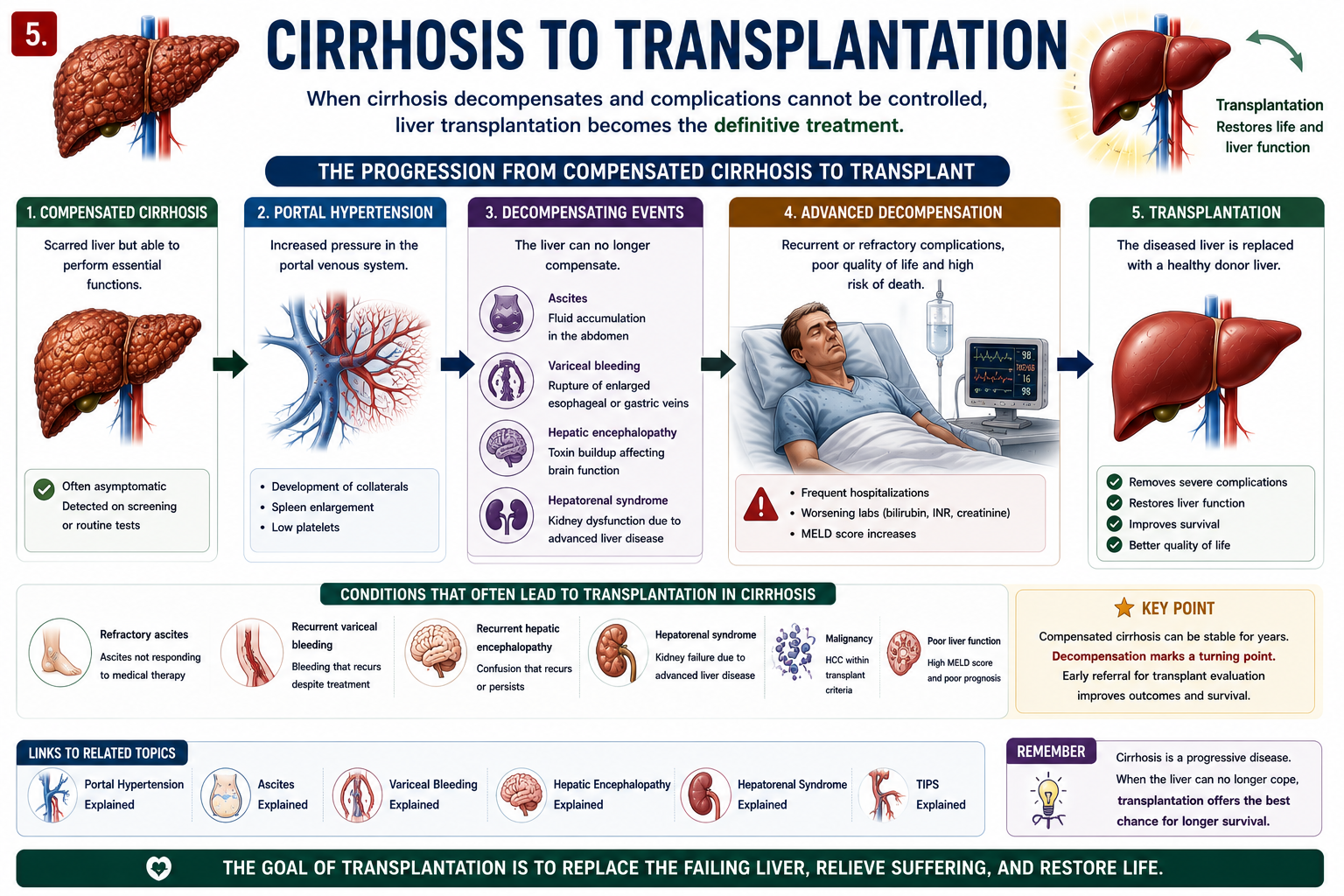
Decompensated cirrhosis is one of the major indications for liver transplantation worldwide.
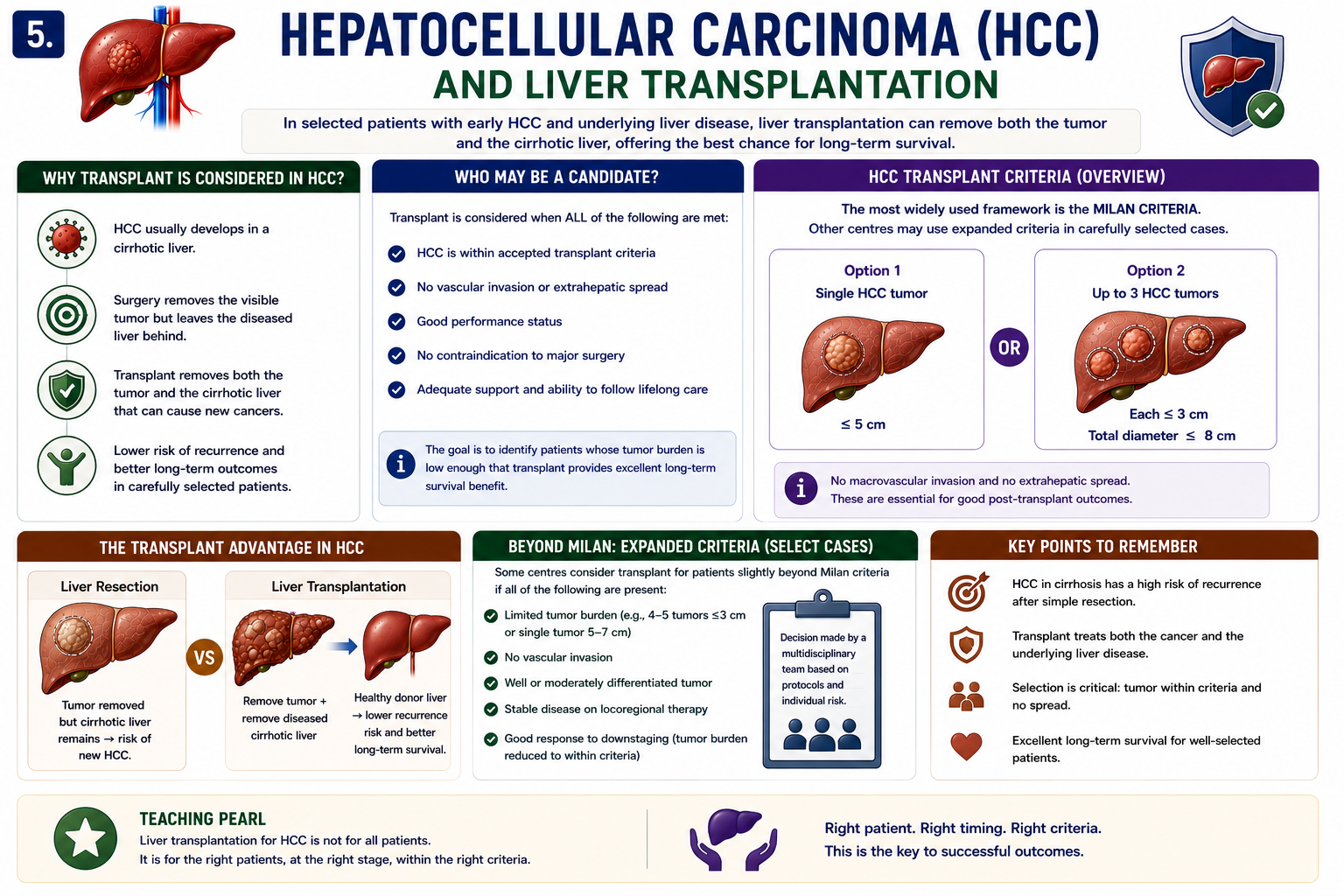
Hepatocellular Carcinoma and Liver Transplantation
Liver transplantation can be considered for selected patients with early hepatocellular carcinoma because it treats both the tumor and the diseased cirrhotic liver underneath.
The best-known framework is the Milan criteria. At student level, the key idea is simple: transplant is considered when tumor burden is limited and there is no vascular invasion or extrahepatic spread.
HCC liver transplant criteria aim to identify patients whose tumor burden is low enough for transplantation to provide good long-term outcomes.
For the full cancer pathway, see Hepatocellular Carcinoma (HCC) Explained.
Resection removes the visible tumor. Transplantation removes both the tumor and the cirrhotic liver that produced the tumor.
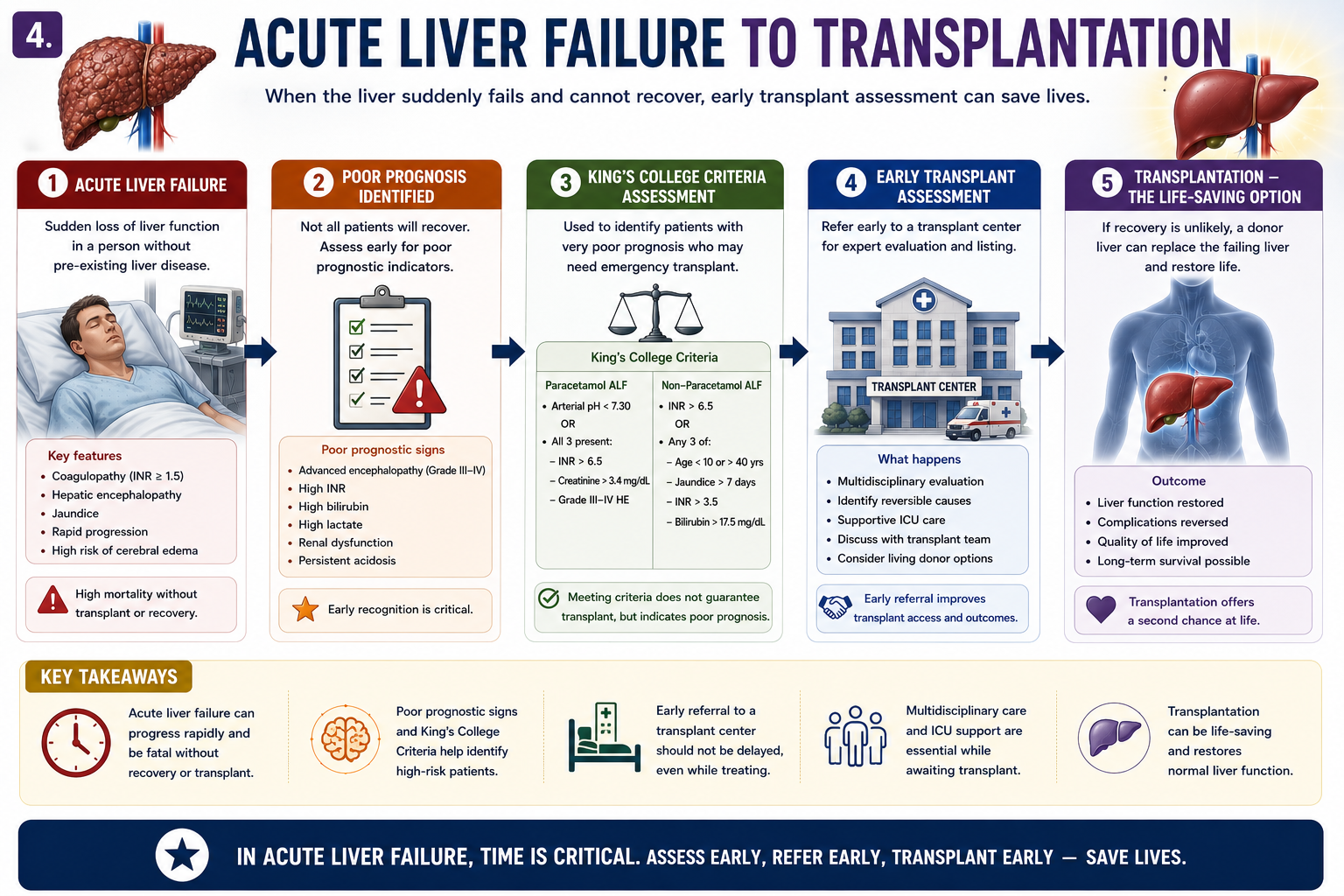
Acute Liver Failure and Liver Transplantation
Acute liver failure transplant assessment is urgent because deterioration can be fast and cerebral edema may become irreversible.
Read Acute Liver Failure Explained first if you need the pathophysiology of INR rise, encephalopathy and cerebral edema.
Transplant assessment should begin before irreversible neurological injury occurs.
Cirrhosis and Liver Transplantation
Cirrhosis liver transplant referral is considered when the patient develops decompensation or high predicted mortality despite optimal care.
This pathway connects much of the hepatology cluster: Portal Hypertension Explained, Ascites Explained, Variceal Bleeding Explained, Hepatic Encephalopathy Explained and Hepatorenal Syndrome Explained.
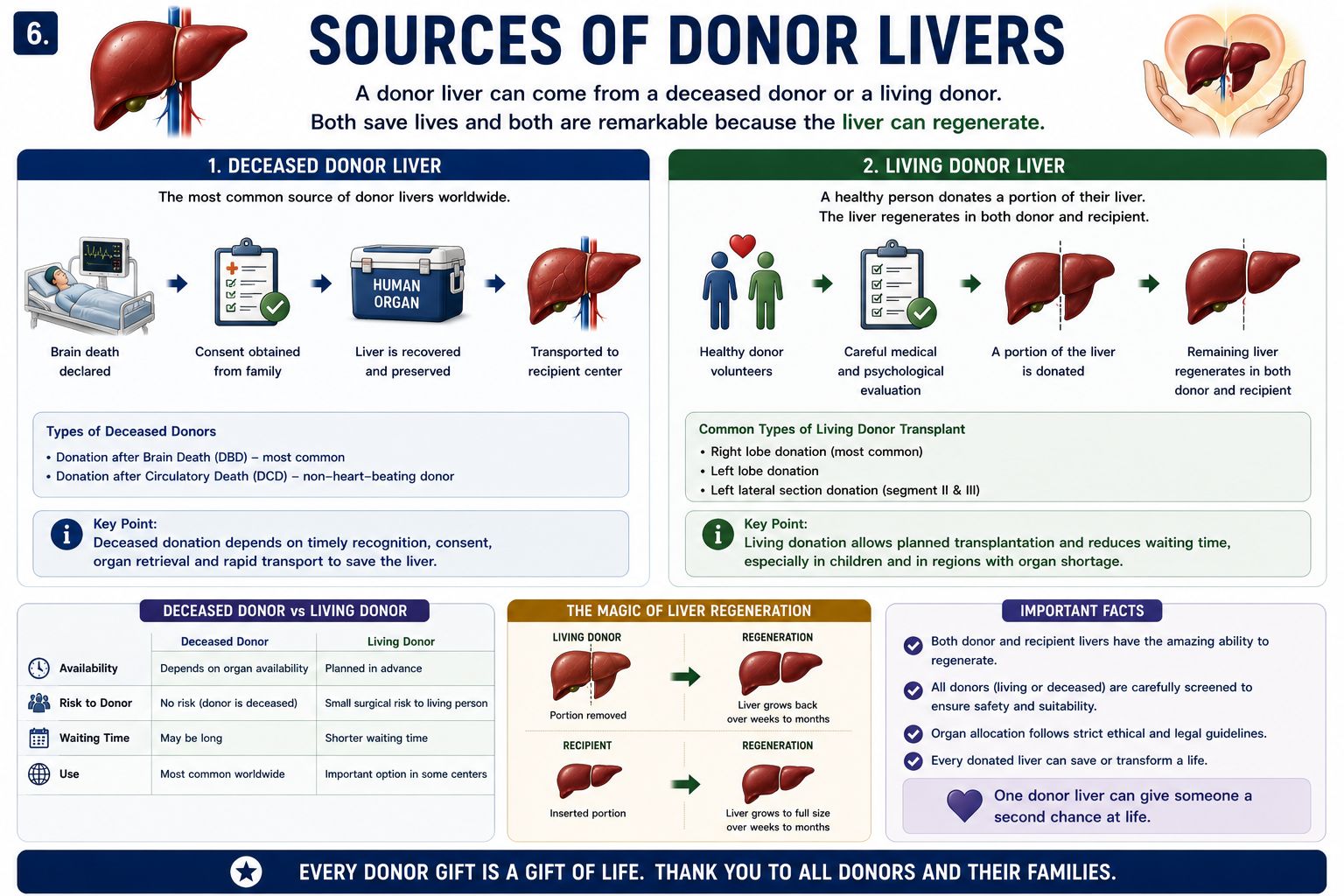
Sources of Donor Livers
Deceased Donor
A deceased donor liver may come from a donor after brain death or, in some systems, donation after circulatory death. This is the most common pathway for whole liver transplantation.
Living Donor
A living donor liver transplant uses part of a healthy donor liver. The remaining liver in the donor and the transplanted liver portion in the recipient can regenerate.
Living donor liver transplant is possible because the liver can regenerate after partial donation.
The liver is unique because both donor and recipient liver tissue can regenerate.
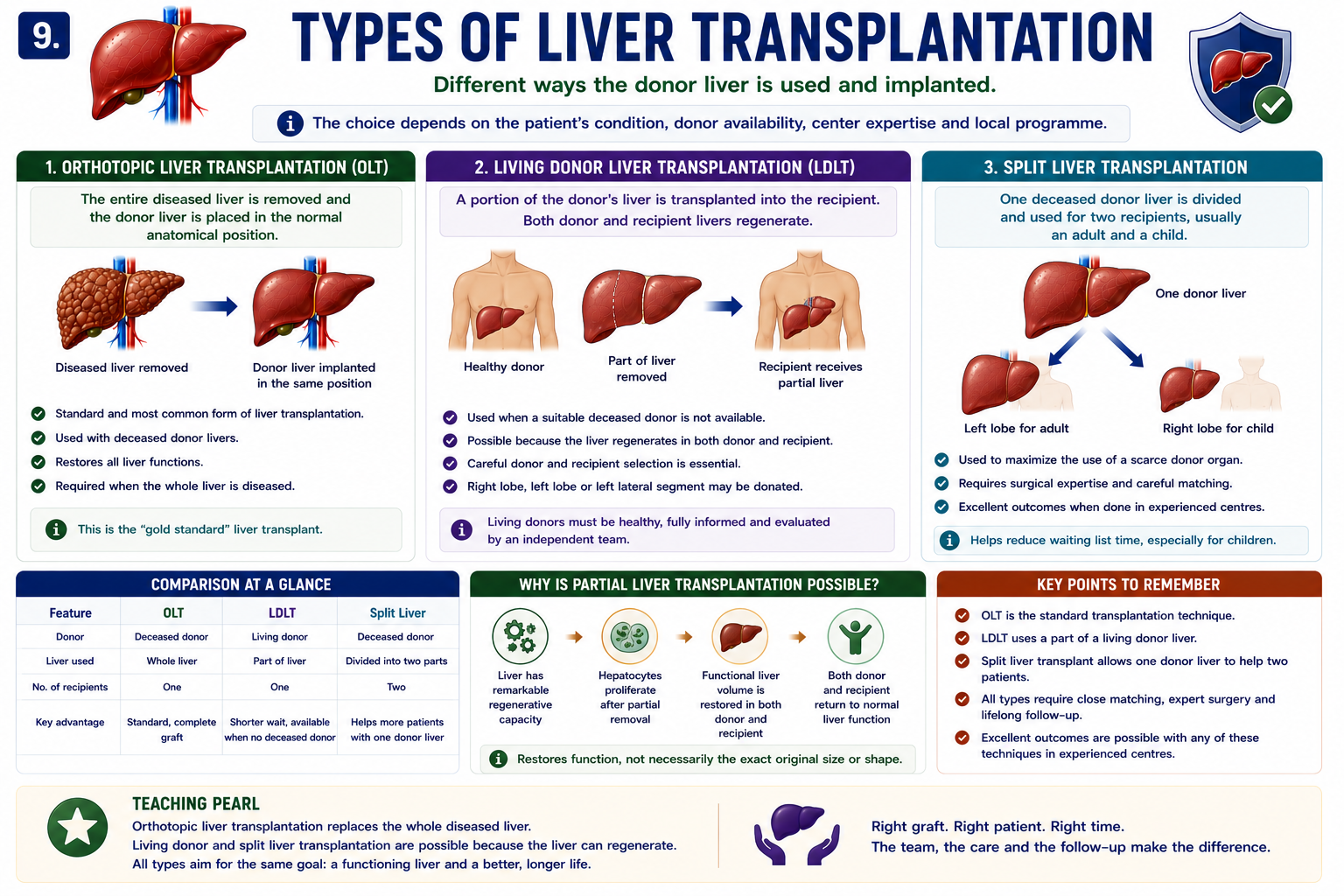
Types of Liver Transplantation
Students often hear terms such as OLT, LDLT and split liver transplantation. These describe how the donor liver is used and implanted.
Orthotopic liver transplantation is the standard operation in which the diseased liver is removed and the donor liver is implanted in the normal anatomical position.
| Type | Meaning | Core Concept |
|---|---|---|
| Orthotopic Liver Transplantation (OLT) | The diseased liver is removed and a donor liver is placed in the normal liver position. | This is the standard form of liver transplantation. |
| Living Donor Liver Transplantation (LDLT) | A living donor gives part of their liver to the recipient. | Possible because the liver can regenerate. |
| Split Liver Transplantation | One deceased donor liver is divided and used for two recipients, often an adult and a child. | Maximizes use of a scarce donor organ. |
Orthotopic liver transplantation means the donor liver is placed in the normal anatomical position after the diseased liver is removed.
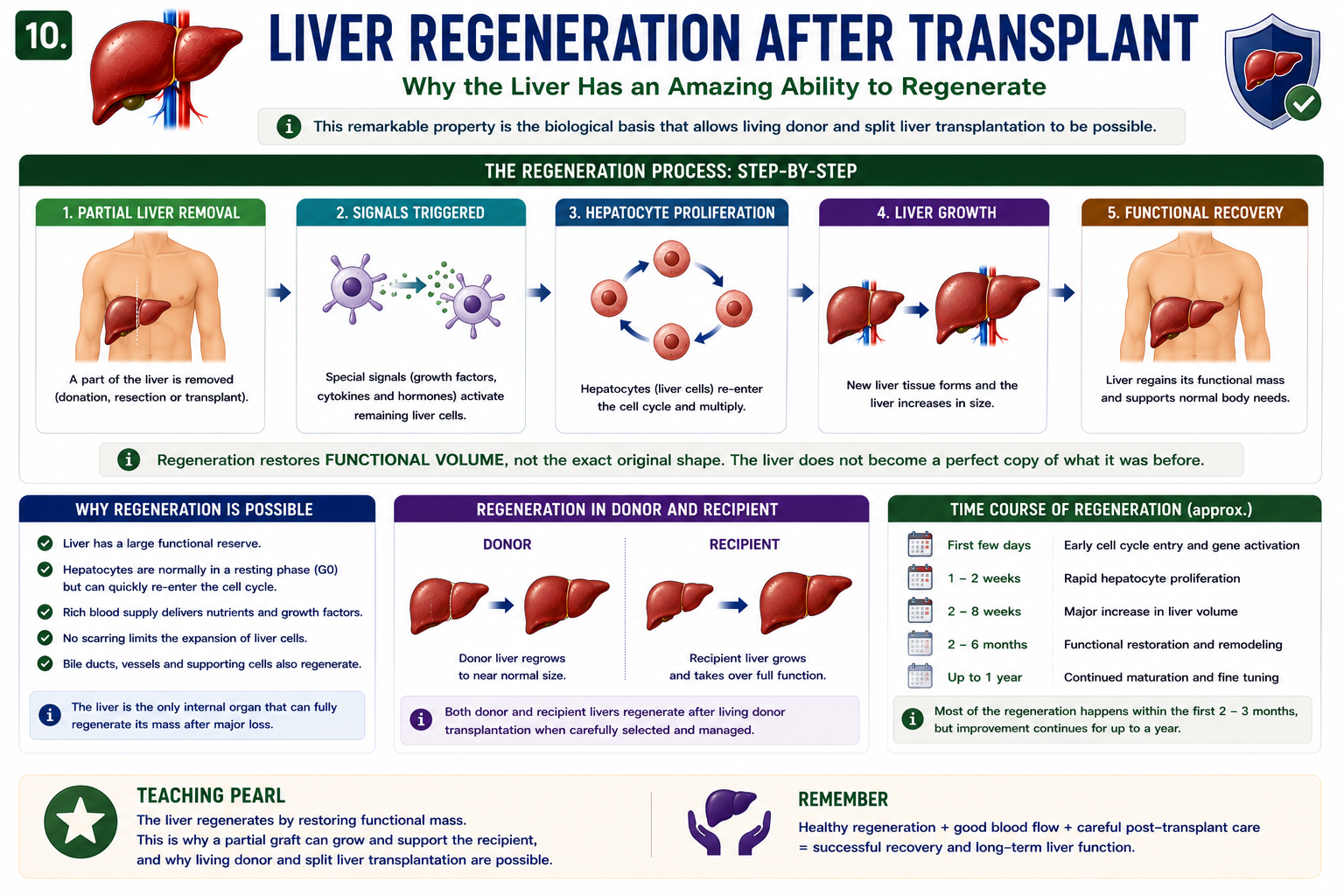
Why Can the Liver Regenerate?
The liver has a remarkable ability to regenerate after partial removal or injury. This is why living donor liver transplantation is possible.
After part of the liver is removed, remaining hepatocytes re-enter the cell cycle and proliferate. The liver restores functional volume rather than recreating the exact original shape.
The liver regenerates by restoring functional mass. This explains why a partial graft can grow and support the recipient after transplantation.
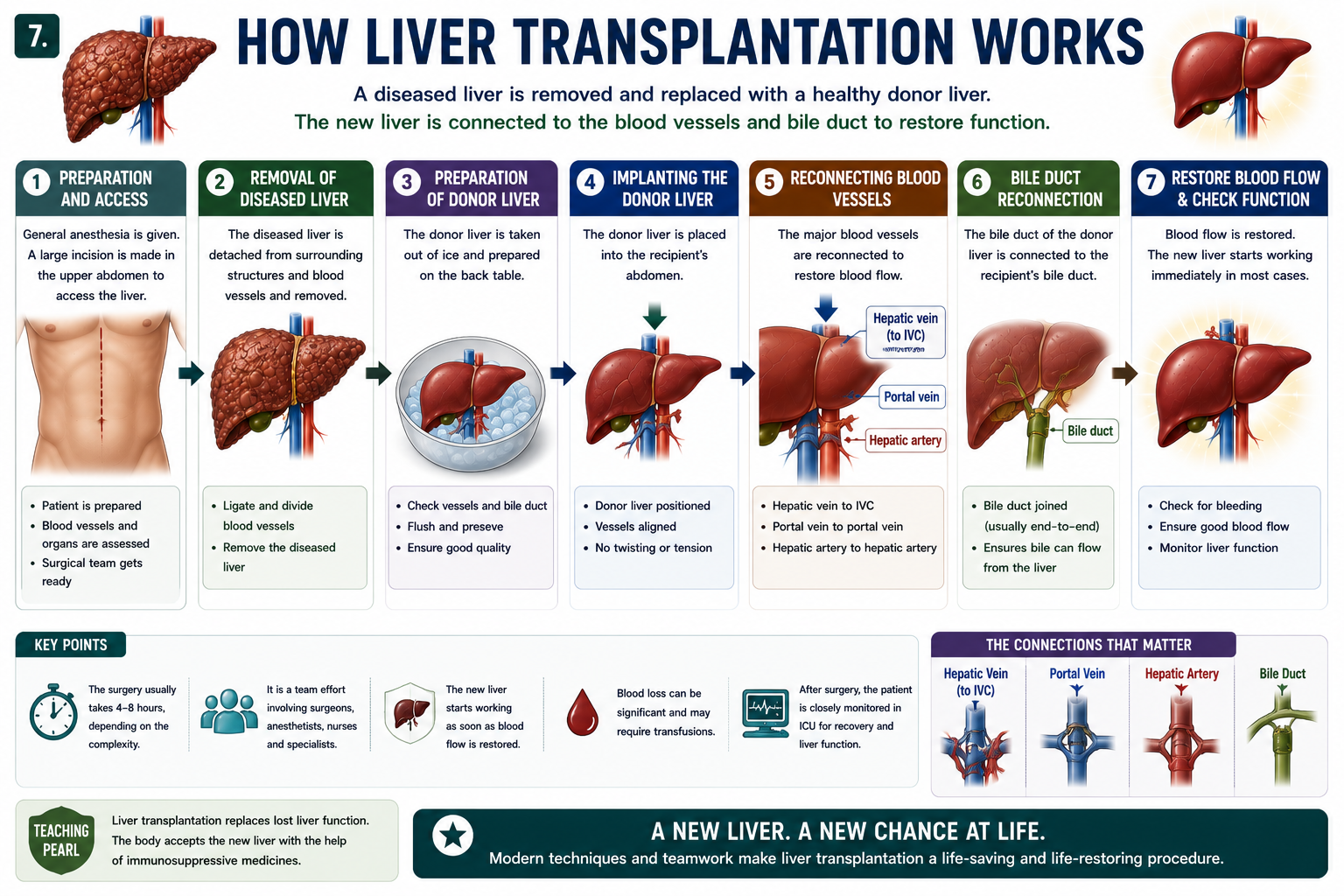
How Liver Transplantation Works
Liver transplant surgery is complex, but the student-level concept is simple: remove the diseased liver, implant the donor liver and reconnect blood flow and bile drainage.
Vascular reconstruction is critical because the donor liver needs immediate inflow from the portal vein and hepatic artery, and venous outflow must drain safely. Bile duct reconstruction restores bile drainage.
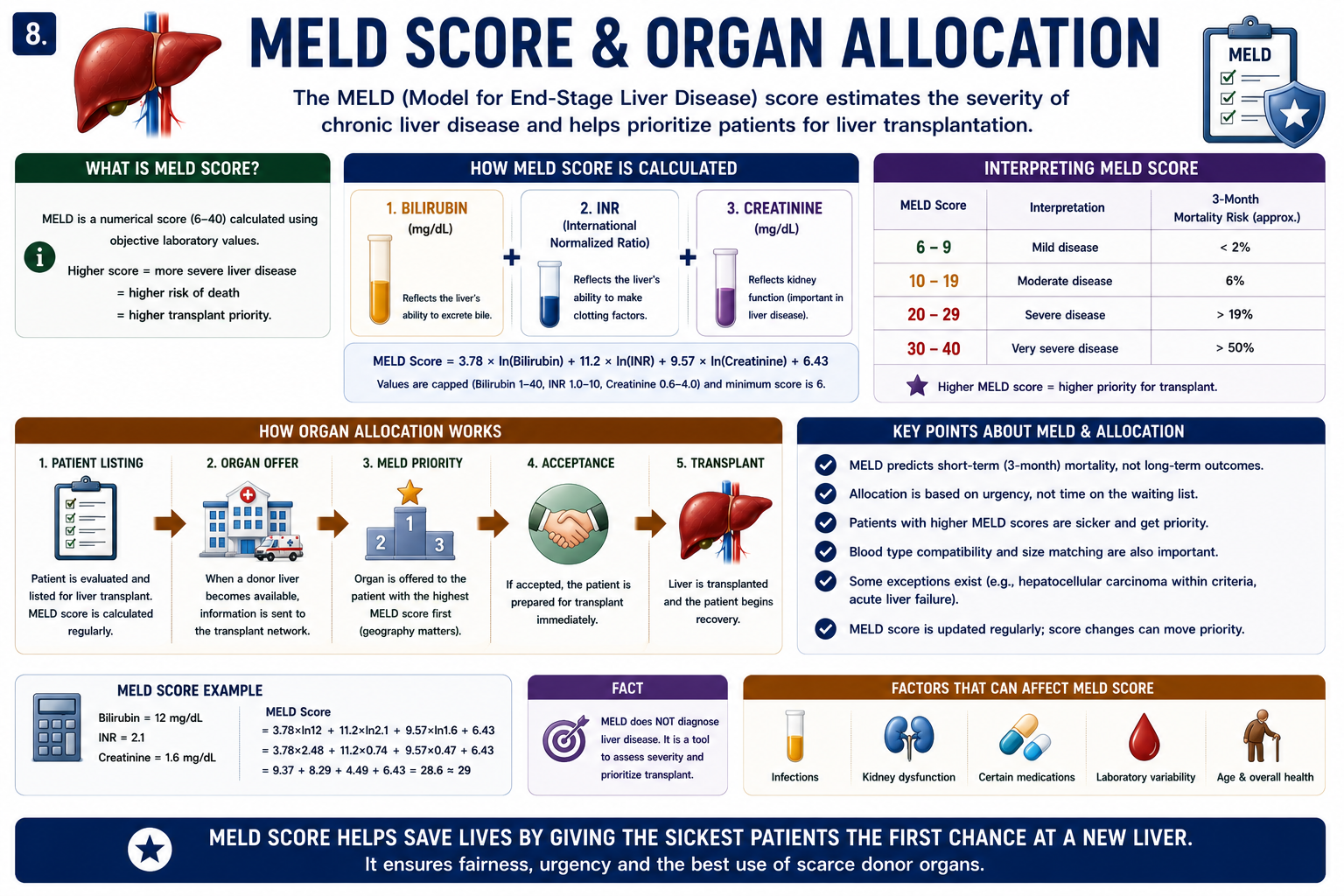
MELD Score and Organ Allocation
The MELD score estimates severity of chronic liver disease and short-term mortality risk. In transplant systems, it helps prioritize patients by medical urgency.
MELD Score Explained covers the formula in more detail. The important point here is that MELD score explained for transplant allocation is about urgency, not diagnosis.
MELD prioritizes urgency rather than waiting time alone. MELD does not diagnose liver disease.
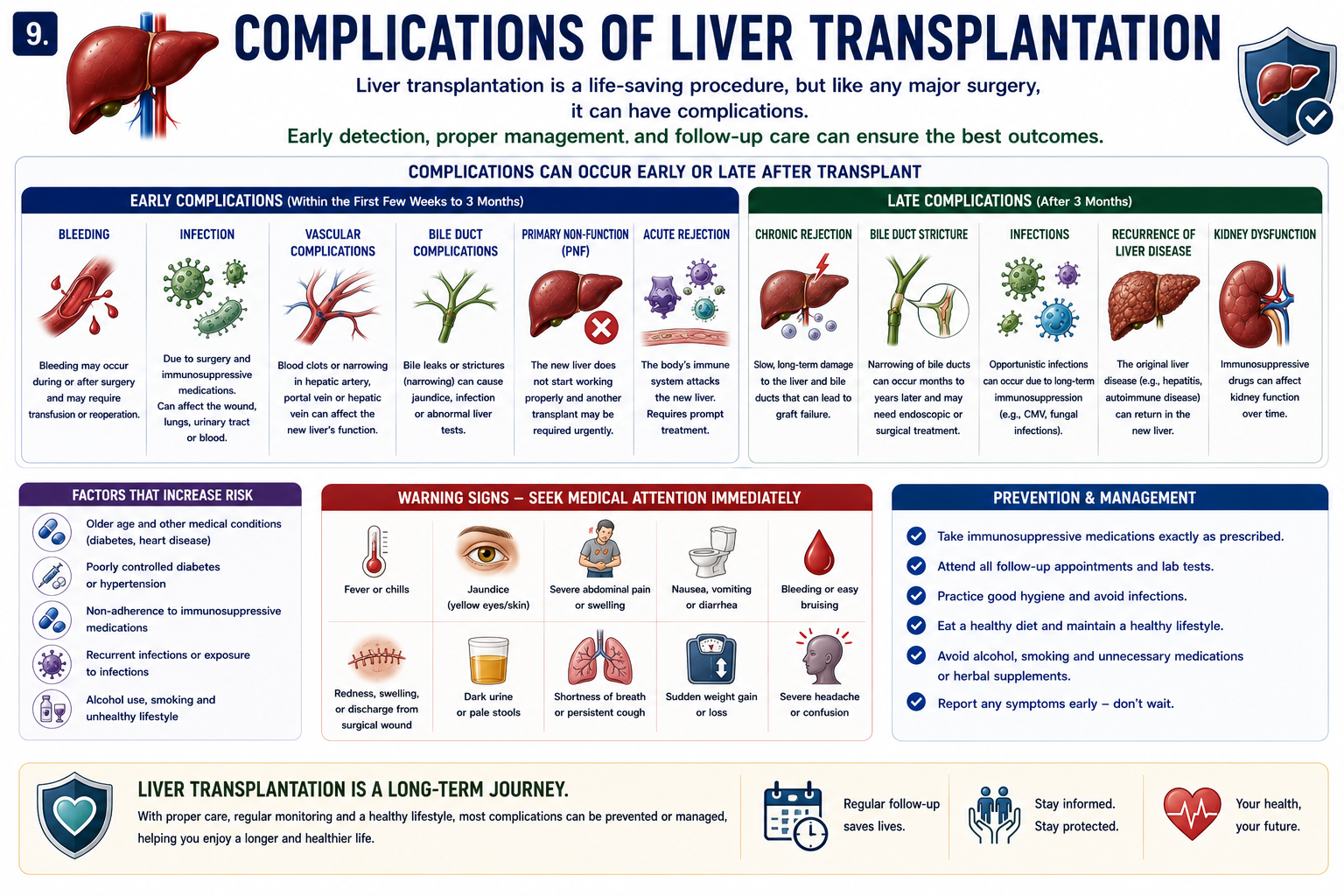
Complications of Liver Transplantation
Liver transplant complications may occur early after surgery or later during long-term follow-up.
| Early | Late |
|---|---|
| Bleeding | Chronic rejection |
| Infection | Renal dysfunction |
| Vascular thrombosis | Malignancy |
| Biliary leak or stricture | Metabolic complications such as diabetes, hypertension and dyslipidemia |
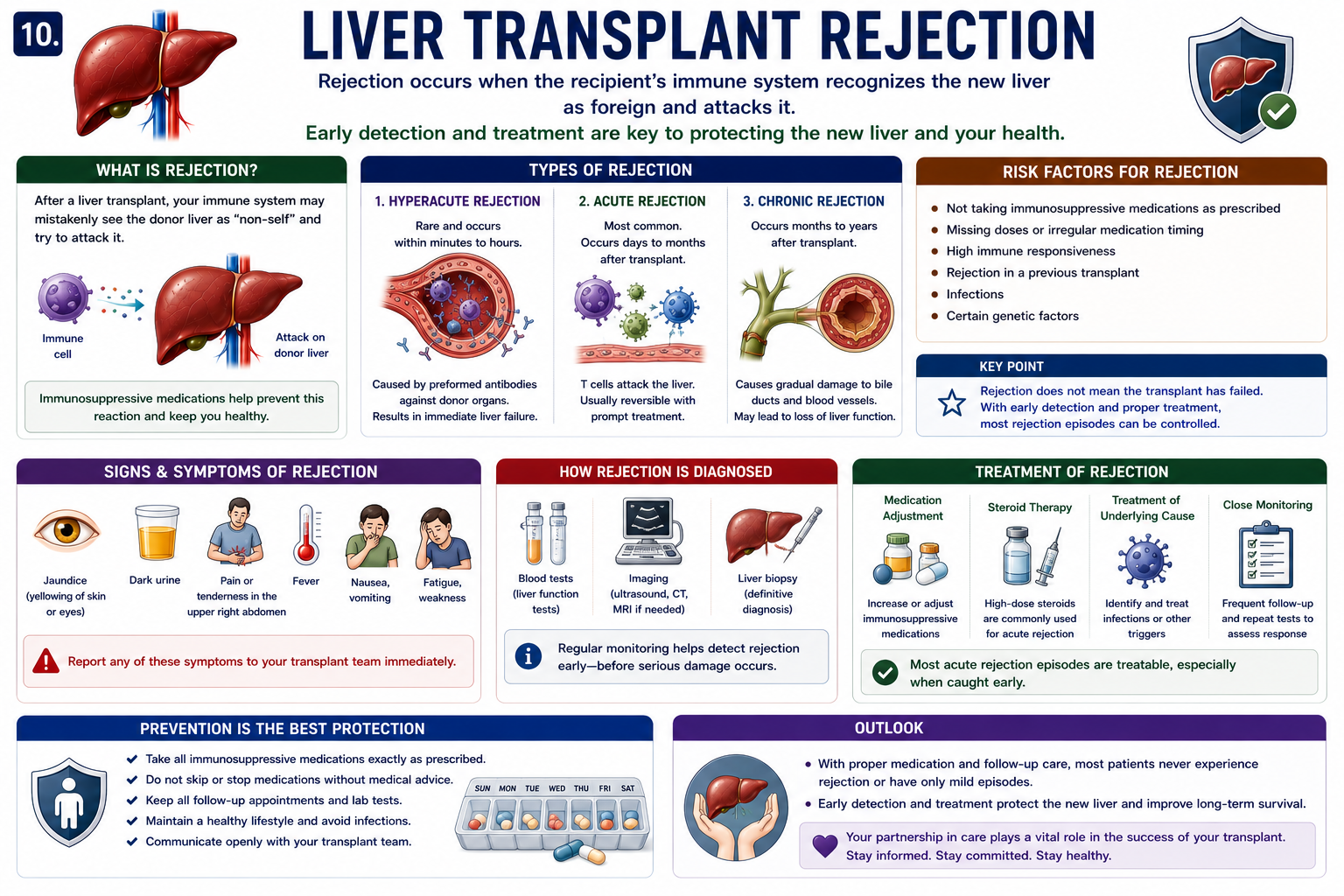
Rejection Explained
Liver transplant rejection occurs when the recipient immune system recognizes the donor liver as foreign and attacks it.
Rejection may be hyperacute, acute or chronic. Acute cellular rejection is the most common teaching topic and is often treatable when detected early.
Liver transplant rejection symptoms may include fever, jaundice, dark urine, fatigue, abdominal discomfort or abnormal liver tests, but rejection can also be detected during routine monitoring.
Most rejection episodes can be treated successfully when detected early.
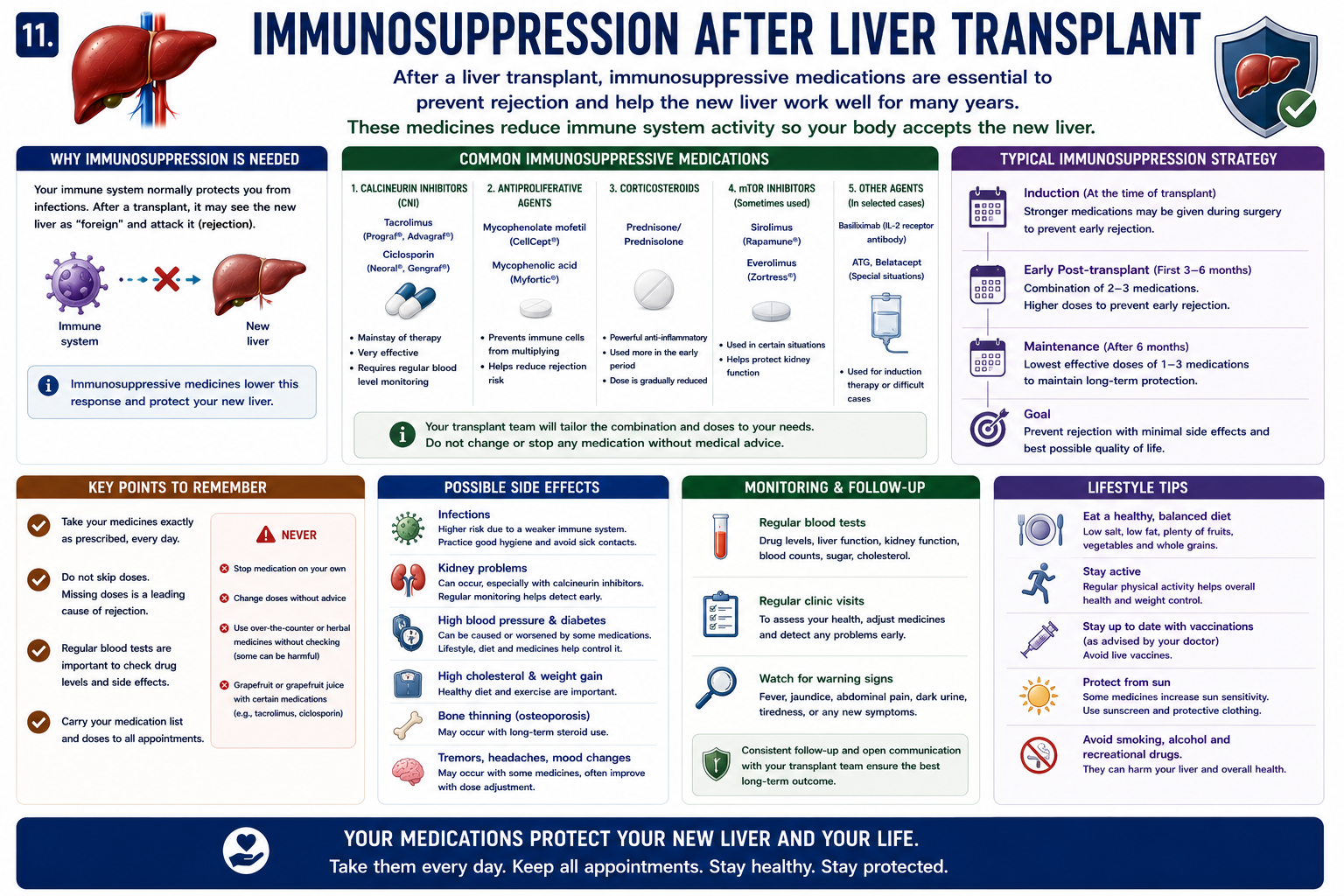
Immunosuppression After Transplant
Liver transplant immunosuppression reduces immune attack on the donor liver and helps preserve graft function.
Common drugs include tacrolimus, mycophenolate and corticosteroids. Tacrolimus is a cornerstone immunosuppressive drug, but long-term therapy requires monitoring for infection, kidney injury, diabetes, hypertension and other complications.
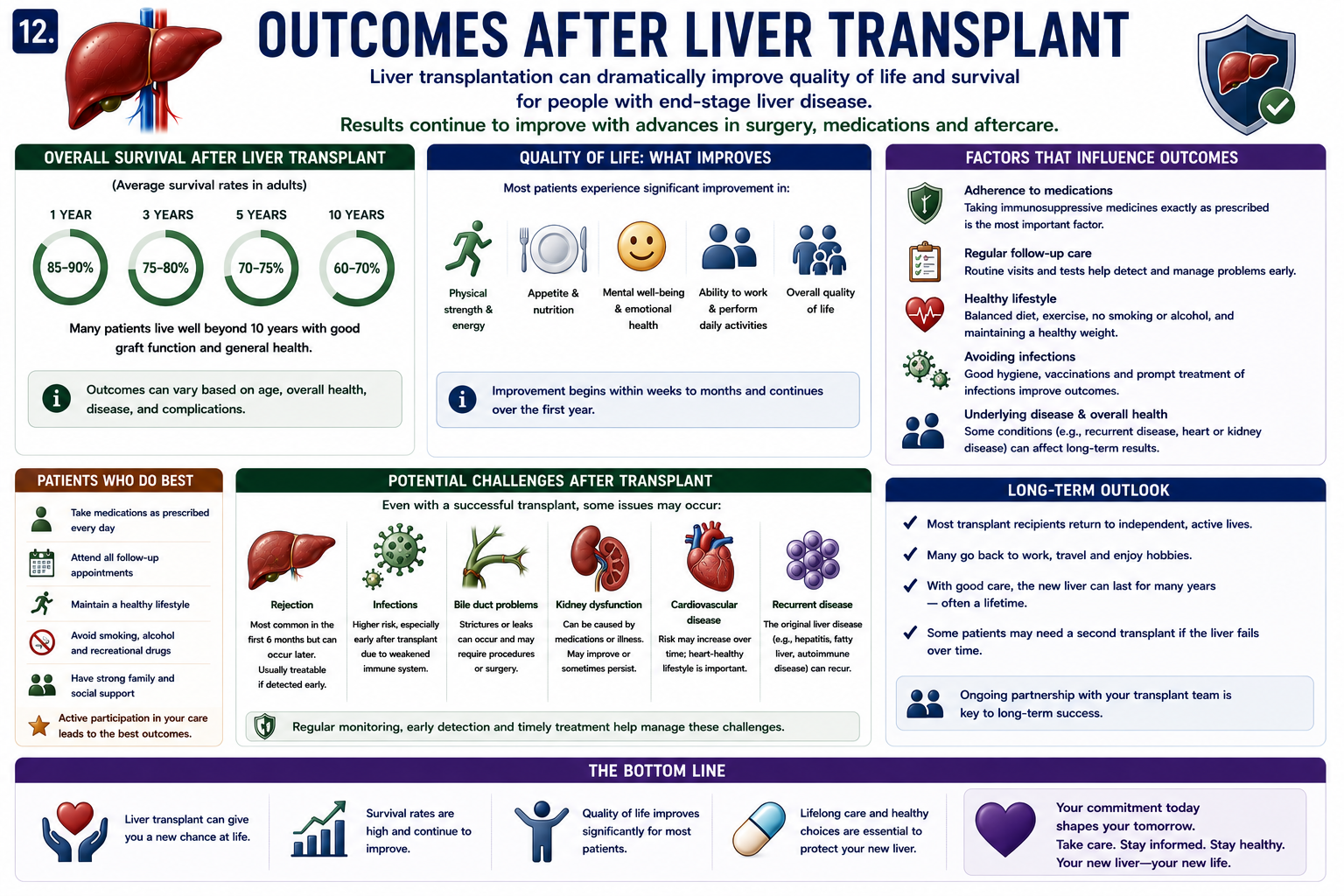
Outcomes After Liver Transplantation
Modern liver transplantation has excellent outcomes for carefully selected patients. Many recipients return to education, work and family life with improved quality of life.
Life after liver transplant requires adherence to immunosuppression, infection prevention, clinic follow-up, cancer screening and management of metabolic risk factors.
Life after liver transplant usually involves long-term medications, clinic follow-up and monitoring, but many patients return to work, education and family life.
- Long-term survival
- Return to work or education
- Improved quality of life
- Long-term follow-up to monitor graft function and complications
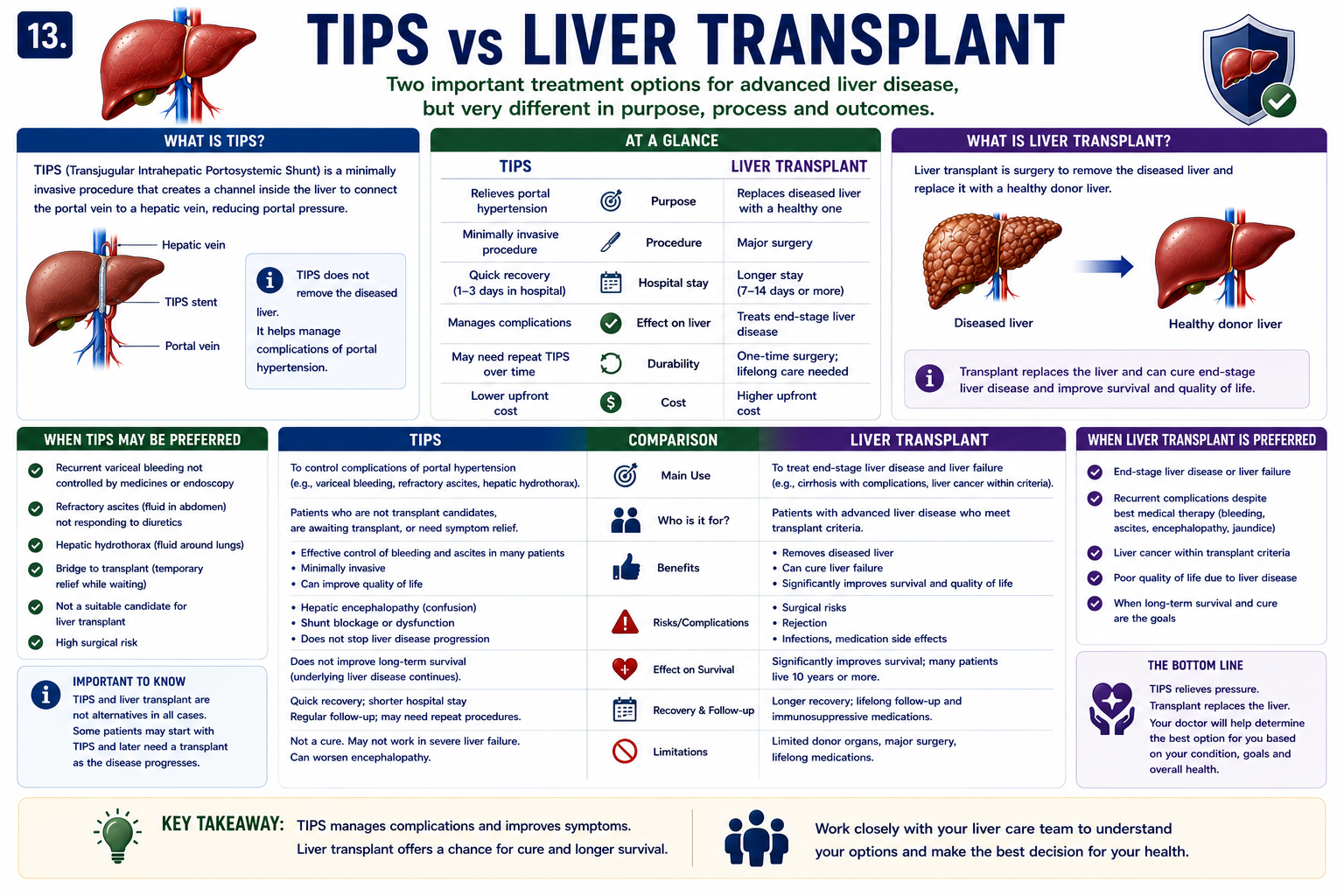
Liver Transplant vs TIPS
TIPS and transplantation sit at different points in the treatment pathway.
| TIPS | Transplant |
|---|---|
| Reduces portal pressure | Replaces the failing liver |
| Native liver remains | Native liver removed |
| Bridge therapy | Definitive therapy |
| Treats complications | Treats underlying liver failure |
TIPS buys time. Transplant replaces the failing liver.
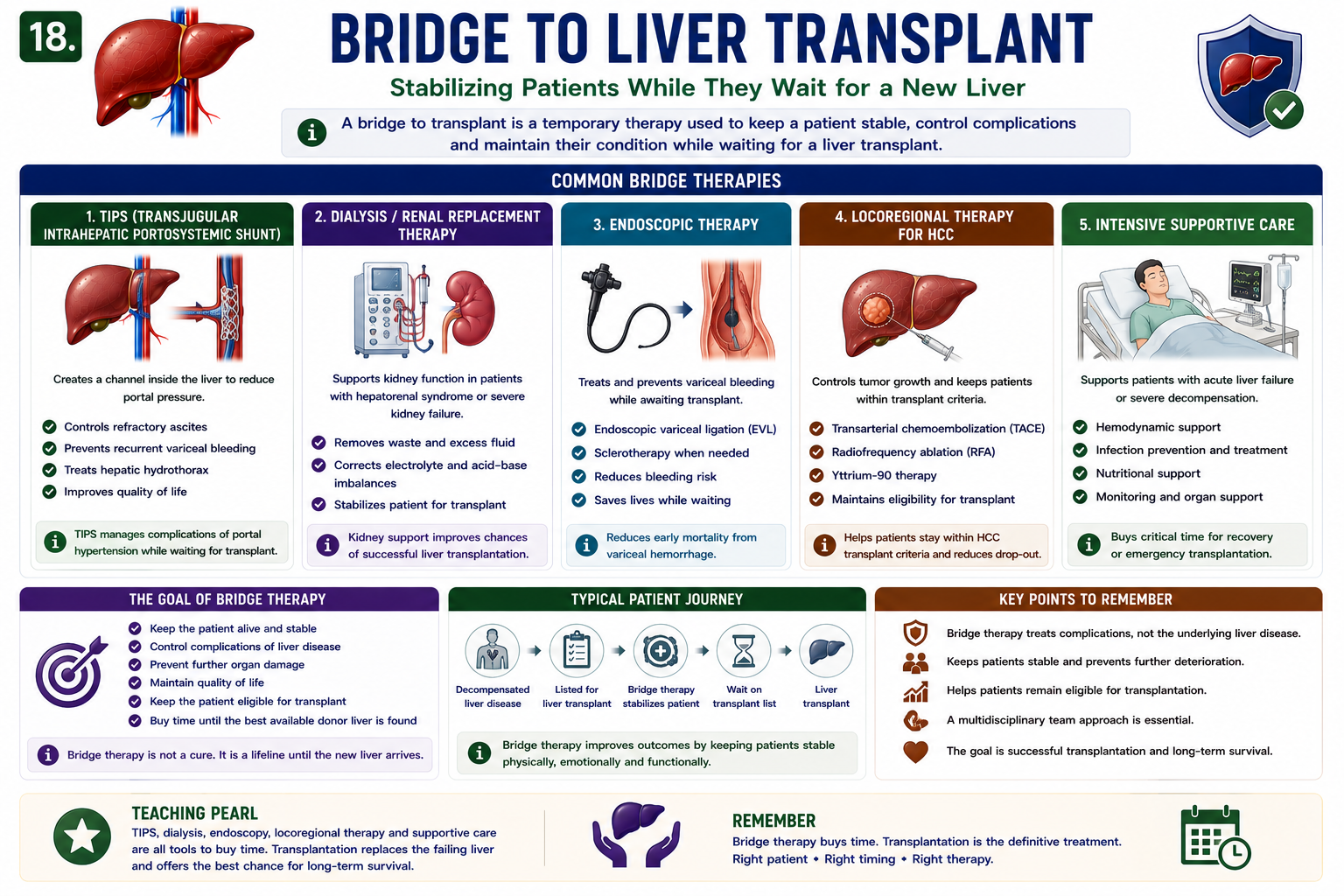
What Does “Bridge to Transplant” Mean?
A bridge to transplant is a treatment that keeps a patient stable while waiting for liver transplantation. It does not usually cure the underlying liver disease, but it reduces risk and buys time.
A bridge to liver transplant is not a cure; it is a stabilizing treatment used while a patient is awaiting transplantation.
| Bridge Therapy | What It Does |
|---|---|
| TIPS | Controls complications of portal hypertension such as refractory ascites, variceal bleeding or hepatic hydrothorax. |
| Dialysis / renal replacement therapy | Supports kidney function in patients with renal failure while awaiting transplant. |
| Endoscopic therapy | Controls variceal bleeding risk while awaiting definitive treatment. |
| Locoregional therapy for HCC | Controls tumor growth and keeps selected patients within transplant criteria. |
| Intensive supportive care | Supports patients with acute liver failure while awaiting recovery or emergency transplantation. |
Bridge therapy buys time. Transplantation is the definitive treatment when the liver cannot recover.
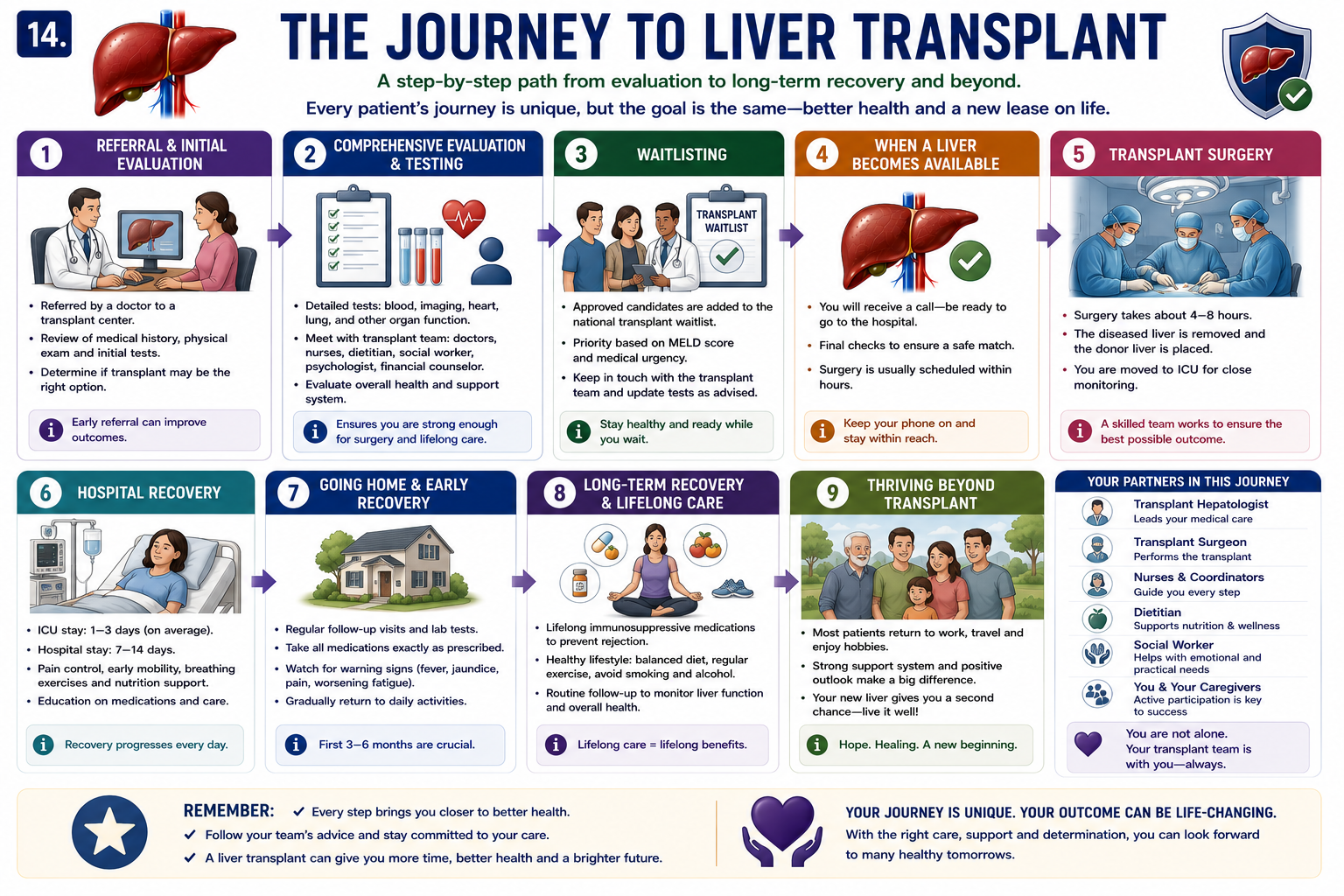
Journey to Liver Transplantation
The transplant journey is not one operation alone. It is a pathway involving referral, assessment, listing, donor matching, surgery and lifelong follow-up.
The liver transplant waiting list is used to organize approved candidates according to urgency, compatibility and organ availability.
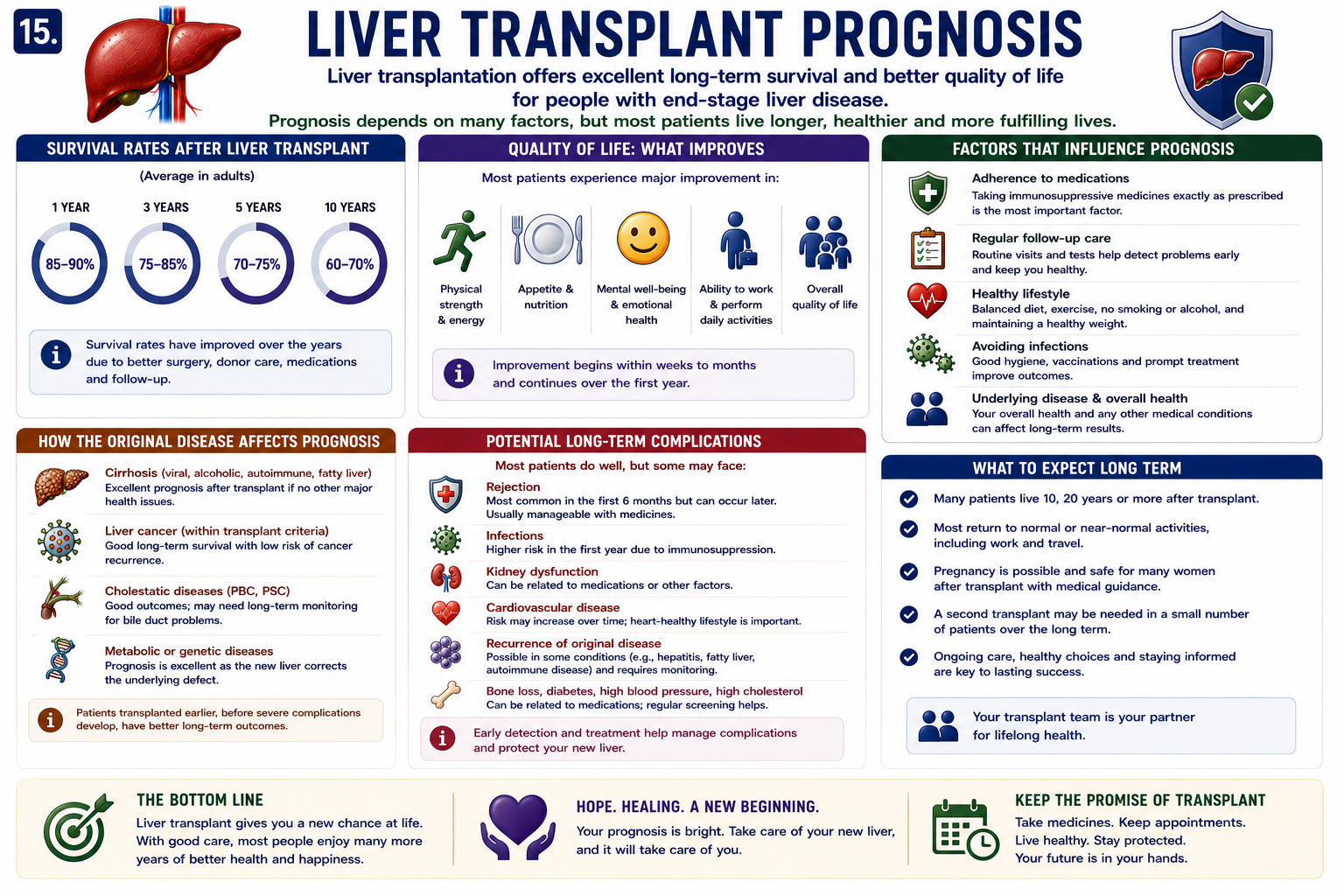
Prognosis
Modern transplantation provides excellent one-year and five-year survival in many patients, especially when transplant assessment, surgery and follow-up occur in experienced centers.
Liver transplant survival rates are generally excellent in carefully selected patients, especially with good graft function and medication adherence.
| Better Outcome | Worse Outcome |
|---|---|
| Good medication adherence | Poor adherence |
| Early diagnosis and referral | Late complications |
| Good graft function | Recurrent disease |
| Controlled infection risk | Severe infection or malignancy |
High-Yield Exam Pearls
- Acute liver failure is a major transplant indication.
- Decompensated cirrhosis is one of the major indications.
- MELD score prioritizes organ allocation by urgency.
- Living donor transplantation is possible because the liver regenerates.
- Tacrolimus is a cornerstone immunosuppressive drug.
- Rejection results from immune attack on the donor liver.
- TIPS is not a substitute for transplantation.
- Early referral improves outcomes.
Frequently Asked Questions
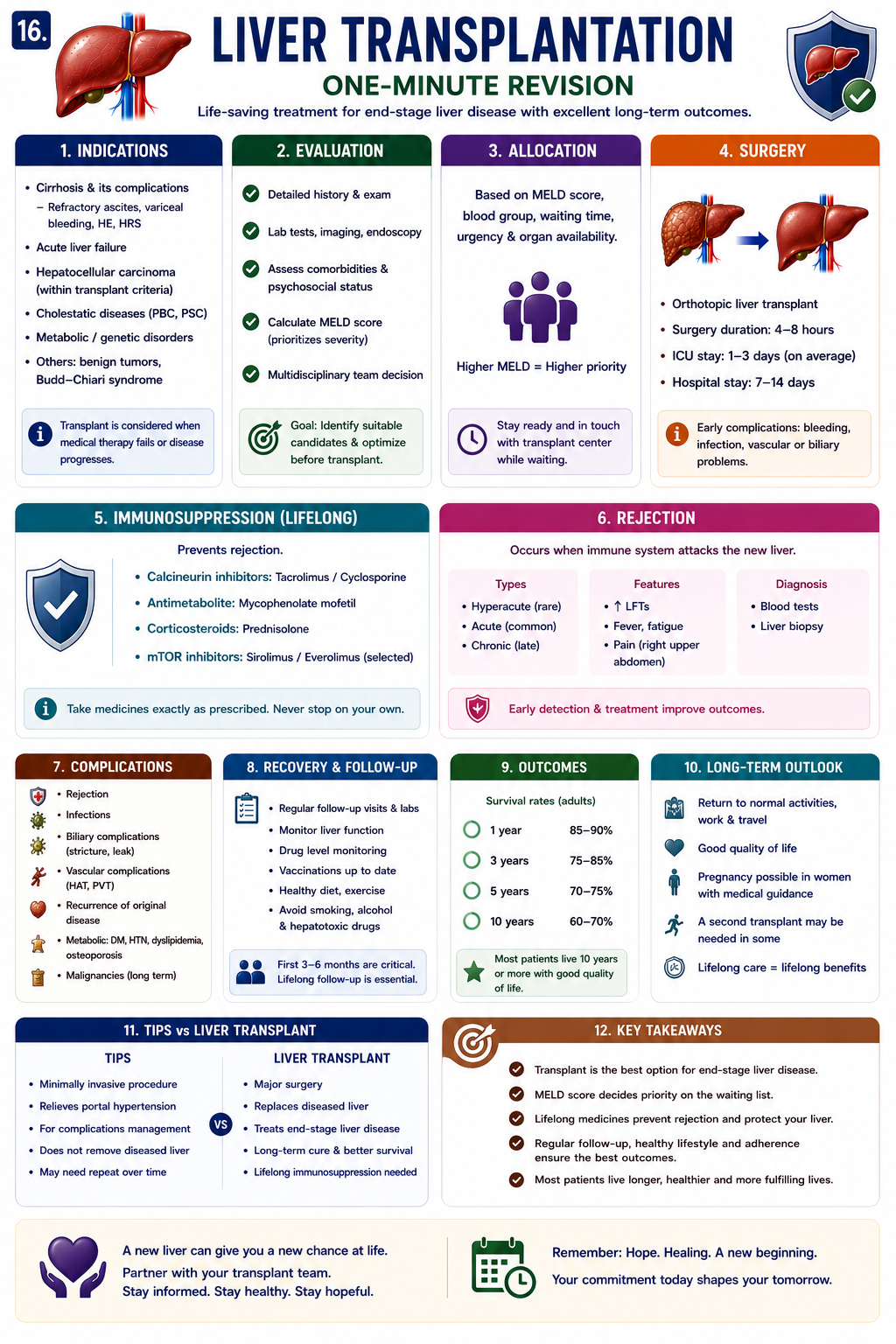
One-Minute Liver Transplantation Revision
Key Takeaways
- Liver transplantation restores life-sustaining liver function when native liver failure is irreversible.
- Major indications include acute liver failure, decompensated cirrhosis, selected HCC and metabolic disease.
- MELD score helps prioritize transplant allocation by mortality risk.
- Donor livers may come from deceased or living donors.
- Rejection is immune attack on the donor liver and is prevented with immunosuppression.
- TIPS can bridge complications, but transplantation replaces the failing liver.
Liver transplantation is the definitive treatment when acute liver failure, decompensated cirrhosis, selected HCC or metabolic liver disease cannot be controlled by other therapy. The core idea is functional replacement: the donor liver restores synthesis, detoxification, metabolism, bile production and long-term survival. Remember the clinical hierarchy: medical therapy controls disease, TIPS buys time, bridge therapies stabilize patients, and transplantation replaces the failing liver.
References
- Girish V, Mousa OY. Liver Transplantation. StatPearls. Updated 2025.
- Martin P, DiMartini A, Feng S, Brown R Jr, Fallon M. Evaluation for liver transplantation in adults: 2013 practice guideline by AASLD and AST. Hepatology. 2014;59(3):1144-1165.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Liver transplantation. J Hepatol. 2016;64(2):433-485.
- Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33(2):464-470.
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334(11):693-699.
This article is intended for medical education only. It does not constitute clinical advice. Liver transplantation decisions require specialist hepatology, transplant surgery, anesthesia, critical care and multidisciplinary transplant-center assessment.
- What Is Transplantation?
- Why It Is Needed
- Indications
- HCC and Transplant
- Acute Liver Failure
- Cirrhosis
- Donor Sources
- Types of Transplant
- Liver Regeneration
- Surgery
- MELD and Allocation
- Complications
- Rejection
- Immunosuppression
- Outcomes
- TIPS vs Transplant
- Bridge to Transplant
- Transplant Journey
- Prognosis
- Exam Pearls
- FAQ
- One-Minute Revision
- Key Takeaways
- References