Students often confuse portal hypertensive gastropathy with gastric varices, peptic ulcer disease, and GAVE (gastric antral vascular ectasia).
PHG is a distinct entity. Unlike gastric varices, it rarely causes sudden catastrophic haemorrhage. Instead it causes chronic occult blood loss, iron deficiency anaemia, and persistent morbidity in patients with cirrhosis.
Understanding PHG requires understanding portal hypertension — because PHG is fundamentally a vascular consequence of elevated portal venous pressure, not a primary gastric disease.
Portal hypertension → varices → variceal bleeding (acute haemorrhage)
Portal hypertension → gastric mucosal congestion → PHG (chronic blood loss)
Portal hypertension → ascites → SBP, HRS
Portal hypertension → TIPS → PHG improvement
Where PHG Fits in Portal Hypertension
Portal hypertensive gastropathy is one member of the wider portal hypertension complication family. It should be understood alongside varices, ascites, SBP, HRS and hepatic encephalopathy.
The key difference is the bleeding pattern. Varices bleed dramatically when they rupture. PHG usually bleeds slowly from a congested gastric mucosal surface.
Think of PHG as the stomach-mucosa complication of portal hypertension. It sits between varices and chronic anaemia in the portal hypertension cluster.
Learning Objectives
- Define portal hypertensive gastropathy and explain its relationship to portal hypertension
- Describe the pathophysiology: how elevated portal pressure causes gastric mucosal vascular changes
- Recognise the typical endoscopic appearances of mild and severe PHG
- Explain how PHG causes anaemia through chronic occult blood loss
- Distinguish PHG from GAVE and from gastric varices
- Outline the management approach including beta blockers, iron replacement and TIPS
What Is Portal Hypertensive Gastropathy?
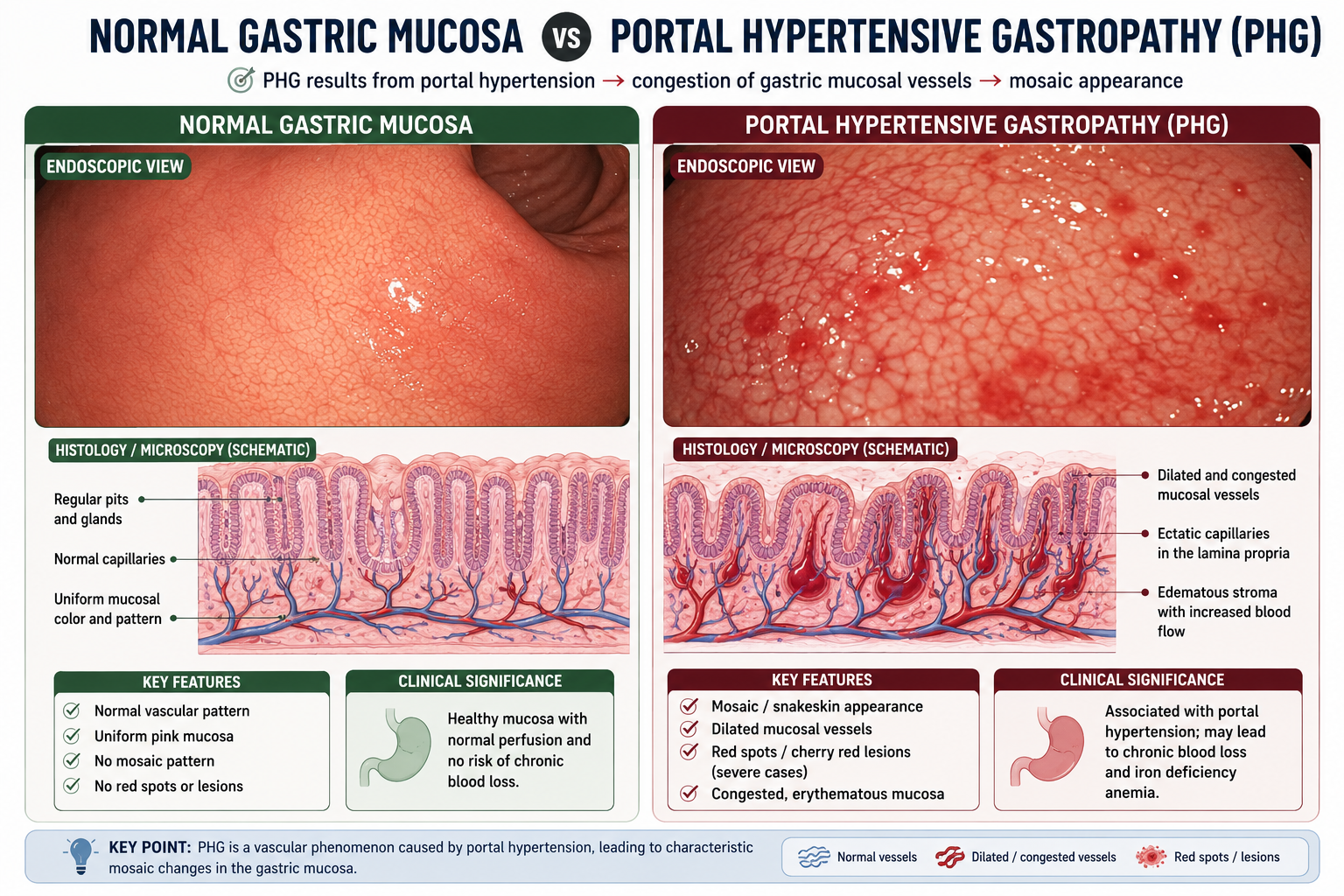
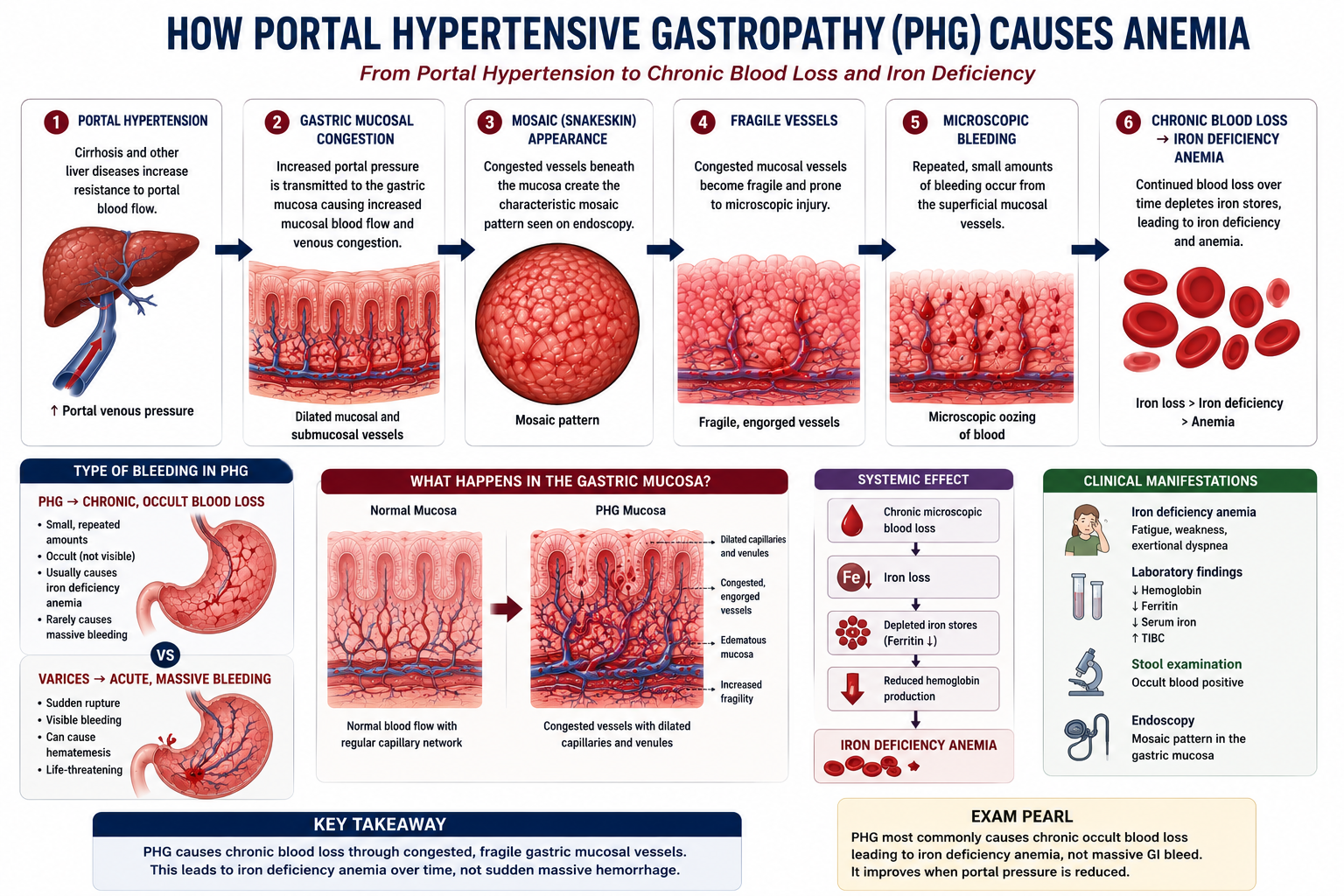
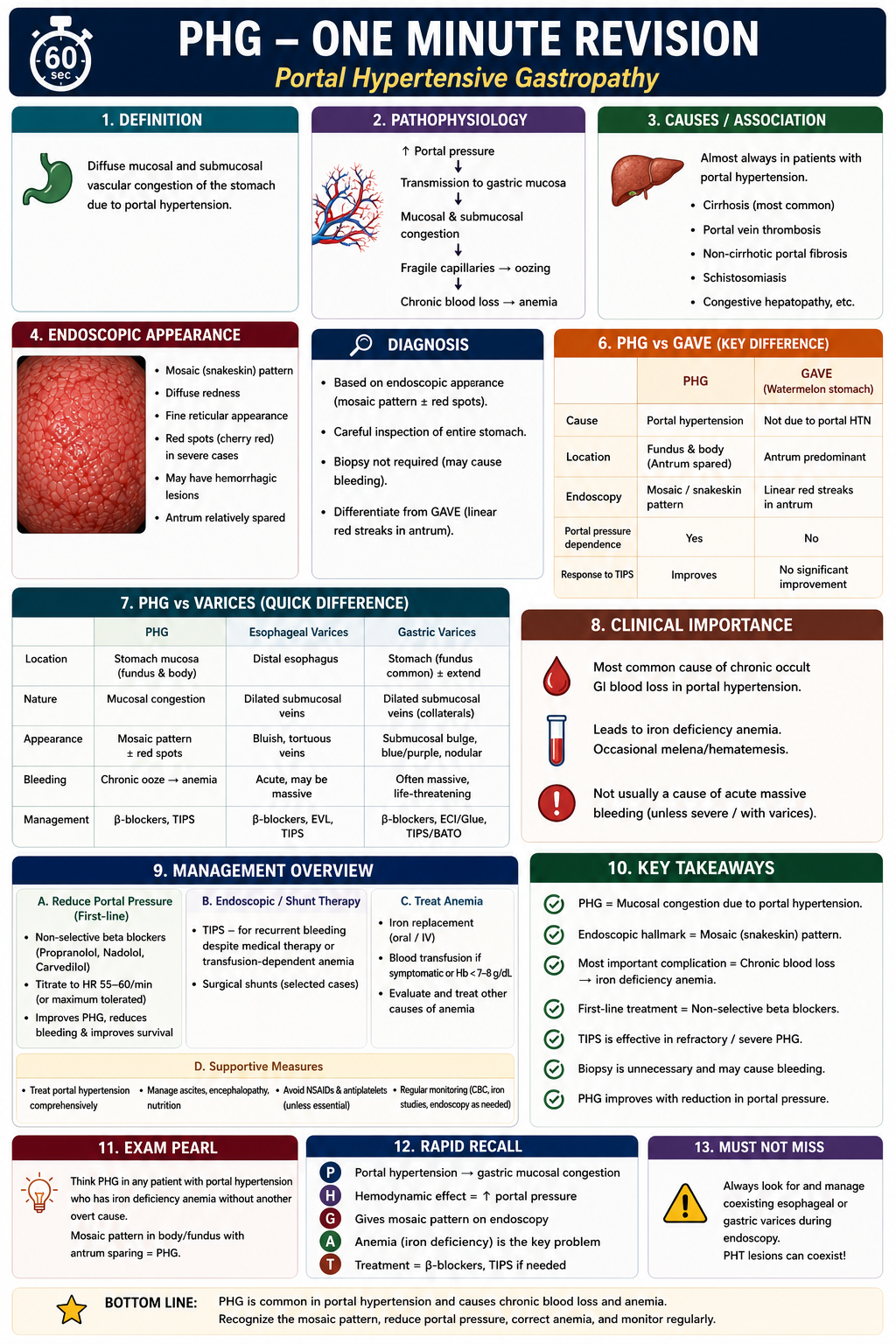
Portal hypertensive gastropathy is a gastric mucosal abnormality caused by portal hypertension, resulting in characteristic vascular congestion and a mosaic appearance on endoscopy. It is a complication of portal hypertension, not a primary gastric disease.
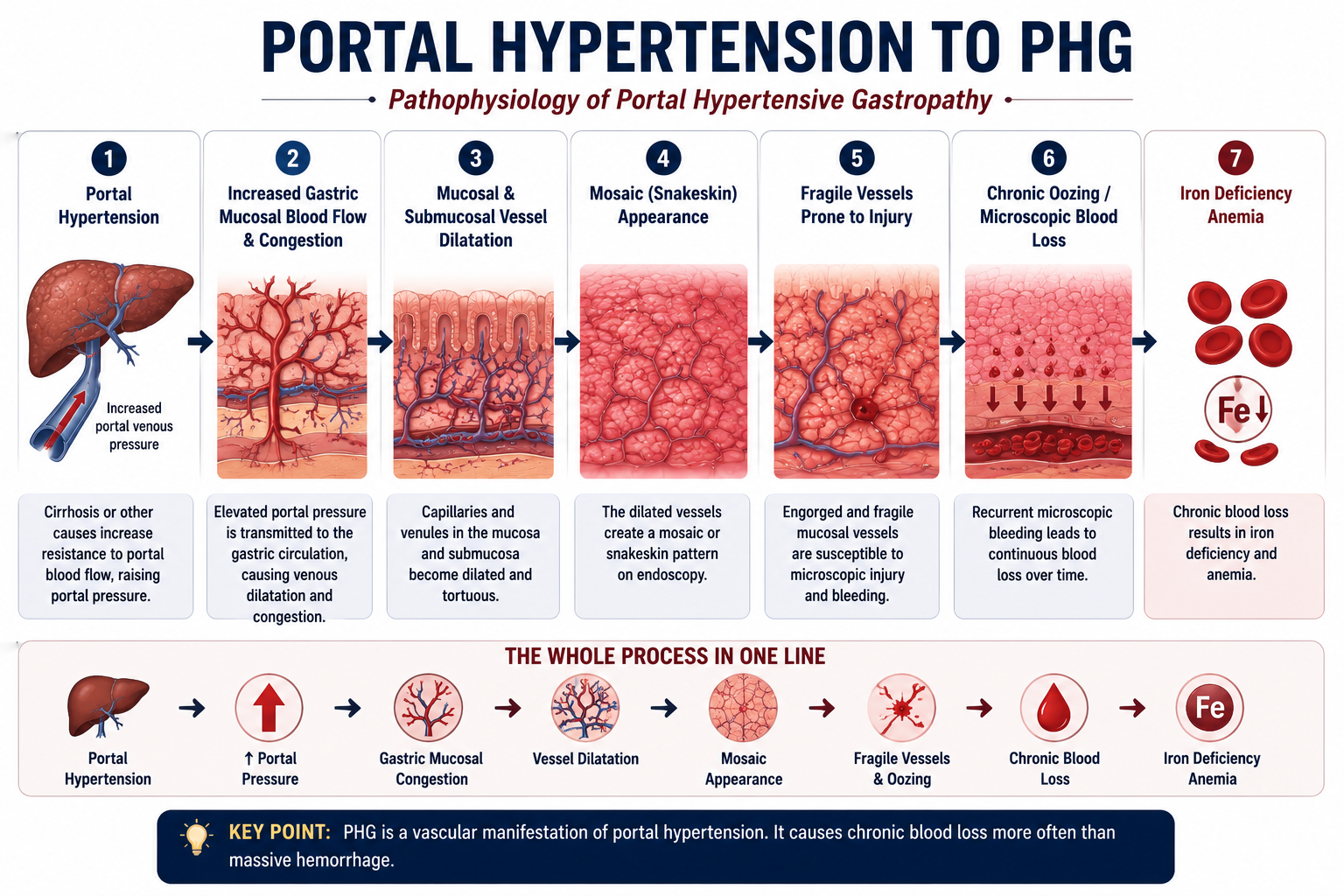
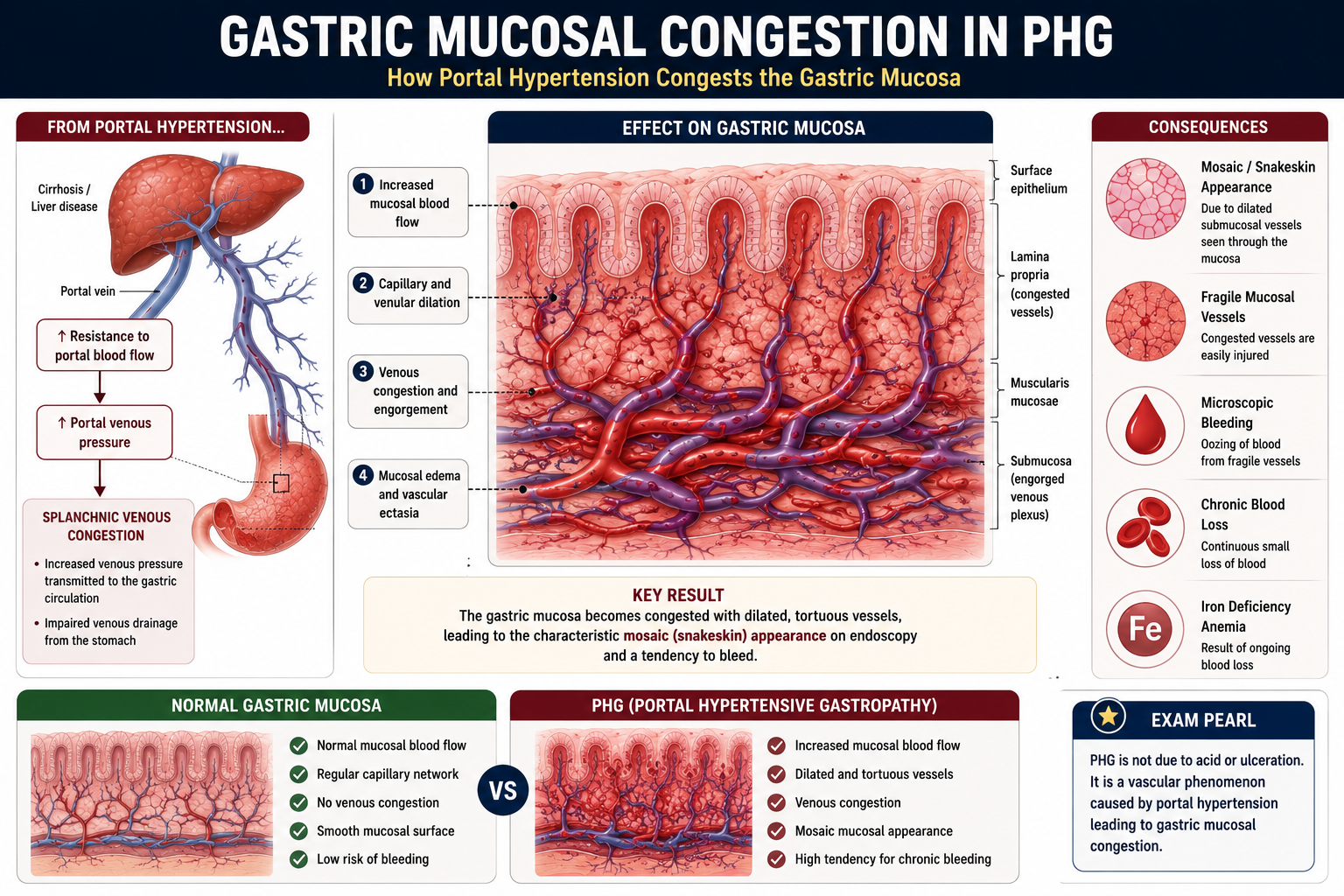
PHG occurs because the elevated pressure in the portal venous system is transmitted to the gastric mucosal circulation. This raises pressure within the small vessels of the gastric wall, causing vascular congestion, dilation of mucosal and submucosal vessels, and structural fragility that predisposes to bleeding.
PHG is one of the most common endoscopic manifestations of portal hypertension. It is reported in a large proportion of patients with cirrhosis undergoing endoscopy, especially when portal hypertension is advanced. The exact prevalence varies between studies, but the important teaching point is simple: PHG becomes more likely and more severe as portal pressure rises.
Pathophysiology of PHG
The pathophysiology of PHG flows directly from the haemodynamic consequences of portal hypertension. The key sequence is straightforward once you understand how elevated portal pressure propagates backwards through the gastric vasculature.
PHG is fundamentally a vascular consequence of portal hypertension. The gastric mucosa itself is not primarily diseased — it is damaged by the sustained increase in venous pressure transmitted from the portal system. This is why reducing portal pressure (with beta blockers or TIPS) improves PHG.
Why Does Portal Hypertension Affect the Stomach?
The stomach receives blood through the left gastric vein and short gastric veins, which drain into the portal system. When portal pressure rises, this venous drainage is impeded, and back-pressure builds up within the gastric mucosal vasculature.
Several specific changes result:
- Increased gastric mucosal blood flow — paradoxically, despite elevated venous pressure, total mucosal blood flow increases due to hyperdynamic circulation in portal hypertension
- Capillary dilation — small vessels within the mucosa become dilated and tortuous
- Microvascular abnormalities — vessel walls become structurally abnormal, reducing their integrity
- Increased susceptibility to injury — congested fragile vessels are more easily traumatised by normal gastric peristalsis and acid exposure
PHG is part of the broader hyperdynamic circulatory state of portal hypertension. Increased splanchnic blood flow and elevated portal pressure combine to overload the gastric mucosal vasculature.
Endoscopic Appearance of PHG
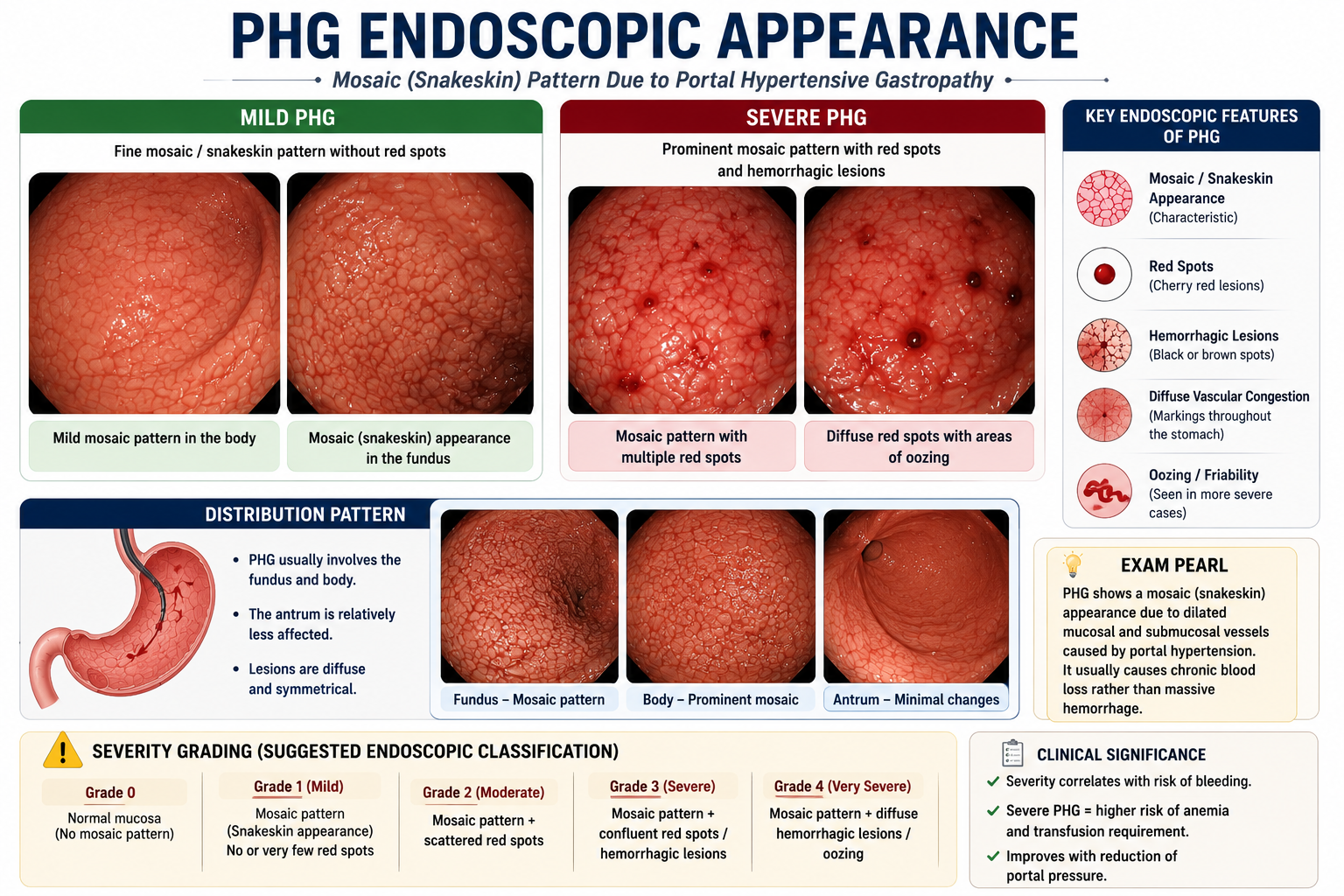
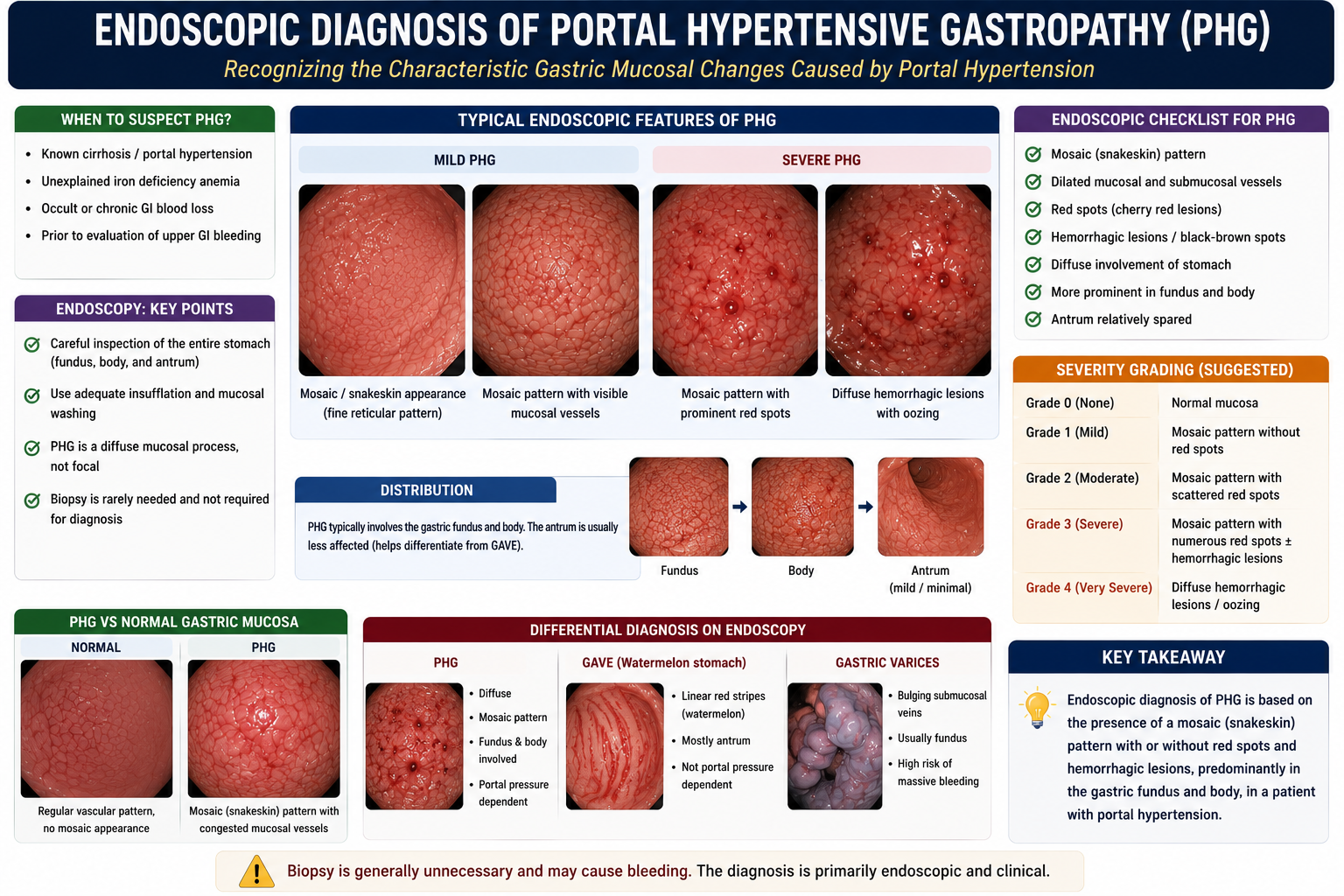
PHG is diagnosed endoscopically. Its appearance is characteristic and graded as mild or severe based on the pattern of mucosal changes visible on endoscopy.
Mild PHG
Mild PHG has a characteristic mosaic pattern — a reticular network of white or pale lines separating areas of pink mucosa, producing a snakeskin or chicken-wire appearance. This reflects dilated submucosal vessels seen through the mucosa.
- Mosaic (snakeskin) appearance — pale reticulate network
- Fine reticular markings throughout the gastric fundus and body
- No active bleeding or red spots
Severe PHG
Severe PHG has additional vascular lesions superimposed on the mosaic background, indicating more advanced mucosal fragility and higher bleeding risk.
- Red spots — punctate red marks on the mosaic background
- Cherry-red lesions — larger discrete red areas
- Diffuse haemorrhagic lesions — extensive mucosal bleeding
- Active oozing in severe cases
| Feature | Mild PHG | Severe PHG |
|---|---|---|
| Mosaic pattern | Present | Present |
| Red spots | Absent | Common |
| Cherry-red lesions | Absent | May be present |
| Active bleeding | Rare | Possible |
| Bleeding risk | Low | Higher |
The mosaic (snakeskin) pattern is the hallmark endoscopic finding of PHG. Severity correlates with bleeding risk — red spots and cherry-red lesions indicate severe PHG with higher risk of significant blood loss.
How Does PHG Cause Anaemia?
PHG is an important cause of iron deficiency anaemia in patients with cirrhosis. Unlike gastric varices, which typically cause dramatic acute haemorrhage, PHG most often causes slow, chronic, microscopic blood loss that cumulatively depletes iron stores.
This explains the classic link between PHG and iron deficiency anemia: repeated microscopic PHG bleeding slowly depletes iron stores without the dramatic presentation of variceal rupture.
PHG more commonly causes chronic occult blood loss than massive haemorrhage. In a cirrhotic patient presenting with unexplained iron deficiency anaemia and a positive faecal occult blood test, PHG should be in the differential alongside peptic ulcer disease and colorectal pathology.
Clinical Presentation
Most patients with PHG already have known cirrhosis and portal hypertension. PHG is often found incidentally on surveillance endoscopy or investigated because of unexplained anaemia.
Common Presentation
- Known cirrhosis with portal hypertension
- Iron deficiency anaemia — often progressive, requiring repeated iron supplementation or transfusions
- Positive faecal occult blood test — often the first clue to ongoing gastrointestinal blood loss
- Symptoms of anaemia: fatigue, reduced exercise tolerance, pallor, dizziness
Less Common
- Acute upper GI bleeding — less dramatic than variceal haemorrhage but can occur in severe PHG
- Melaena — if bleeding is sufficient
In a cirrhotic patient with unexplained iron deficiency anaemia — especially one who has required multiple iron infusions or transfusions — PHG should be considered and upper GI endoscopy performed. The mosaic appearance on endoscopy is diagnostic.
Diagnosis
PHG is primarily an endoscopic diagnosis. There are no specific blood tests or imaging findings that establish the diagnosis — it is the characteristic mucosal appearance on upper GI endoscopy that confirms PHG.
Typical endoscopic findings:
- Mosaic (snakeskin) appearance — the defining feature
- Fine reticular pale markings separating pink mucosal areas
- Red spots or cherry-red lesions in severe disease
- Changes most prominent in the gastric fundus and body (not confined to antrum)
- Diffuse distribution distinguishes PHG from GAVE (which is antrum-predominant)
PHG is distributed diffusely in the gastric fundus and body. GAVE (gastric antral vascular ectasia) is confined to the antrum with a watermelon-stripe pattern. Location on endoscopy is a key differentiator.
The phrase mosaic stomach appearance is often used to describe the endoscopic pattern of PHG. It is essentially the same concept as the snakeskin gastric mucosa seen in portal hypertensive gastropathy — both terms refer to the same reticular vascular pattern visible on endoscopy.
PHG vs GAVE
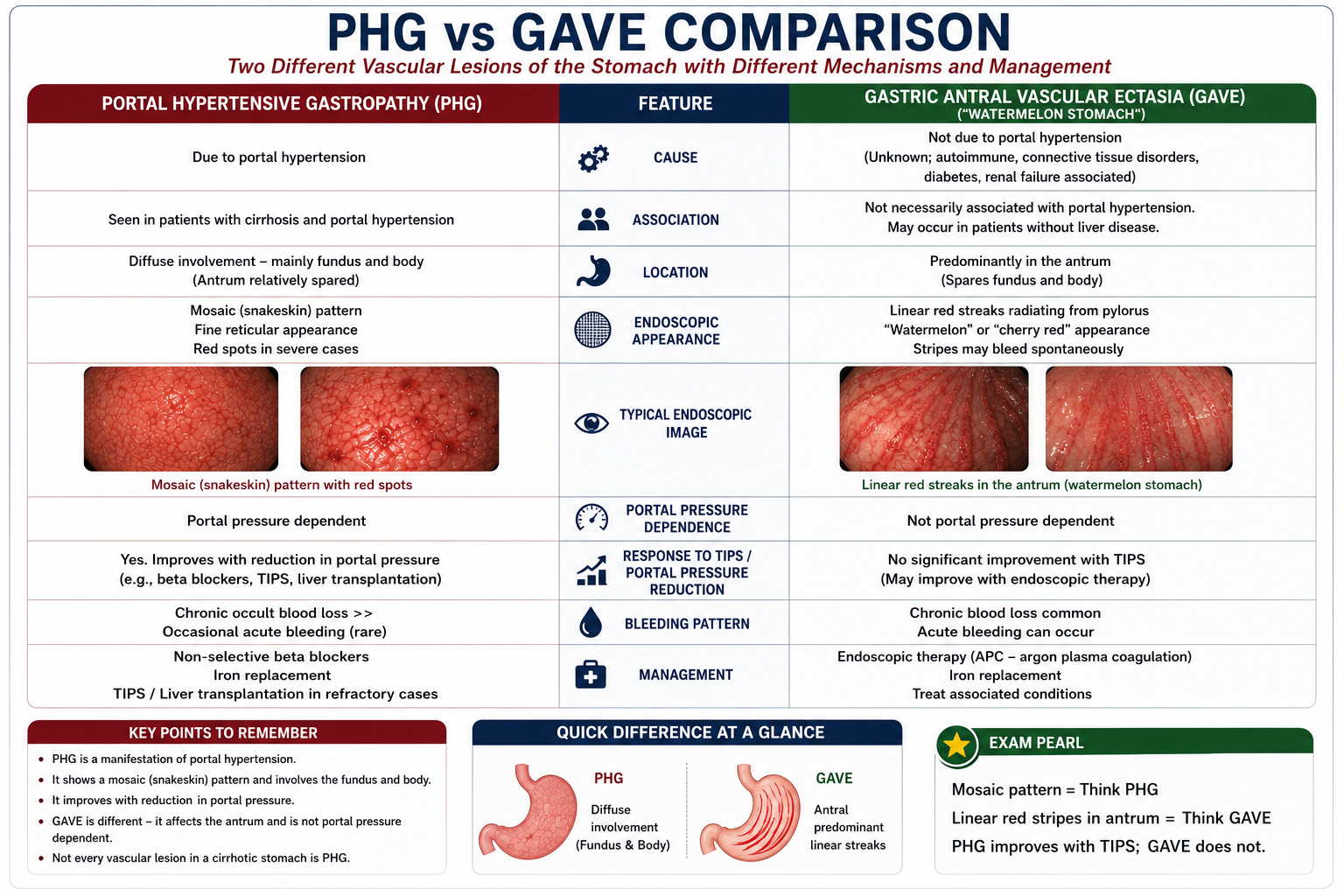
Distinguishing PHG from gastric antral vascular ectasia (GAVE) is one of the most important — and commonly examined — differentials in hepatology endoscopy.
PHG
- Caused by portal hypertension
- Diffuse: fundus and body
- Mosaic snakeskin pattern
- Portal pressure dependent
- Improves with TIPS
- Responds to beta blockers
GAVE
- Different mechanism (not portal pressure)
- Confined to antrum
- Watermelon stripes (linear red stripes)
- Not portal pressure dependent
- Does not improve with TIPS
- Treated with endoscopic ablation
| Feature | PHG | GAVE |
|---|---|---|
| Cause | Portal hypertension | Different mechanism (uncertain, not portal pressure) |
| Location | Diffuse — fundus and body | Antrum only |
| Endoscopic appearance | Mosaic/snakeskin pattern | Watermelon stripes (linear red stripes radiating from pylorus) |
| Portal pressure dependent | Yes | No |
| Responds to TIPS | Yes — portal pressure reduction improves PHG | Usually no |
| Management | Beta blockers, TIPS if refractory | Endoscopic ablation (argon plasma coagulation) |
Not every vascular lesion in a cirrhotic stomach is PHG. GAVE can also occur in cirrhosis but is not portal pressure dependent — so TIPS will not help GAVE. Getting this distinction wrong changes management entirely.
PHG = diffuse mosaic mucosa + chronic occult blood loss
GAVE = antral watermelon stripes + endoscopic ablation treatment
Gastric varices = large submucosal veins + risk of massive acute bleeding
PHG vs Gastric Varices
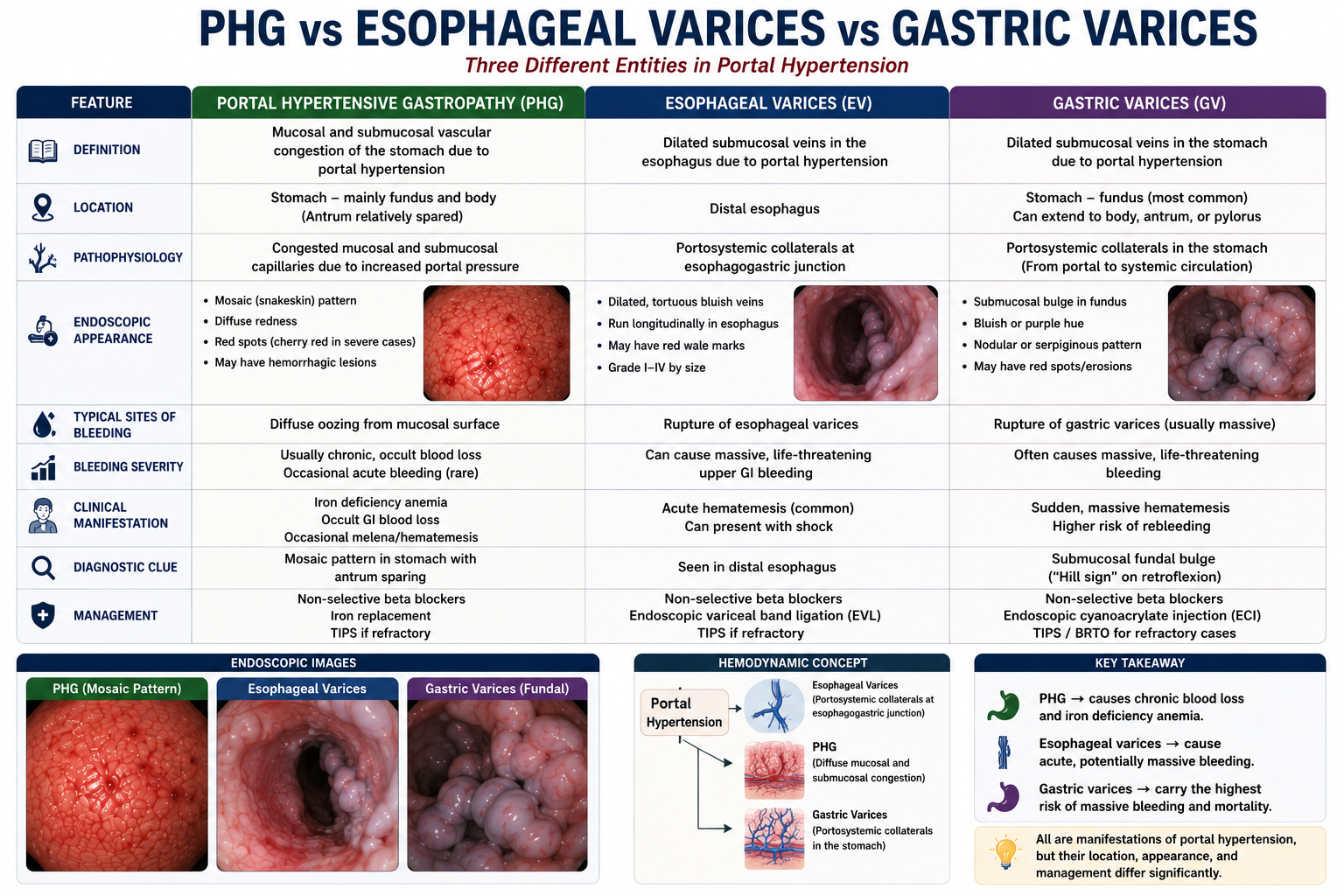
PHG and gastric varices are both complications of portal hypertension but differ fundamentally in their nature, bleeding pattern and management.
| Feature | PHG | Gastric Varices |
|---|---|---|
| Nature of lesion | Mucosal vascular congestion — diffuse capillary-level changes | Large dilated veins in the gastric wall |
| Bleeding pattern | Chronic, occult, microscopic — iron deficiency anaemia | Massive acute haemorrhage — life-threatening |
| Endoscopy | Mosaic/snakeskin mucosal pattern | Large submucosal bulging variceal columns |
| Acute management | Beta blockers, iron replacement, TIPS if severe | Vasoactive drugs, band ligation/glue injection, TIPS |
Gastric varices bleed acutely and massively — they are an emergency with high mortality. PHG bleeds chronically and slowly — it is managed electively. The distinction affects urgency and approach completely.
Management of PHG
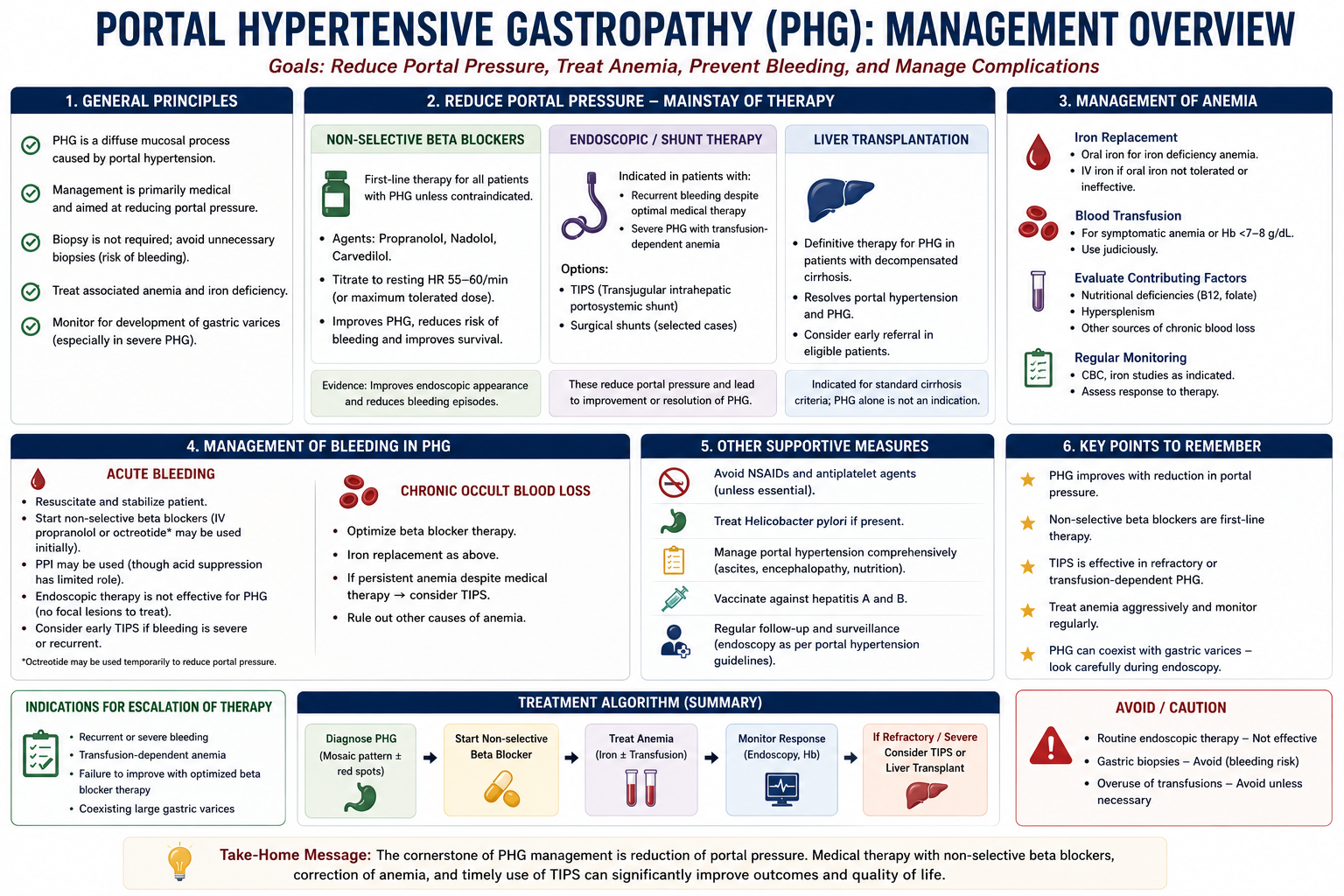
Management of PHG targets the two key problems: the underlying elevated portal pressure driving the gastropathy, and the anaemia resulting from chronic blood loss.
1. Iron Replacement
Iron deficiency anaemia from chronic PHG-related blood loss is treated with iron supplementation — oral iron for mild deficiency, intravenous iron for moderate-to-severe deficiency or when oral iron is poorly tolerated. Blood transfusion may be required for symptomatic severe anaemia.
2. Non-Selective Beta Blockers
Non-selective beta blockers — propranolol, nadolol or carvedilol — are the first-line pharmacological treatment for PHG. They reduce portal pressure by decreasing cardiac output and splanchnic vasoconstriction, thereby reducing gastric mucosal congestion and bleeding risk.
3. Endoscopic Therapy
Endoscopic therapy has a limited role in PHG compared with varices, because PHG involves diffuse mucosal changes rather than discrete treatable lesions. It may be used for specific bleeding points but cannot address the underlying mucosal disease.
Therefore, portal hypertensive gastropathy treatment is based on reducing portal pressure and correcting anaemia, rather than simply applying focal endoscopic therapy.
4. TIPS
Transjugular intrahepatic portosystemic shunt (TIPS) is used for refractory PHG bleeding that does not respond to beta blockers and iron replacement. By directly reducing portal pressure, TIPS relieves the venous congestion driving PHG and leads to improvement in the gastropathy.
PHG is portal pressure dependent — reducing portal pressure directly reduces the mucosal congestion driving PHG. GAVE is not portal pressure dependent, so TIPS does not improve it. This distinction explains why TIPS is used for refractory PHG but not for GAVE.
Complications
PHG is a chronic condition and its complications reflect persistent blood loss and progressive liver disease.
Severe PHG often reflects more severe portal hypertension and more advanced liver disease. Therefore, marked PHG with recurrent anaemia should not be treated as an isolated gastric problem. It should prompt careful reassessment of the patient's overall cirrhosis severity, portal hypertension control, nutritional status and transplant suitability where appropriate.
- Iron deficiency anaemia — the most common complication; may be severe and require repeated transfusions
- Recurrent transfusion requirement — patients with severe PHG may become transfusion dependent
- Acute upper GI bleeding — less common than with varices but can occur, particularly in severe PHG
- Reduced quality of life — fatigue, reduced exercise tolerance and frequent hospital attendances
PHG severity correlates with portal pressure and the severity of underlying liver disease. Patients with more advanced cirrhosis (high Child-Pugh or MELD scores) are more likely to have severe PHG and transfusion-dependent anaemia.
High-Yield Exam Pearls
PHG = complication of portal hypertension
Mosaic snakeskin = hallmark endoscopic finding
Chronic occult bleeding → iron deficiency anaemia
PHG is portal pressure dependent — TIPS improves it
GAVE = antrum, watermelon stripes, NOT portal pressure dependent
Gastric varices = massive acute bleeding; PHG = slow chronic bleeding
Beta blockers = first-line PHG treatment
- PHG is caused by portal hypertension — it is a vascular consequence of elevated portal pressure, not a primary gastric disease.
- Mosaic appearance — the characteristic snakeskin or chicken-wire pattern on endoscopy; this is the hallmark finding you need to recognise.
- Chronic not acute — PHG causes chronic occult blood loss and iron deficiency anaemia more often than acute massive haemorrhage.
- PHG improves when portal pressure falls — this is why beta blockers and TIPS both work for PHG.
- PHG vs GAVE — the most commonly examined distinction. PHG: diffuse, mosaic, portal pressure dependent, TIPS works. GAVE: antrum only, watermelon stripes, NOT portal pressure dependent, TIPS doesn't work.
- PHG vs gastric varices — varices are dilated veins causing massive acute bleeding; PHG involves mucosal vascular congestion causing slow chronic loss.
- TIPS for refractory PHG — reducing portal pressure relieves mucosal congestion and improves gastropathy.
Key Takeaways
- Portal hypertensive gastropathy is a gastric mucosal abnormality caused by portal hypertension — not a primary gastric disease
- Elevated portal pressure transmits to the gastric mucosal vasculature, causing congestion, capillary dilation and structural fragility
- The hallmark endoscopic finding is the mosaic (snakeskin) pattern of the gastric fundus and body
- Severe PHG has additional red spots and cherry-red lesions indicating higher bleeding risk
- PHG causes chronic occult blood loss leading to iron deficiency anaemia more commonly than acute haemorrhage
- Diagnosis is endoscopic — mosaic pattern diffusely distributed in the fundus and body
- PHG is portal pressure dependent — its severity correlates with the degree of portal hypertension
- PHG differs from GAVE: GAVE is in the antrum, has a watermelon stripe pattern, and is not portal pressure dependent
- PHG differs from gastric varices: varices are dilated veins causing acute massive bleeding; PHG causes slow chronic loss
- Management: iron replacement for anaemia; non-selective beta blockers to reduce portal pressure; TIPS for refractory cases
- PHG improves when portal pressure is reduced — unlike GAVE, which does not respond to TIPS
Frequently Asked Questions
One-Minute PHG Revision
References
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460.
- Garcia-Tsao G, Bosch J. Management of varices and variceal hemorrhage in cirrhosis. N Engl J Med. 2010;362(9):823–832.
- Thuluvath PJ, Yoo HY. Portal hypertensive gastropathy. Am J Gastroenterol. 2002;97(12):2973–2978.
- Cubillas R, Rockey DC. Portal hypertensive gastropathy: a review. Liver Int. 2010;30(8):1094–1102.
- Burak KW, Lee SS, Beck PL. Portal hypertensive gastropathy and gastric antral vascular ectasia (GAVE) syndrome. Gut. 2001;49(6):866–872.
- De Franchis R; Baveno VI Faculty. Expanding consensus in portal hypertension: report of the Baveno VI Consensus Workshop. J Hepatol. 2015;63(3):743–752.
PHG is the chronic gastric mucosal bleeding complication of portal hypertension. Remember the triad: portal hypertension + mosaic gastric mucosa + iron deficiency anaemia.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist hepatological input when managing patients.