Many students understand ascites but struggle to explain why a patient with cirrhosis develops a large pleural effusion.
Hepatic hydrothorax is not primarily a lung disease. It represents movement of ascitic fluid from the abdominal cavity into the pleural cavity through defects in the diaphragm.
Understanding hepatic hydrothorax requires understanding portal hypertension and ascites — because hydrothorax is best understood as an extension of ascites into the chest.
Portal hypertension → ascites → SBP
Portal hypertension → ascites → hepatic hydrothorax → spontaneous bacterial empyema
Portal hypertension → varices → variceal bleeding
Portal hypertension → PHG, HE, HRS
Learning Objectives
- Define hepatic hydrothorax and distinguish it from primary lung or cardiac disease
- Explain the pathophysiology: how ascitic fluid reaches the pleural cavity through diaphragmatic defects
- Explain why hepatic hydrothorax is usually right-sided
- Understand why hydrothorax can occur without clinically obvious ascites
- Interpret pleural fluid findings and distinguish hydrothorax from other effusions
- Outline the management approach from salt restriction to TIPS and transplantation
- Explain why routine chest drain placement is dangerous in hepatic hydrothorax
- Recognise spontaneous bacterial empyema as a complication of hydrothorax
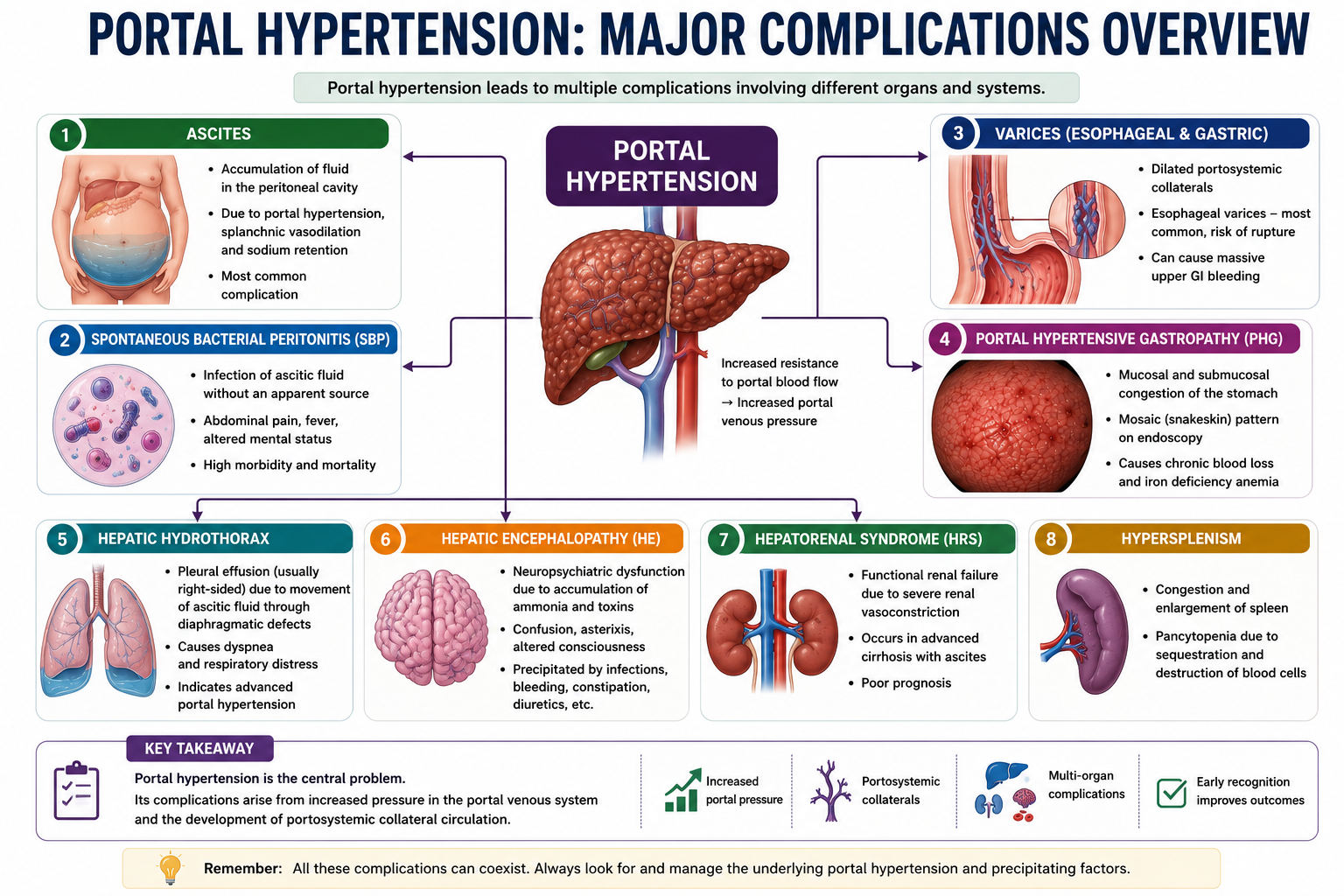
Where Hepatic Hydrothorax Fits in Portal Hypertension
Portal hypertension produces multiple complications through different mechanisms. Hepatic hydrothorax shares its origin with ascites — both arise from the same haemodynamic disturbances — but hydrothorax represents the subset of fluid that crosses the diaphragm into the chest.
Hydrothorax is best understood as an extension of ascites into the chest. It is not a separate disease process — it shares the same haemodynamic origin as ascites. Treating the portal hypertension and reducing ascites formation is therefore the correct treatment target.
What Is Hepatic Hydrothorax?
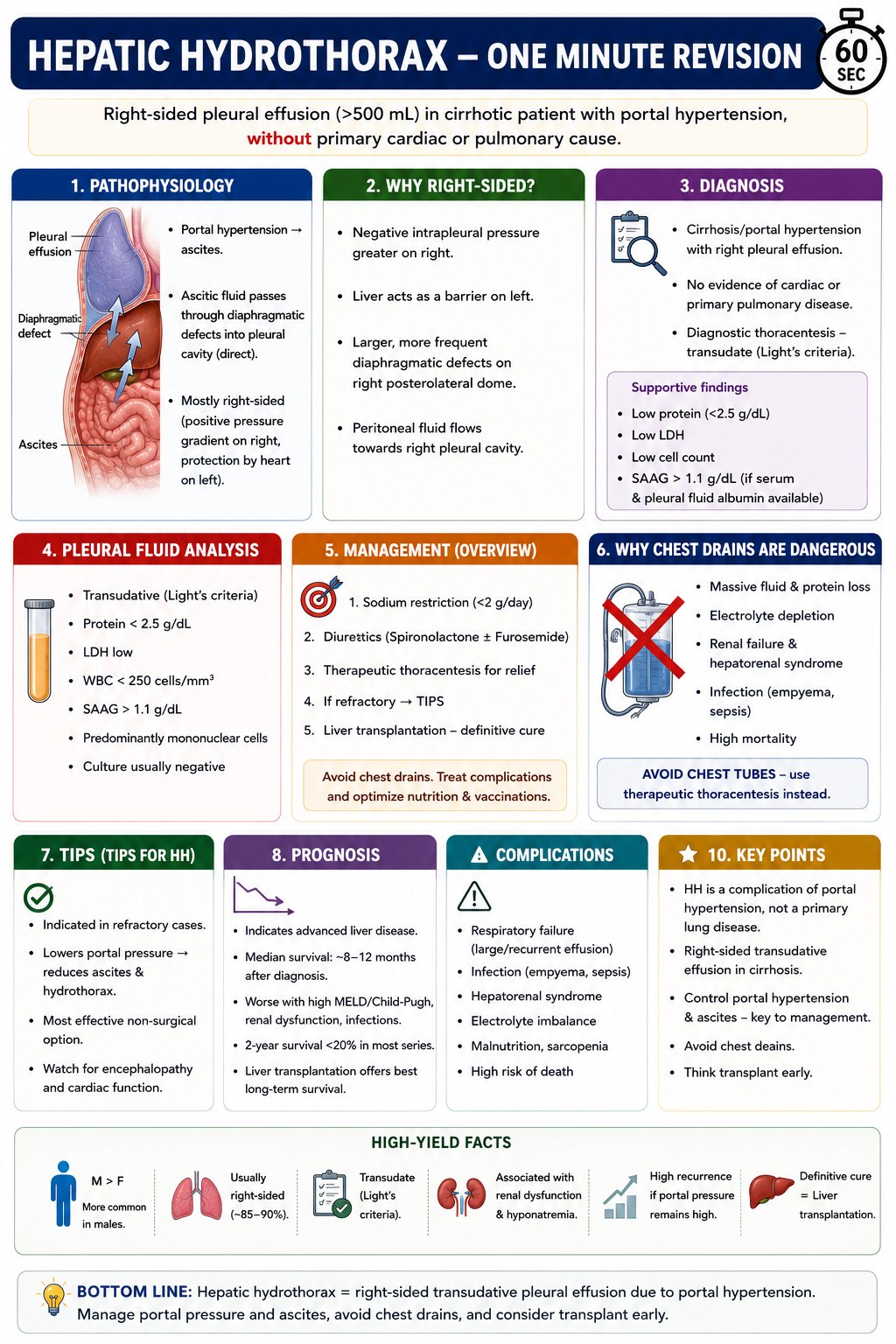
Hepatic hydrothorax is a pleural effusion occurring in patients with portal hypertension and cirrhosis in the absence of primary cardiac or pulmonary disease. It is a complication of portal hypertension, not a primary chest condition.
Hepatic hydrothorax develops in approximately 5–12% of patients with cirrhosis and portal hypertension. Although it is less common than ascites, its presence usually indicates advanced portal hypertension and decompensated liver disease.
The term distinguishes this type of pleural effusion — driven by portal hypertension and diaphragmatic fluid transfer — from effusions caused by heart failure, pneumonia, malignancy or primary pulmonary disease. The distinction is clinically important because management targets the liver disease, not the chest.
Hepatic hydrothorax affects approximately 5–12% of patients with cirrhosis. It is more common in patients with advanced portal hypertension and large-volume ascites, though it can also develop in patients with relatively modest ascites when diaphragmatic defects are particularly efficient at transferring fluid.

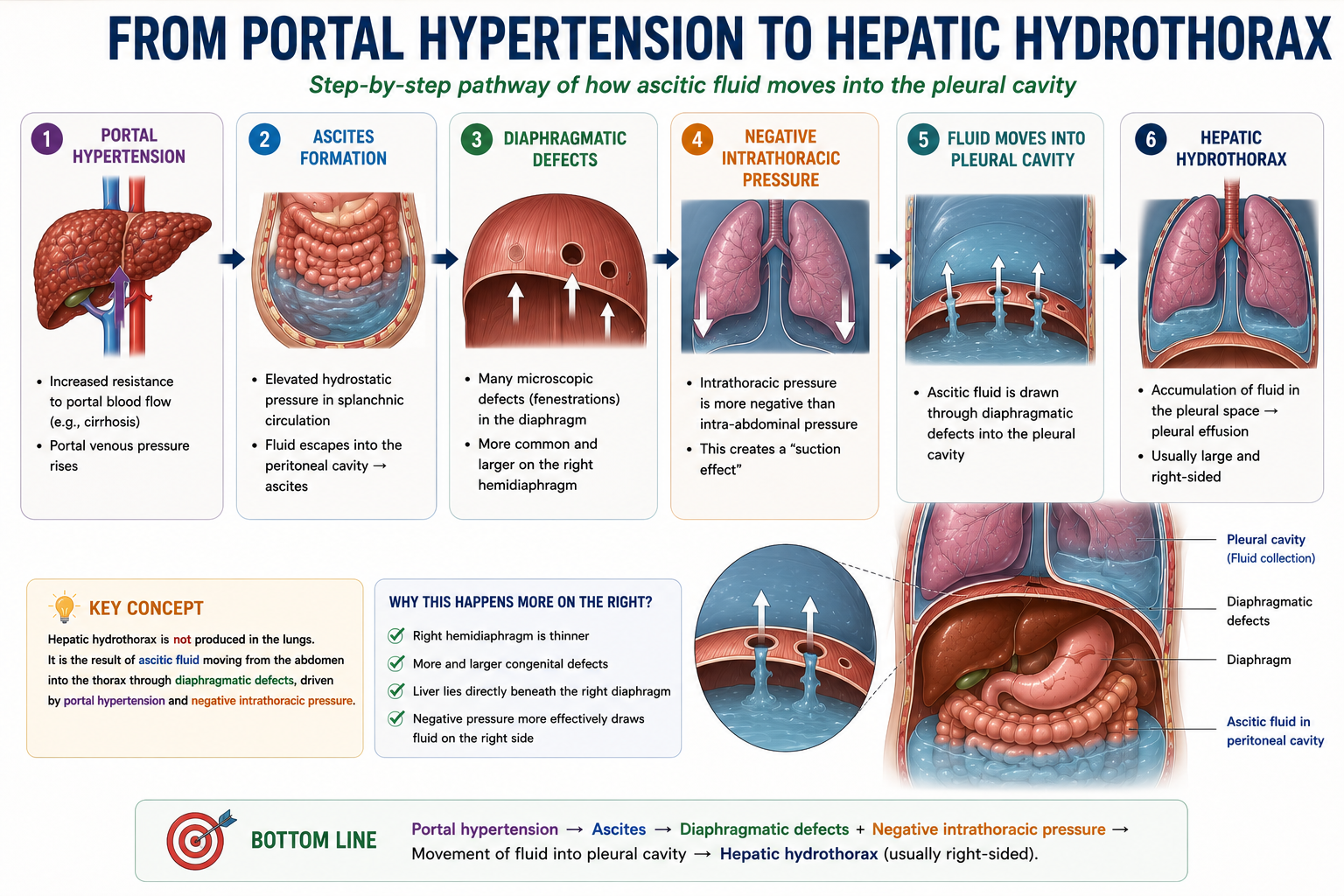
Pathophysiology of Hepatic Hydrothorax
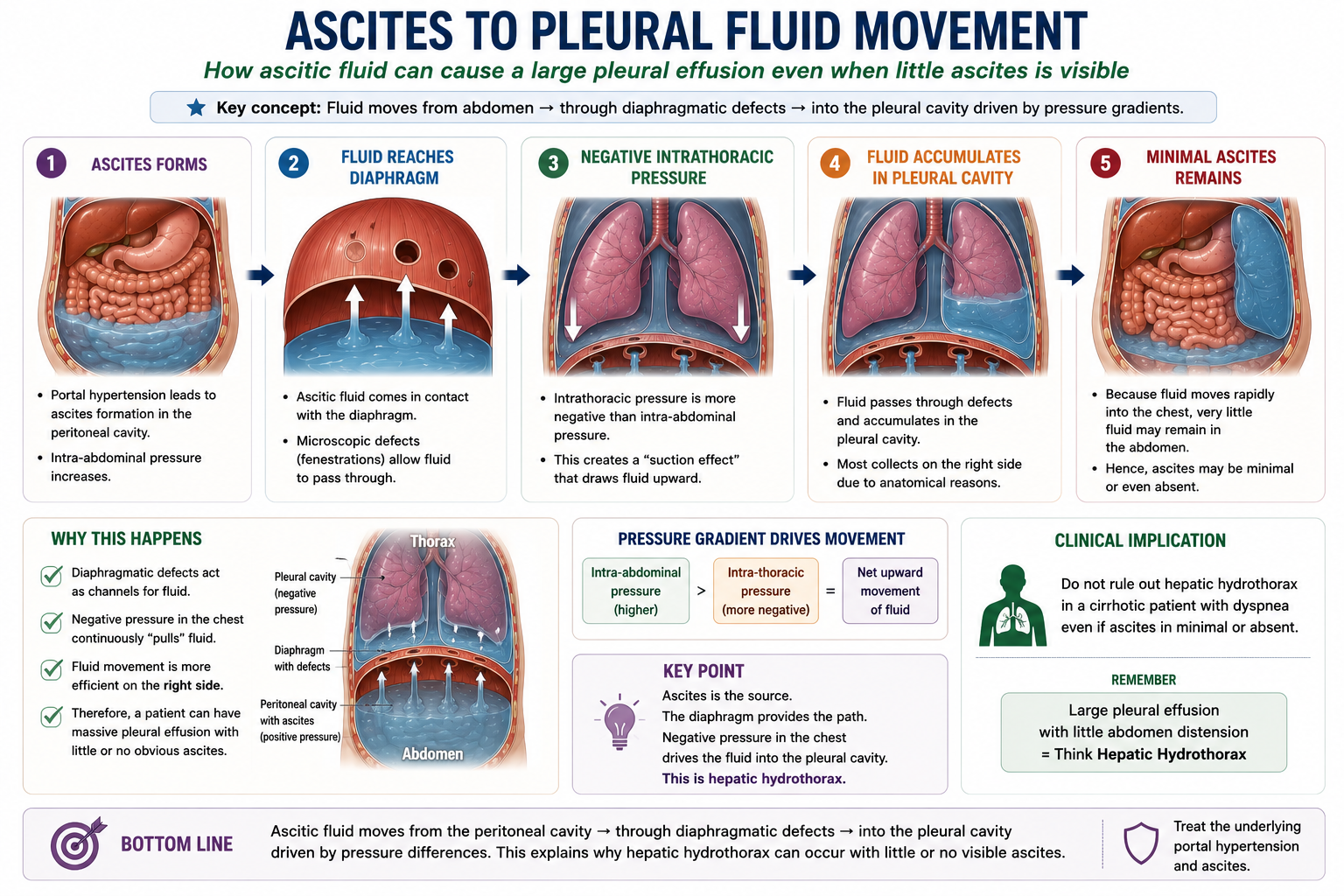
The pathophysiology of hepatic hydrothorax is mechanically straightforward once the two key drivers are understood: the presence of ascitic fluid in the abdomen, and a pressure gradient that favours its movement into the chest.
The diaphragm is not a perfect barrier. Small anatomical defects — blebs, pores or fenestrations — exist in many people. In healthy individuals these defects are inconsequential. In patients with cirrhosis and ascites, the elevated intra-abdominal pressure combined with the physiologically negative intrathoracic pressure creates a persistent one-way pressure gradient that drives ascitic fluid upward through these defects into the pleural cavity.
Hydrothorax is not created inside the chest. It originates in the abdomen. The pleural space simply acts as a reservoir for fluid that has moved upward from the peritoneal cavity through diaphragmatic defects under negative intrathoracic pressure.
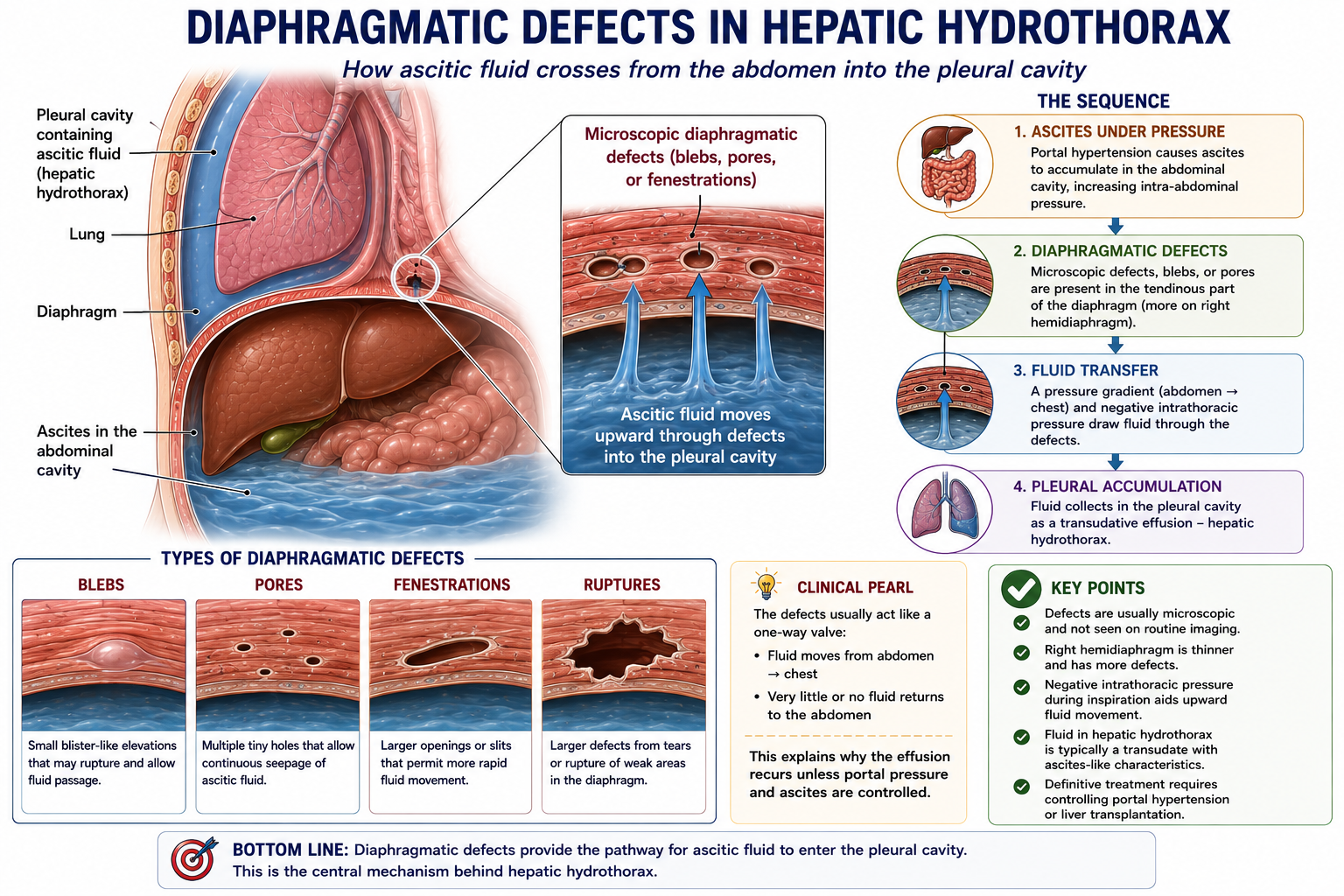
How Does Fluid Cross the Diaphragm?
The diaphragm normally separates the abdominal cavity from the pleural cavity. In hepatic hydrothorax, this barrier becomes functionally incomplete because of small defects, blebs, pores or fenestrations.
These defects may be microscopic and invisible on routine imaging. However, when ascites is present, the pressure gradient between the abdomen and chest allows fluid to move through them repeatedly.
The pleural effusion is not produced by the pleura itself. The pleural cavity simply receives ascitic fluid that crosses through diaphragmatic defects in hepatic hydrothorax. This is why the fluid usually has transudative, ascites-like characteristics.
Understanding diaphragmatic defects in hepatic hydrothorax explains why the pleural effusion keeps recurring unless portal pressure and ascites formation are controlled.
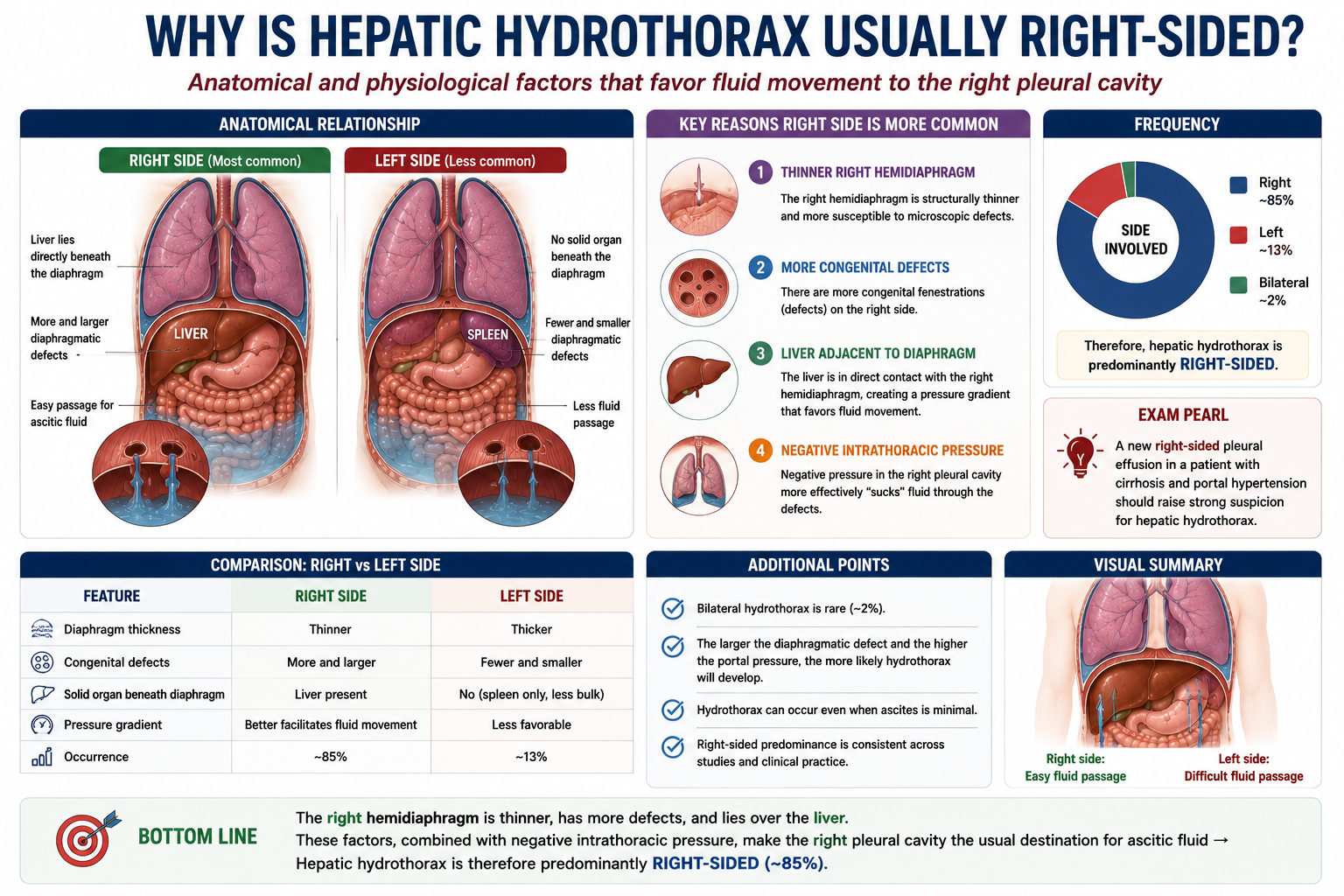
Why Is Hepatic Hydrothorax Usually Right-Sided?
The right-sided predominance of hepatic hydrothorax is one of the most frequently examined facts about this condition. Understanding the reason makes it memorable.
- The right hemidiaphragm is thinner than the left, making it structurally more prone to developing small defects
- More microscopic defects are found in the right diaphragm, providing more routes for fluid transfer
- The liver lies directly beneath the right diaphragm, which may facilitate fluid transfer due to anatomical proximity and local pressure effects
- The left diaphragm is reinforced by the pericardium, which limits the formation of defects on that side
| Side | Frequency | Reason |
|---|---|---|
| Right | ~85% | Thinner diaphragm, more defects, liver proximity |
| Left | ~13% | Less common — pericardium reinforces left diaphragm |
| Bilateral | ~2% | Defects on both sides; usually severe portal hypertension |
A right-sided pleural effusion in a cirrhotic patient should always raise suspicion of hepatic hydrothorax. It is one of the most important differential diagnoses to consider in this setting, alongside heart failure and infection.
Why Can Hydrothorax Occur With Little Ascites?
This is a conceptually important teaching point that frequently appears in examinations and clinically confuses students.
Intuitively, one might expect that hepatic hydrothorax would only develop in patients with obviously large-volume ascites. In reality, some patients with hepatic hydrothorax have surprisingly little detectable ascites.
When diaphragmatic defects are large or particularly porous, fluid moves rapidly from the peritoneal cavity into the pleural space as fast as (or faster than) it accumulates. The pleural cavity effectively acts as a continuous drain for newly formed ascitic fluid. This means that on examination or imaging, the abdomen appears to have little fluid while the chest has a large effusion.
Absence of obvious ascites does not exclude hepatic hydrothorax. In a patient with cirrhosis and a right-sided pleural effusion, the absence of clinically detectable ascites does not rule out a hepatic origin for the effusion.
Clinical Presentation
Most patients with hepatic hydrothorax already have known cirrhosis and portal hypertension. The hydrothorax presents with respiratory symptoms caused by pleural fluid compression of the lung.
Symptoms
- Dyspnoea — the most common symptom, often disproportionate to the degree of ascites visible on examination
- Dry non-productive cough — caused by diaphragmatic irritation and lung compression
- Orthopnoea — difficulty breathing when lying flat, as fluid redistributes
- Reduced exercise tolerance — progressive as effusion enlarges
Signs
- Reduced breath sounds — at the right base (or left, or bilaterally)
- Stony dull percussion note — over the effusion
- Reduced chest expansion — on the affected side
- Signs of chronic liver disease and portal hypertension may be present
In a patient with cirrhosis presenting with breathlessness and a right-sided pleural effusion, hepatic hydrothorax should be high on the differential. The history of liver disease, the right-sided predominance, and transudative pleural fluid all support the diagnosis.
Pleural Fluid Findings
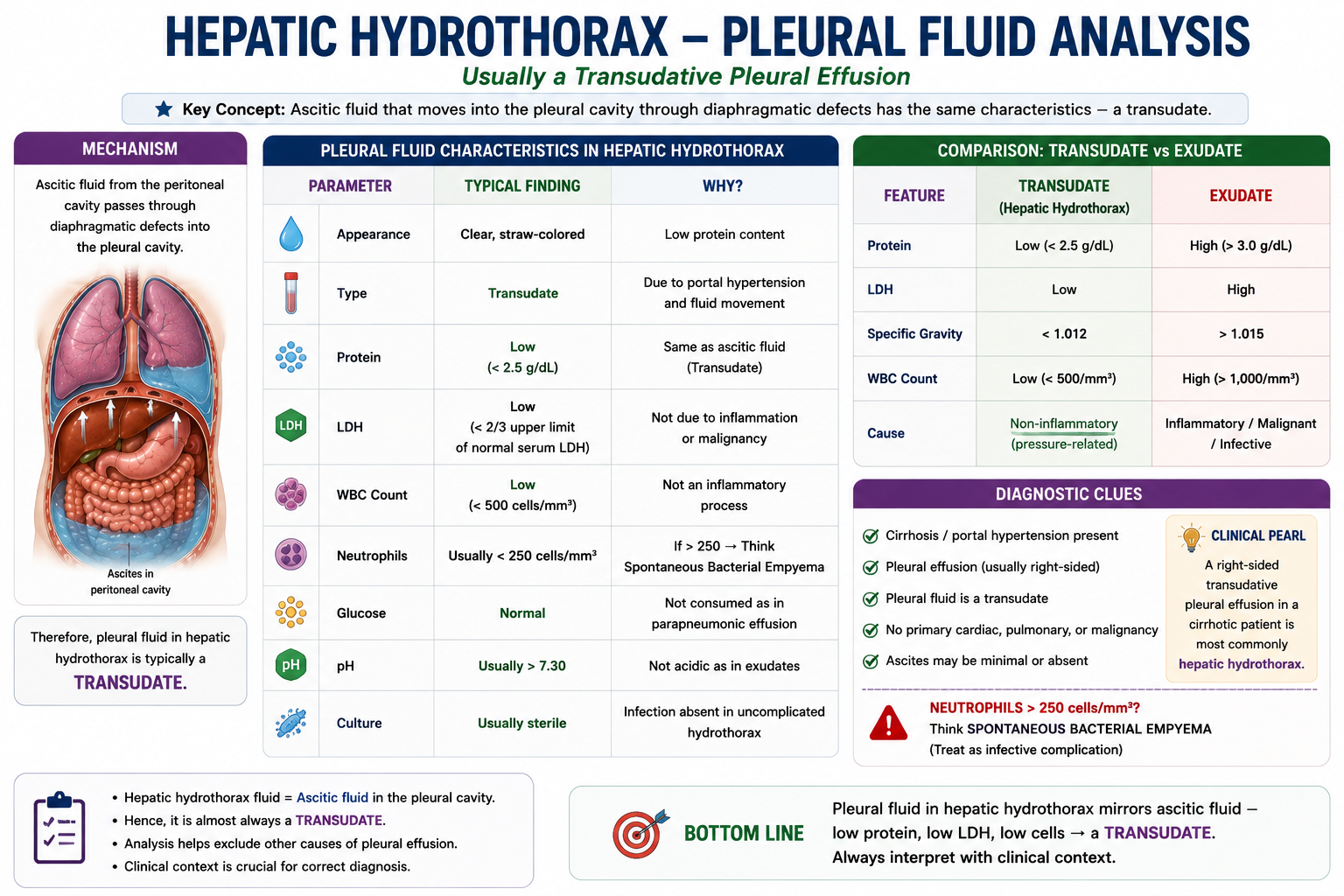
Thoracentesis (pleural aspiration) is performed to characterise the effusion and confirm the diagnosis. The pleural fluid in hepatic hydrothorax has characteristic features that reflect its origin as ascitic fluid.
| Feature | Typical Finding in Hepatic Hydrothorax |
|---|---|
| Appearance | Clear or straw-coloured (occasionally turbid if infected) |
| Type | Transudate (by Light's criteria) |
| Protein | Low |
| LDH | Low |
| White blood cells | Low (raised if infected — spontaneous bacterial empyema) |
| Gradient (serum-pleural albumin) | Typically mirrors the SAAG pattern |
Hepatic hydrothorax produces a transudative pleural effusion. The pleural fluid composition closely resembles ascitic fluid, because it originates from the same source. The detection of a transudate in a cirrhotic patient with right-sided effusion strongly supports hepatic hydrothorax.
Differential Diagnosis
Not all pleural effusions in cirrhotic patients are hepatic hydrothorax. The main differentials must be considered, particularly conditions that can coexist with cirrhosis.
| Condition | Pleural Fluid Type | Distinguishing Features |
|---|---|---|
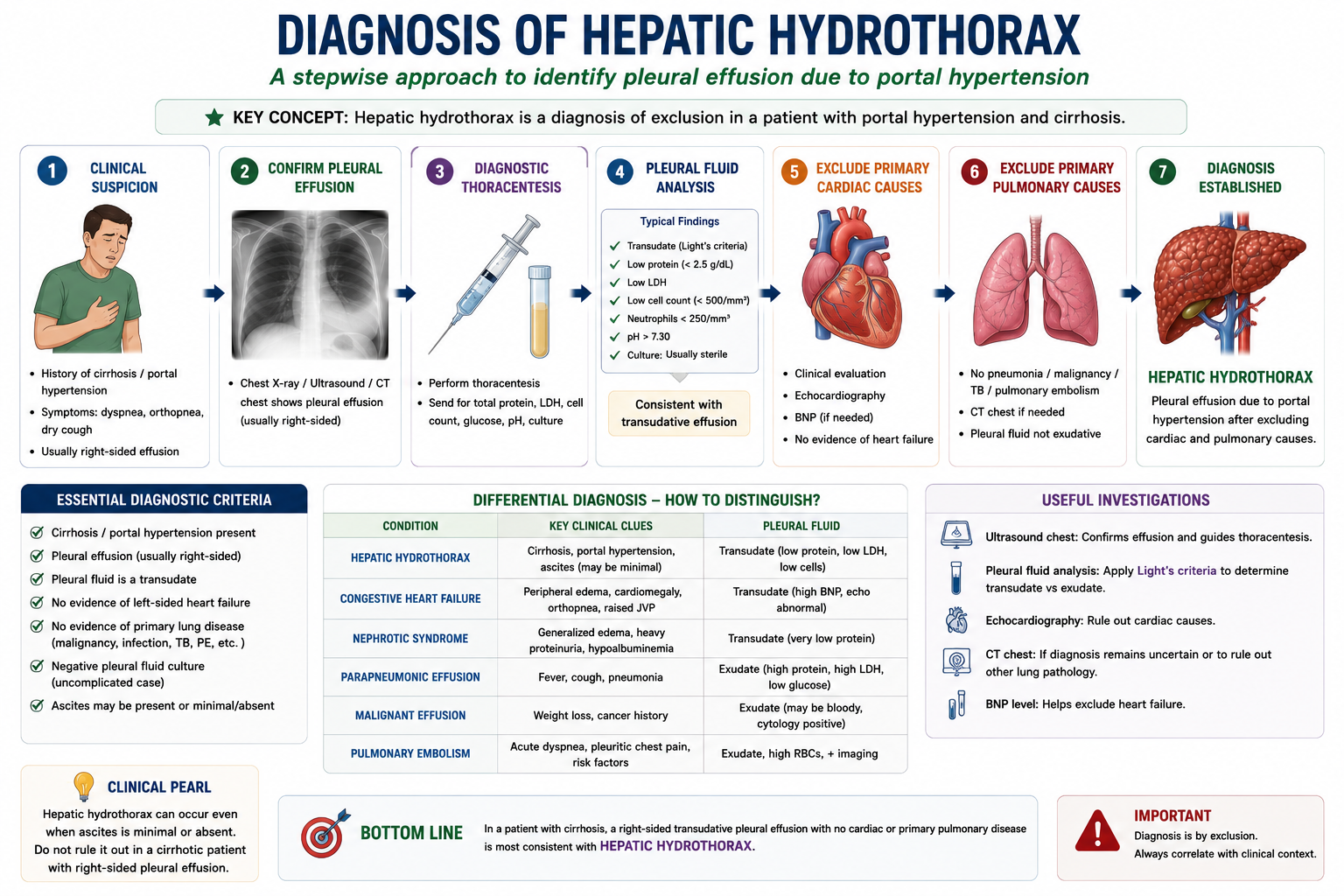
| Hepatic hydrothorax | Transudate | Cirrhosis; right-sided; resembles ascitic fluid; responds to portal pressure reduction |
| Heart failure | Transudate | Cardiac history; bilateral effusions common; JVP raised; responds to diuretics |
| Nephrotic syndrome | Transudate | Heavy proteinuria; hypoalbuminaemia; no cirrhosis required |
| Parapneumonic effusion | Exudate | Fever; pneumonia on imaging; high WBC in fluid |
| Malignant effusion | Exudate (usually) | Malignancy history; cytology positive; often left-sided or bilateral |
| Spontaneous bacterial empyema | Exudate or infected transudate | PMN >250/mm³ in pleural fluid; complication of hepatic hydrothorax |
Heart failure and hepatic hydrothorax can coexist. Always consider whether the pleural effusion can be fully explained by the liver disease or whether additional cardiac pathology needs to be excluded.
The distinction between hepatic hydrothorax vs heart failure is clinically important because both may produce transudative pleural effusions, but the treatment targets are completely different.
Hepatic Hydrothorax vs Heart Failure Effusion
| Feature | Hepatic Hydrothorax | Heart Failure Pleural Effusion |
|---|---|---|
| Main driver | Portal hypertension with ascites crossing the diaphragm | Raised systemic and pulmonary venous pressure from cardiac failure |
| Typical laterality | Usually right-sided | Often bilateral, may be right-predominant |
| Ascites | Common, but may be minimal or absent clinically | Not a defining feature |
| JVP | Usually not elevated unless cardiac disease coexists | Often elevated |
| Echocardiography | Used to exclude cardiac disease | Usually shows structural or functional cardiac abnormality |
| Treatment target | Portal pressure and ascites control | Cardiac failure management |
Both hepatic hydrothorax and heart failure can produce transudative pleural effusions. Therefore, a transudate alone does not prove hepatic hydrothorax. The diagnosis depends on the full clinical context and exclusion of cardiac causes.
Diagnosis
The diagnosis of hepatic hydrothorax is based on a combination of clinical context and pleural fluid analysis. There is no single definitive test — diagnosis is reached by establishing that the effusion is transudative, that cirrhosis and portal hypertension are present, and that primary cardiac and pulmonary causes have been excluded.
A right-sided transudative pleural effusion in a patient with cirrhosis and portal hypertension should strongly suggest hepatic hydrothorax, provided primary cardiac and pulmonary causes are excluded.
In uncertain cases, nuclear scintigraphy (radionuclide imaging after intraperitoneal injection of a tracer) can directly demonstrate fluid movement from the peritoneal to the pleural cavity through diaphragmatic defects, confirming the diagnosis.
Management of Hepatic Hydrothorax
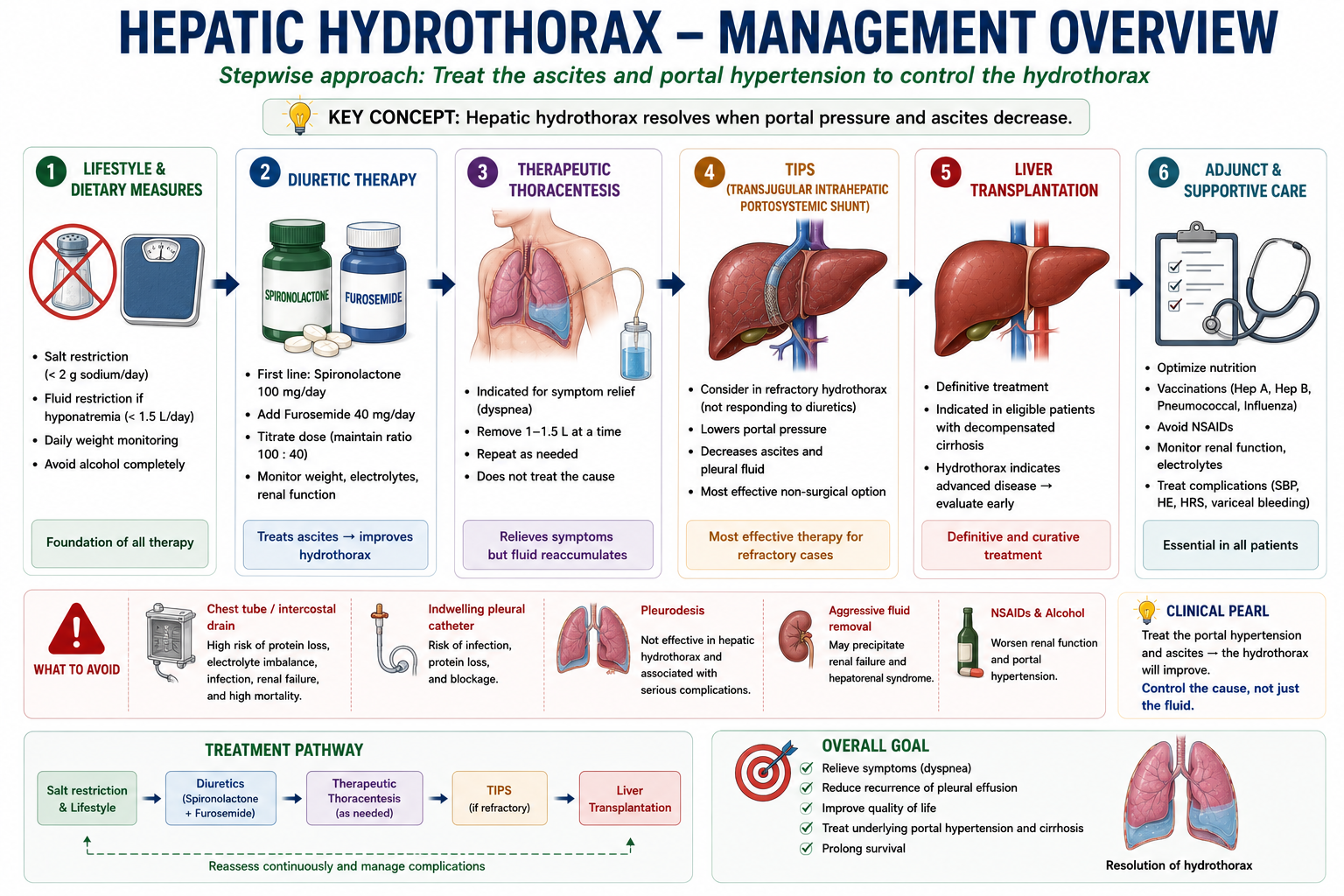
Management follows a stepwise approach that targets the underlying cause — portal hypertension and ascites formation — rather than simply draining the chest.
1. Salt Restriction
Dietary sodium restriction (typically <2 g/day) reduces fluid accumulation by limiting the osmotic driving force for ascites formation. This in turn reduces the volume of ascitic fluid available to enter the pleural cavity.
2. Diuretics
Diuretics reduce ascites volume and therefore the source of pleural fluid. The same agents used for ascites management are used — spironolactone (aldosterone antagonist) combined with furosemide (loop diuretic). Hepatic hydrothorax is treated simultaneously with the underlying ascites.
3. Therapeutic Thoracentesis
Pleural aspiration provides rapid symptomatic relief of dyspnoea by removing accumulated fluid. However, it does not treat the underlying cause — the diaphragmatic defects remain open and fluid will re-accumulate from the peritoneal cavity. Repeated thoracentesis is often needed but is not a definitive treatment.
Thoracentesis treats the symptom. It does not treat the cause. Fluid will return as long as portal hypertension drives ascites formation and the diaphragmatic defects remain patent.
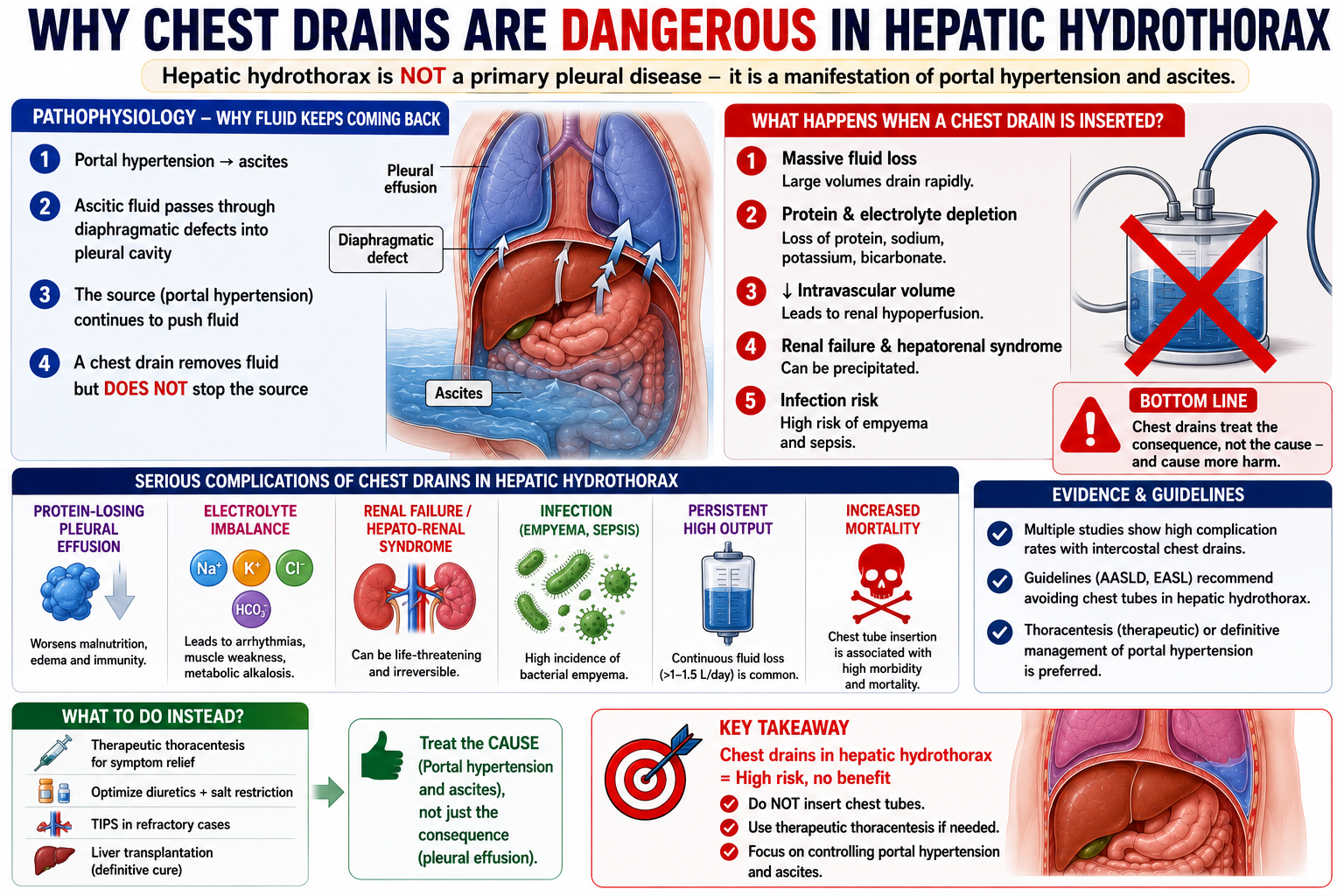
Why Chest Drains Are Dangerous in Hepatic Hydrothorax
This is one of the most high-yield exam points about hepatic hydrothorax. Students often assume that the logical management of a large pleural effusion is a chest drain — but in hepatic hydrothorax, routine intercostal chest tube placement is generally avoided because of its serious complications.
Because the diaphragmatic defects remain open, fluid from the peritoneal cavity continuously refills the chest drain output. The drain effectively places a high-flow drain on the entire peritoneal fluid compartment, leading to rapid depletion of protein, albumin and electrolytes, and significantly increasing the risk of infection and renal failure.
Routine chest tube placement is generally avoided in hepatic hydrothorax. The combination of continuous drainage-related protein loss, electrolyte depletion, renal dysfunction and infection risk carries a high mortality in patients who already have decompensated cirrhosis.
TIPS for Hepatic Hydrothorax
TIPS (transjugular intrahepatic portosystemic shunt) is used for hepatic hydrothorax that is refractory to diuretic therapy and repeated thoracentesis.
Because hepatic hydrothorax is driven by portal hypertension generating ascites, reducing portal pressure directly addresses the source of the pleural fluid.
TIPS works for hepatic hydrothorax by the same mechanism as it works for refractory ascites — portal pressure reduction reduces ascites formation, which reduces the source of fluid entering the pleural cavity. However, TIPS carries encephalopathy risk — see Hepatic Encephalopathy Explained.
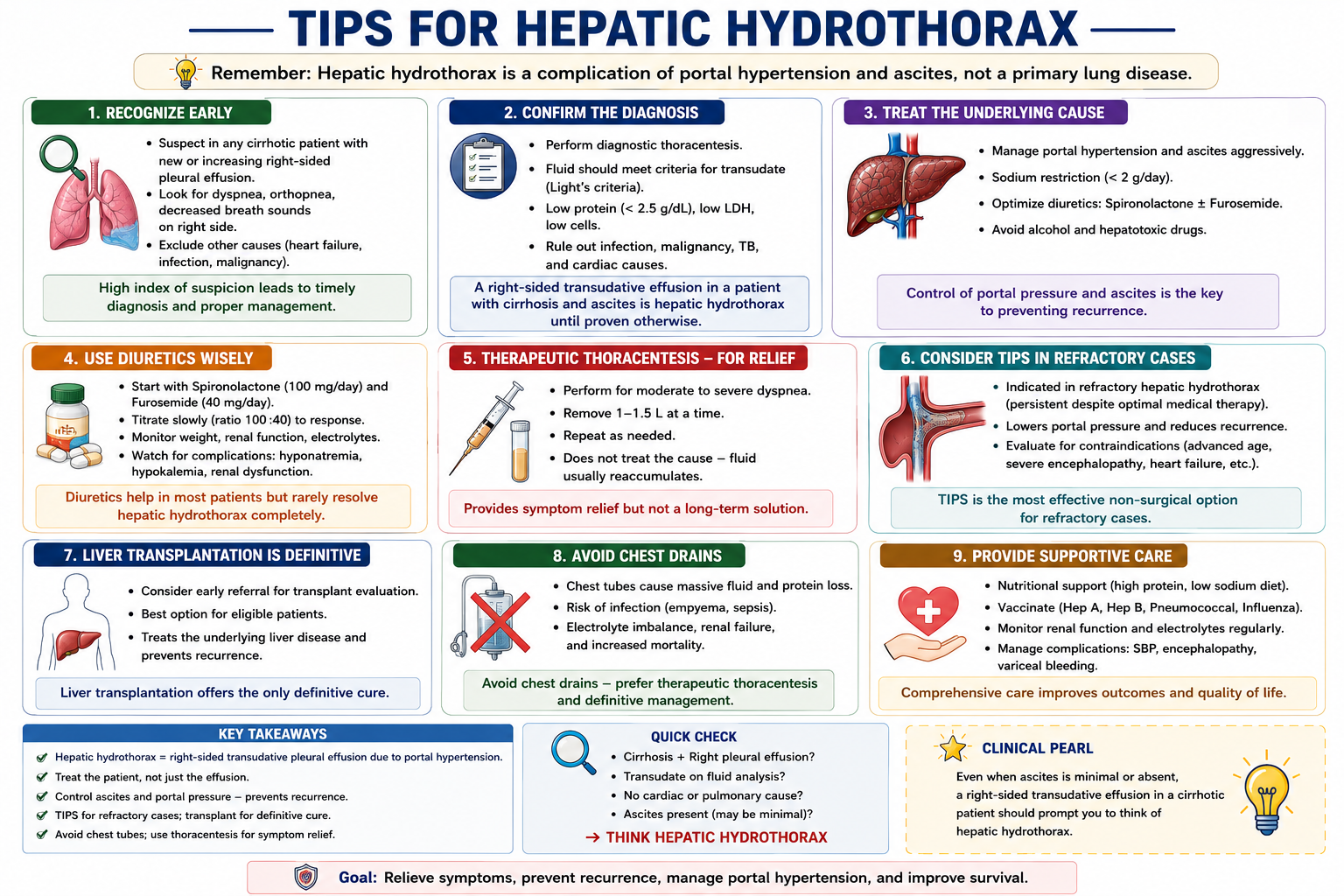
Liver Transplantation and Prognosis
Hepatic hydrothorax is a marker of decompensated cirrhosis. Its development indicates advanced portal hypertension with a liver that can no longer maintain fluid homeostasis. Prognosis without transplantation is poor.
Liver transplantation is the only definitive treatment for hepatic hydrothorax. By restoring normal hepatic function and eliminating portal hypertension, transplantation removes the haemodynamic driver of both ascites and hydrothorax. All patients with hepatic hydrothorax should be assessed for transplant suitability.
Any patient with refractory hepatic hydrothorax should be discussed early with a liver transplant centre. Repeated thoracentesis may provide temporary symptom relief, but recurrent hydrothorax usually reflects advanced decompensated liver disease.
Refractory or recurrent hepatic hydrothorax should trigger early hepatic hydrothorax transplant referral discussion, especially when repeated thoracentesis is required.
Hepatic hydrothorax contributes to Child-Pugh decompensation scoring. MELD score guides transplant prioritisation using objective laboratory values. Patients with refractory hydrothorax often qualify for exception points on transplant waiting lists.
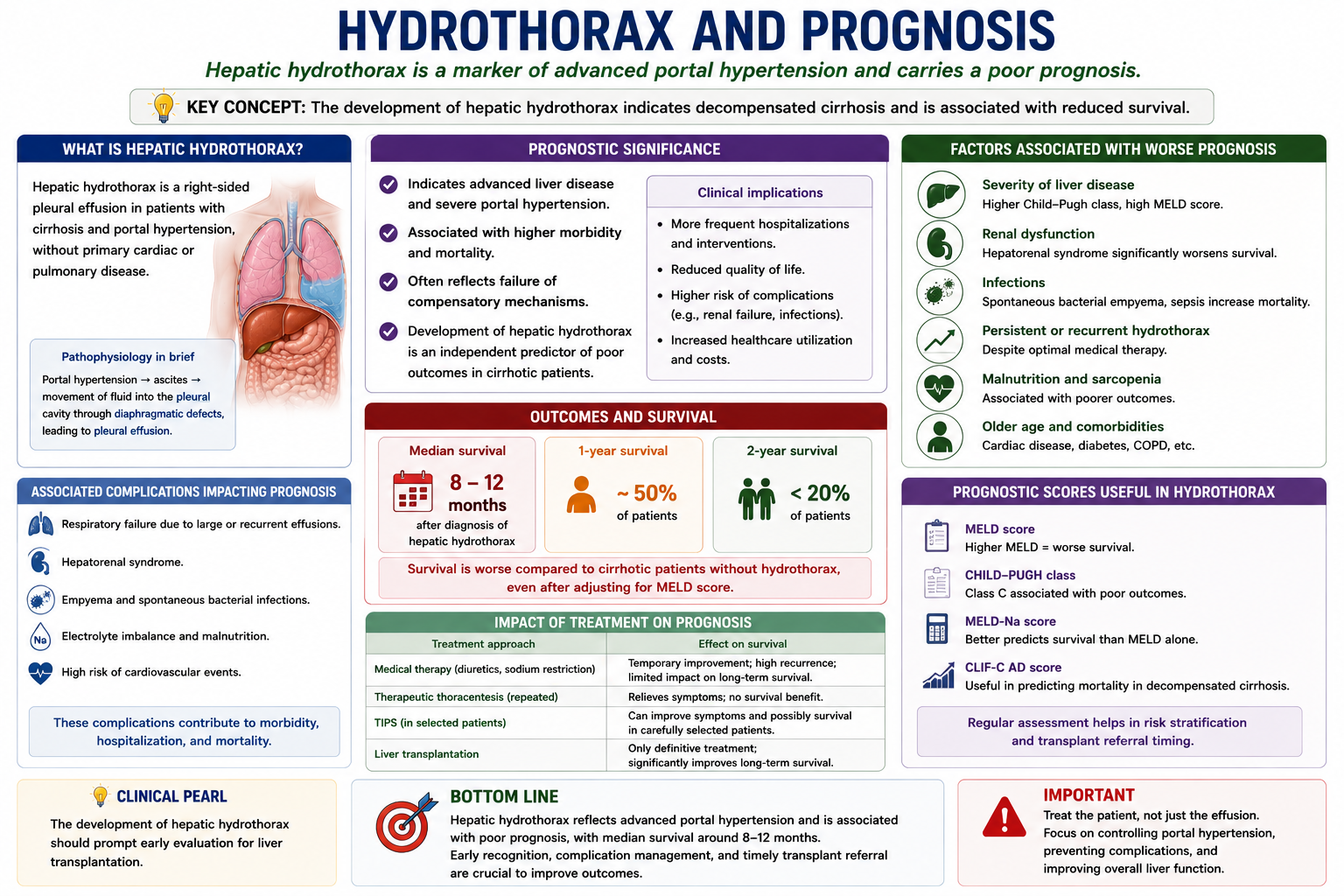
Complications
- Respiratory failure — large effusions cause lung compression and significant hypoxia
- Recurrent pleural effusions — fluid re-accumulates rapidly as long as the underlying portal hypertension persists
- Infection — spontaneous bacterial empyema — the most dangerous direct complication (see below)
- Renal dysfunction — from over-diuresis or chest drain complications
- Reduced quality of life — breathlessness, reduced exercise tolerance, frequent hospital admissions for thoracentesis
Spontaneous Bacterial Empyema
Spontaneous bacterial empyema (SBE) is a serious complication of hepatic hydrothorax in which the pleural fluid becomes infected without an obvious adjacent source such as pneumonia.
Spontaneous bacterial empyema is the pleural equivalent of SBP. Just as ascitic fluid can become infected in SBP without a contiguous source, pleural fluid in hepatic hydrothorax can become infected in the same way. The diagnostic criterion is PMN >250/mm³ in the pleural fluid, analogous to the ascitic fluid PMN threshold in SBP.
SBE is diagnosed by pleural fluid analysis showing >250 polymorphonuclear leucocytes/mm³ or a positive culture. It should be suspected in any patient with hepatic hydrothorax who develops fever, worsening breathlessness or clinical deterioration. It is treated with antibiotics (similar organisms to SBP — Gram-negative enteric bacteria are most common) and albumin infusion.
High-Yield Exam Pearls
Hepatic hydrothorax = extension of ascites into the chest
Mechanism: ascites → diaphragmatic defects → negative intrathoracic pressure → pleural cavity
Usually right-sided (~85%) — thinner diaphragm, more defects, liver proximity
Can occur without obvious ascites — fluid transfers faster than it accumulates
Pleural fluid: transudate (low protein, low LDH)
Chest drains: generally avoided — protein loss, renal failure, infection
TIPS: reduces portal pressure → reduces ascites → improves hydrothorax
Spontaneous bacterial empyema = SBP equivalent in the chest
Hydrothorax = decompensated cirrhosis → assess for transplant
- Not a lung disease — hepatic hydrothorax originates in the abdomen, not the chest. Target portal hypertension, not the pleura.
- Usually right-sided — the right hemidiaphragm is thinner and has more defects; the liver lies beneath it.
- No obvious ascites ≠ no hydrothorax — rapid fluid transfer through defects can deplete abdominal fluid while filling the chest.
- Transudate — the pleural fluid is transudative because it is essentially ascitic fluid. Exudate suggests infection (spontaneous bacterial empyema).
- Chest drains are dangerous — continuous drainage causes protein loss, electrolyte depletion, renal failure and infection. Avoid routine chest tube placement.
- TIPS treats the cause — by reducing portal pressure and ascites formation, TIPS reduces the source of pleural fluid.
- SBE = SBP of the chest — spontaneous bacterial empyema is the pleural equivalent of SBP, with PMN >250/mm³ as the diagnostic threshold.
- Transplant is definitive — hepatic hydrothorax indicates decompensated cirrhosis; all patients should be assessed for transplant suitability.
Key Takeaways
- Hepatic hydrothorax is a pleural effusion caused by portal hypertension and cirrhosis, not by primary cardiac or pulmonary disease
- Mechanism: ascitic fluid passes through small diaphragmatic defects driven by negative intrathoracic pressure
- Usually right-sided (~85%) — the right hemidiaphragm is thinner with more defects; the liver lies directly beneath it
- Can occur with little or no visible ascites — rapid fluid transfer depletes abdominal fluid as fast as it forms
- Pleural fluid is transudative — low protein and low LDH, resembling ascitic fluid
- Diagnosis: cirrhosis + right pleural effusion + transudative fluid + exclusion of cardiac/pulmonary cause
- Management stepwise: salt restriction → diuretics → therapeutic thoracentesis → TIPS → liver transplantation
- Chest drains are generally avoided — continuous drainage causes protein loss, electrolyte depletion, renal failure and infection
- TIPS reduces portal pressure → reduces ascites → reduces pleural fluid source → improves hydrothorax
- Spontaneous bacterial empyema is the pleural equivalent of SBP — diagnosed by PMN >250/mm³ in pleural fluid
- Hepatic hydrothorax signals decompensated cirrhosis and increased mortality — all patients need transplant assessment
Frequently Asked Questions
One-Minute Hepatic Hydrothorax Revision
Hepatic hydrothorax is ascites that has escaped into the chest. Remember the triad: cirrhosis + right-sided transudative pleural effusion + no primary cardiac or pulmonary cause. Treat the portal hypertension and ascites — not just the chest.
References
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460.
- Cardenas A, Kelleher T, Chopra S. Review article: hepatic hydrothorax. Aliment Pharmacol Ther. 2004;20(3):271–279.
- Falchuk KR, Jacoby I, Colucci WS, Rybak ME. Tetracycline-induced pleural symphysis for refractory hepatic hydrothorax. Ann Intern Med. 1977;86(5):641–642.
- Huang PM, Chang YL, Yang CY, Lee YC. The morphology of diaphragmatic defects in hepatic hydrothorax: thoracoscopic finding. J Thorac Cardiovasc Surg. 2005;130(1):141–145.
- Garcia N Jr, Mihas AA. Hepatic hydrothorax: pathophysiology, diagnosis, and management. J Clin Gastroenterol. 2004;38(1):52–58.
- Xiol X, Castellote J, Baliellas C, et al. Spontaneous bacterial pleural empyema in cirrhotic patients: analysis of eleven cases. Hepatology. 1990;11(3):365–370.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist hepatological input when managing patients.
- Where Hydrothorax Fits
- What Is Hepatic Hydrothorax?
- Pathophysiology
- Diaphragmatic Defects
- Why Right-Sided?
- Why Little Ascites?
- Clinical Presentation
- Pleural Fluid Findings
- Differential Diagnosis
- Diagnosis
- Management
- Why Chest Drains Are Dangerous
- TIPS for Hydrothorax
- Prognosis & Transplantation
- Complications
- Spontaneous Bacterial Empyema
- Exam Pearls
- Key Takeaways
- FAQ
- One-Minute Revision
- References